
Divergent T-cells and forgetful B-cells
One protein to rule them all

As we build a foundation into certain subjects to further understand the deep changes SARS-CoV-2 brought and still brings, lingering questions remain. One of these questions, especially from a scientific curiosity perspective was “Why do the SARS-CoV-2 vaccines, with emphasis on the mRNA don’t produce long-lasting immunity ?”. In pursuing the answers, many hypotheses and ideas have been proposed, many of which I wrote myself.

Long ago, there were already signs many of the vaccinated failed to mount Memory B cells, even post-vaccination, and that other antibodies present in the body heavily affected immune memory formation. This was also the first sign of a shift in immunity, from your normal IgG’s to IgG4. Questions remain, plentiful the more you learn.
As written in recent articles, most of our defenses against SARS-CoV-2 are now T-cell based, not B-cell (B-cells = antibodies), immunology is highly complex but in simplistic terms:
B-Cells - Slower response time (3-5 days), mostly to limit the number of pathogens and reduce disease burden
T-cells - Faster (<2 days), mostly to control the severity of the disease/infection
Given that the government, pharmaceutical companies, and nudge units distorted decades of immunology to push the “antibodies are everything and forever” propaganda, I am always interested in B-cells and antibodies changes, effects…or loss.
As many of you may be aware, certain infections will give you a long, lasting immune response, some can last 10-20 years, tetanus vaccination even longer, and even influenza infections can provide lasting immunity towards that strain (it is one of the reasons the flu mutates so much).
Interestingly enough, among all the antigens they tested (S1, S2, RBD, NTD, NP, and S2P), S2P was the one with the strongest response followed by S1. S2P is the Spike with Proline mutations that are present in the mRNA vaccine. By doing thorough experiments with samples from vaccinated patients and taking into account breakthrough infections, with special attention, the cells could live outside the body (these types of cells can die very quickly when you try to do experiments) the authors found one of the potential reasons the antibody immunity doesn’t last long.
Besides the mutational burden, as how fast the virus mutates in the spots our antibodies “glue” to stop it, here they found simply put the vaccinated individuals in this study don’t develop Long-lasting Plasma cells in the Bone Marrow, only short-lived ones.
The argument here is that to develop Long-Lived Plasma cells (LLPC), antigen-secreting cells (such as B cells) need to go through complex, long changes until they reach a final maturation stage to become LLPC. This is a hard process on these cells and many die during it. It is believed that LLPC is derived directly from memory B cells, and as you probably saw at the very start of the article, the vaccine has difficulty eliciting these from the get-go.
Failure to imprint, therefore failure to create memory will inevitably fail to induce said LLPCs. Even after 33 months after the vaccine, these antigen-secreting cells are still excluded from the Bone Marrow LLPC. Even after breakthrough infections the body still fails to amount long-lasting immunity.
The author’s closing remarks are worth consideration especially the last paragraph, something a certain someone stated many, many years ago. That someone was Ralph Baric.

In simplistic terms, this explains why there is a huge discrepancy at different points in time in the pandemic between vaccinated X unvaccinated, viral loads, and viral spread, at least initially. It can also explain some viral rebound cases at the time. And given it is the weekend, your conspiracy for it will be, it is interesting that both MERS-CoV (which has a similar Furin Cleavage Site to SARS-CoV-2), and SARS-CoV-1 also induce short-lived antibodies.
As I usually do often these days, this is just a small glimpse of what is going on, the truth is much more complex and there are even more confounding factors affecting the formation of memory B cells and LLPCs. But it is a great piece of the puzzle. In summary, vaccinated B cells be link:

Given that I vehemently believe both are byproducts of long-term gain of function. Someone has been cooking for a long time. But not only of antibodies the immune system lives, so by fate or by chance, we have one exciting paper on T-Cells.
The spike-specific TCRβ repertoire shows distinct features in unvaccinated or vaccinated patients with SARS-CoV-2 infection

A lingering question has been if there are responses to T-Cell responses between vaccinated and unvaccinated if each group’s immune response has a preference for different “locations” in the Spike Protein, and the large variance between groups and even inside each group’s infection severity. Some studies indicated that a broader, more diverse repertoire of TCR leads to less severe disease, severe (hospitalized) cases will often have a less diverse repertoire.
A larger repertoire means your body recognizes more of the “Lego pieces” to deal with a pathogen. If it is too focused or less diverse, mutations and other variables inside the body can lead the pathogen to escape and cause a lot of inflammation and subsequently damage. Some of these TCRs are the ones responsible for eliciting a CD8+ T cell response, the response necessary for properly dealing with the virus early on.
Worth noting, since treatments will affect many of these variables and T-cell responses, that the samples here were collected before any treatment if the patient had one to begin with. NV = Non-vaccinated, V = Vaccinated (With Pfizer’s mRNA vaccine).
Their first step was to test if stimulating PBMC (Peripheral Blood Mononuclear Cells, different types of cells that including T cells) with S-peptides, and found that exposure to the S-peptides did increase the response, and this was similar in both vaccinated and unvaccinated.
Next by using advanced modeling with an algorithm named GLIPH2, the authors found that both groups NV and V shared TCRβ sequences, meaning that both groups target similar places when compared to a large public database. The researchers identified a total of 1171 unique TCRβ sequences associated with 149 different peptides, which are small pieces of proteins that TCRs recognize. Among these, 130 epitopes were common between both V and NV groups, suggesting that there are common targets that T cells from both vaccinated and non-vaccinated individuals are recognizing.
So far, this entails “Vaccinated and unvaccinated share many lego pieces that their T cells will use to deal with the virus and create a proper immune response”. And the following is the reason I decided to cover this paper. Specifically the next paragraph and image, directly from the paper.
Among the 130 shared peptides, TCRβ clonotypes associated with S regions S135-177, S264-276, S319-350 and S448-472 were significantly more abundant in the post-stimulation repertoires of V group than the NV group (Fig. 5a, b and Table 4). Conversely, TCRβ clonotypes associated with protein region S673-699 was significantly more abundant in the post-stimulation repertoires of NV group than the V group (Fig. 5a, b and Table 4). Moreover, the S645-645 and S751-760 peptides were exclusively associated with TCRβ clonotypes in the NV group, while S778-789, S863-871 and S1260-1269 peptides were exclusively associated with TCRβ clonotypes in the V group (Fig. 5a, b and Table 4). These results indicate a distinct profile of TCR epitope specificity between the N and NV COVID-19 groups following infection with SARS-CoV-2.
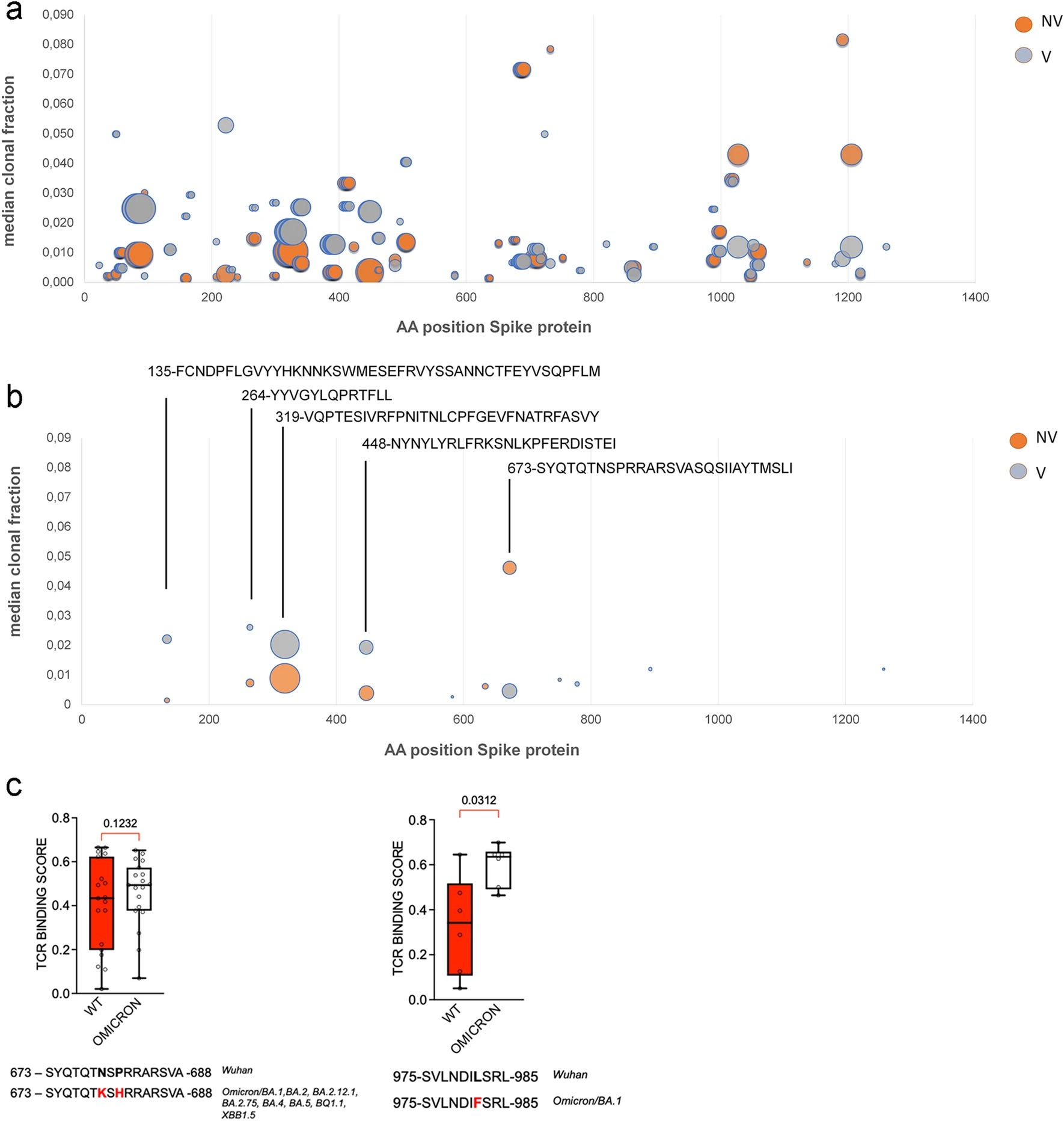
One of my primary and largest interests is superantigens, together with toxins. That PRRAR sequence is all-in-one. All the letters in the “C” section in the image form a multifunctional protein. It is the cleavage site, it also mimics one of the most powerful toxins known to science (SEB), and it also can mimic Neisseria Meningitis (another powerful toxin). Ironically it also mimics a part of HIV (GP120).
Also as a matter of interest, there is another HIV insert in the sequences above, the “135” one, HKNNKS. Here is where things get complicated. There is a measurable difference in how the T-cell responses between unvaccinated and vaccinated, with each group of immune cells targeting specific sequences.
The unvaccinated will often target the superantigenic region, while the vaccinated target other regions, there is an overlap, but there are distinct T-cell responses between the two. While I don’t think the safety trade-off and the many unknowns are worth the protection, it would explain why vaccinated children suffer less from MIS-C.
But if you read the excerpt above, you read that the vaccinated respond to places the unvaccinated don’t respond that strongly. Here is where things get rather interesting. The majority of those sequences are the pockets Lipid A and LPS (Endotoxin) have more binding strength.

This adds an incredible layer of complexity to everything discussed here and in dozens of older articles, because exposure and response to superantigens and toxins modulate your entire immune response, not only towards that specific pathogen, but it will affect, quite literally, your immune response towards any subsequent infection.
Among many variables responsible for these distinct differences, given the evidence and literature, I infer the major contributor to this difference is the proline modifications added in the vaccine, that stabilize the Spike, and make it easier for endotoxin to bind to the Spike, among other changes.
And this opens up a whole can of worms. While I could digress into plentiful of tangents I will end this in topic. Care to guess what happens to your B Cells when exposed to LPS or Lipid A (or a chimeric protein containing these molecules) ?
B cells will develop accelerated division, but later experience a decline, resulting in fewer cells reaching the aforementioned later stages of development (becoming Plasma Cells).
Everything discussed here and the related articles will be important later on, after all, Omicron still does all this, just not as hyper-aggressively as Wuhan Original (trademark pending).


If you recall, SARS-CoV-2 antibodies can help cause Dengue ADE -> https://hiddencomplexity.substack.com/p/sars-cov-2-antibodies-can-help-cause
With a million cases of dengue so far this year, Brazil is in a state of emergency
https://www.npr.org/sections/goatsandsoda/2024/03/04/1235795657/dengue-brazil-state-of-emergency-vaccine
Glad I never had Dengue in my life, don't want to start now lmao.
Professor - Your excellence continues. Long term LLPC exclusion is very problematic, and a post LPS exposure decline in B cell population, even more so. In that vein, or marrow of the matter, consider that spike utilizes both LPS & HMGB1 as gene delivery agents Mr. Mulder