First and foremost, all this research in regard to immune response and pathways wouldn’t be possible without someone who wishes to remain anonymous. That person deserves more of the credit than I do.
After months of seriously looking into the virus and viral infections from a metabolic perspective and plenty of interdisciplinary research, I held the opinion that this was a metabolic disease and was inducing a specific and nasty form of cell death. It’s called Ferroptosis, and it’s deeply connected to a lot of diseases.
I was still trying to pinpoint what exactly was causing the systemic ferroptosis, when the anonymous person contacted me. Sometimes parts of the truth are in your face, and you just don’t see it.
The most important lesson I learned last year was “Always look upstream” (in physiological, biological, and cell pathways, but now I apply it to my entire mental framework). In every virus post I wrote, I left clues and breadcrumbs.
As previously discussed, viruses and vaccines induce large amounts of Interferon Gamma, which in turn makes your cells produce variable amounts of Interleukin-12. Enough IL-12, IL-23, add to the mix aberrant IL-17 and your road will lead you to Rome.
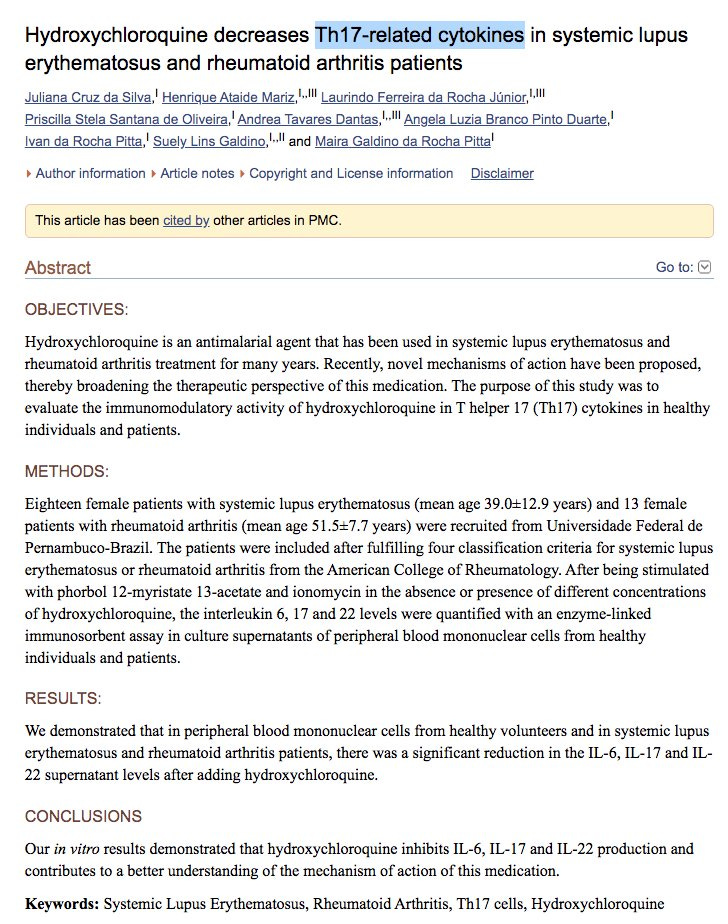
Side note, and a later addition. This paper show links between ferroptosis and shifting your immune response towards Th17, using Psoriasis as a model, a common model for studying, among other things, the pathological role of Th17 cells. Keratinocytes have a high expression of ACE2.
Ferroptosis is recognized as more immunogenic than apoptosis. This is because it not only promotes cell death but also potentiates a series of inflammatory reactions through the release of DAMPs and alarmins [24, 25]. Currently, ferroptosis inhibitors have been demonstrated to perform anti-inflammatory effects in experimental models of acute kidney injury, intracerebral hemorrhage, and neurodegenerative diseases [20, 26, 27].
Immune cells and the “IL-17 axis” are implicated in the pathogenic mechanisms of psoriasis [4]. Keratinocytes were previously recognized as initiators in the inflammatory process. They play an essential role in the amplification of the inflammatory cascade, through the secretion of chemokines and cytokines [5,6,7].
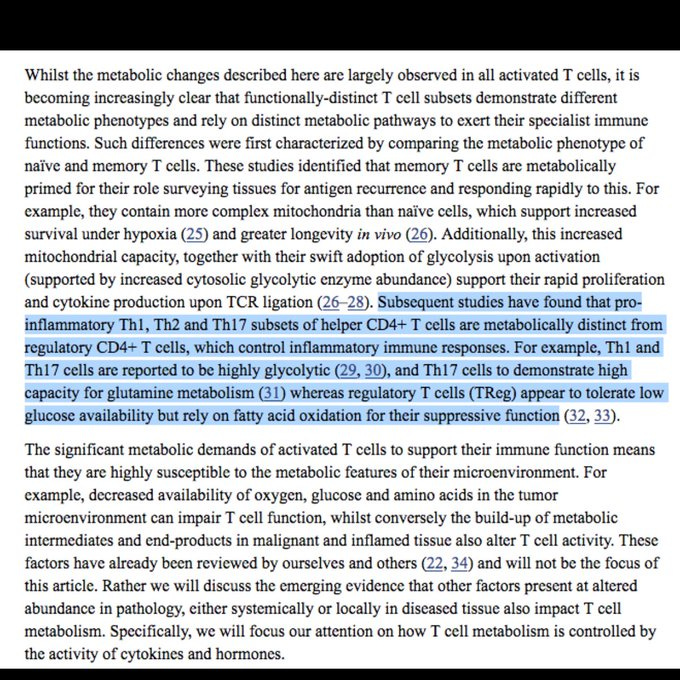
In our research, a positive correlation was observed between lipid oxidation and the Th22/Th17 pathway at a single-cell level.
Enough of said cytokines, enough inflammation, or immune reaction, you stop Th1 differentiation and go to Th17. So, what is Th17 ? Th17 cells play a role in host defense against extracellular pathogens, particularly at the mucosal and epithelial barriers, but aberrant activation is linked to the pathogenesis of various autoimmune diseases.
The roads to Rome. KREGGs pathway.
While among the first few, there was someone who saw it before any other scientist in the planet. Peter Hotez, yes, that Peter Hotez. Pro-vaccine Peter.
Increasing evidence points to host Th17 inflammatory responses as contributing to the severe lung pathology and mortality of lower respiratory tract infections from coronaviruses. This includes host inflammatory and cytokine responses to COVID-19 caused by the SARS-2 coronavirus (SARS CoV2). From studies conducted in laboratory animals, there are additional concerns about immune enhancement and the role of potential host immunopathology resulting from experimental human COVID-19 vaccines Th17 cells differentiate in part through the actions of IL-6 [7], and IL-6 has been shown to have an important role in the lung pathology associated with SARS infection
Patients display significant increases of proinflammatory or anti-inflammatory cytokines, including T helper type-1 and type-2 cytokines, chemokines and galectins; their lymphocytes produce more tumor necrosis factor (TNF), interferon-γ, interleukin (IL)-2 and IL-17
The massive production and release of cytokines is very similar to what occurs during polyclonal, superantigen-driven, T-cell activation48. A fourfold increase of the levels of a TH1 molecule such as IFN-γ was indeed observed in plasma from COVID-19 patients as compared with controls. IFN-γ activates macrophages, which produce proinflammatory cytokines, which then overwhelm the system. When cells from patients were stimulated with anti-CD3/28, an increased number of CD4+ T cells producing IFN-γ, TNF, IL-17, and IL-2 was observed as compared with healthy controls
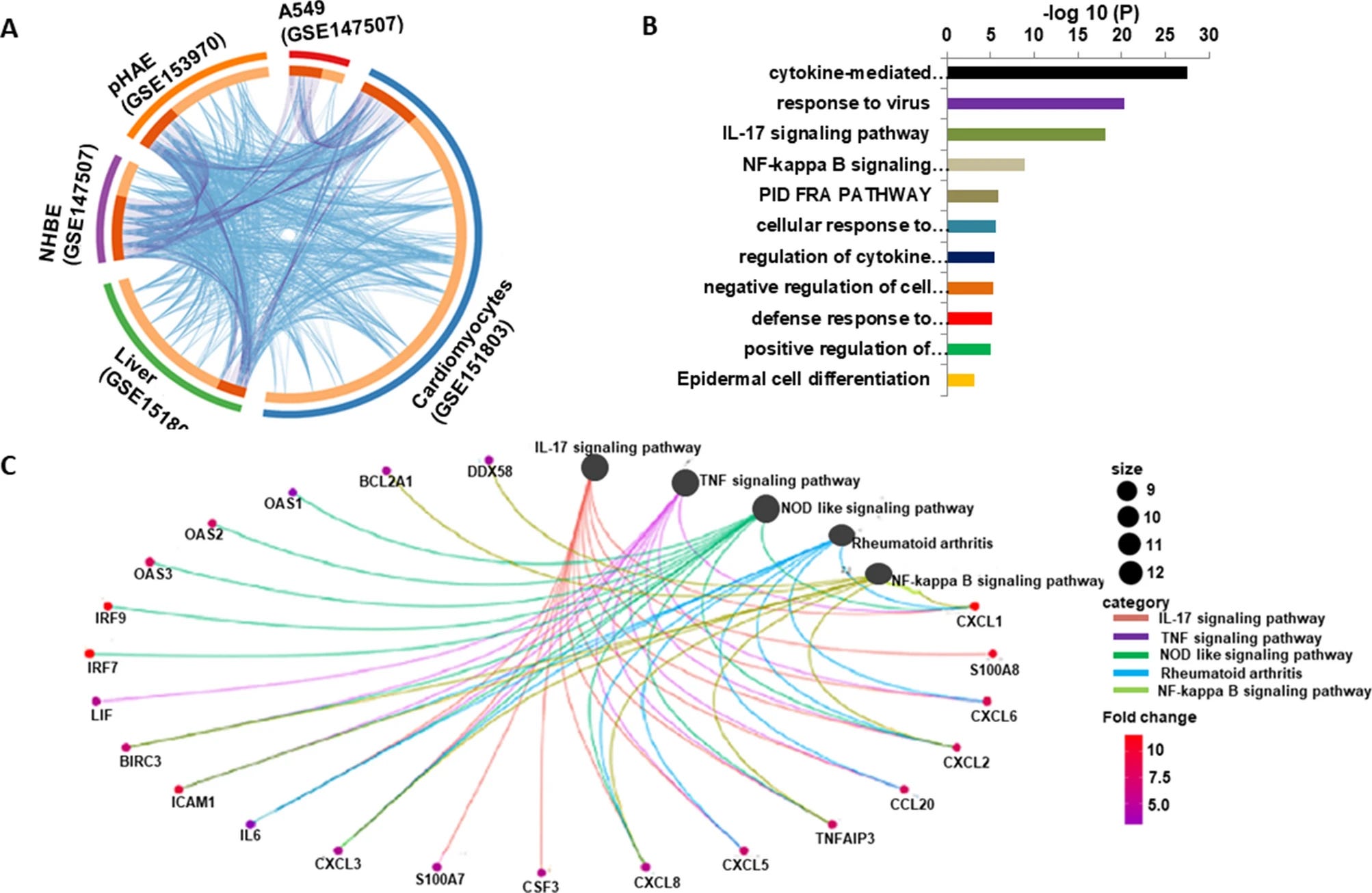
Genes such as interleukin (IL)-6, CXCL8, CCL20, CXCL1 and CXCL3 were upregulated, which in particular regulate the cytokine storm and IL-17 signaling pathway. Of note, SARS-CoV-2 infection strongly activated IL-17 signaling pathway compared with other respiratory viruses.
Taken together, our comprehensive data analysis showed that SARS-CoV-2 initiated a distinct IL-17-driven inflammatory response irrespective of the cells used in various studies.
There are numerous papers showing that the virus induces high levels of IFN-gamma, IL-17 and other cytokines and effectors to shift your immune response towards Th17. All my posts were building to this. That the virus (to various extents, multiple variables), and the jab, by design, is inducing a strong Th17 response very early on.
There is a literal dozen, perhaps more, different pathways that lead to similar outcomes or help to feed each other and disease. I will try to keep it shorter and simple. As previously covered in The Toll of TLR, the vaccines modulate your Toll Like Receptors, so they can enter your cells and deliver their mRNA payload. There is no off-button in biology, and when the immune responses kick in…
Moreover, mRNA vaccines, like BCG or diphtheria, may cause a significant increase in IL‐6 production and recruitment of Th17 cells, which play an important role in pathomechanism of psoriasis.
In line with these transcriptional findings, robust antigen-specific polyfunctional Th1 and Th17 responses were observed within CD4+ T cells in all vaccinated individuals. Although CD8+ T cell responses were weak and highly variable
…strongly suggesting that mRNA vaccines promote the development of a Th1/Th17 response. No significant production of immune mediators was noted by CD8+ T cells, except for perforin and modest levels of IFN-γ…
…Our single-cell analyses suggest an expansion of activated CD4+ T cells (CD38+HLA-DR+) that are skewed toward a Th1 and Th17 phenotype…
…Cytokine analysis of stimulated CD4+ T cells also suggested a robust Th1/Th17 response and a lack of Th2 response to spike peptides. In contrast, cytokine-producing CD8+ T cells were observed in only 2 of the 4 individuals, and effector responses to spike peptides were weak, suggesting a delay in development of effector CD8+ T cell response…
This entire paper makes the point of most of my posts here. Skewed immune response towards Th1, differentiation to Th17, a weak response from CD8 cells, which authors argue is delayed, but it is basically nonexistent, production of IFN-gamma.
Metabolism plays a large role in all of this, so I wasn’t so far off.
The vaccines also immune suppress you, both by modulating your TLR response, by the design itself to severely skew towards CD4, and the use of the entire spike protein, leading to the activation of latent and chronic infections. Which…
The involvement of TLR9 in the EBV DNA-triggered induction of IL-17A suggests therapeutic targeting of this endosomal receptor in EBV positive subjects with an autoimmune flare-up or possibly for prophylactic purposes.
The state of immunosuppression many find themselves in leads to a transient CVID (Reverse AIDS for the stickiness of the meme).
Cytokine profiles provided insight into activation of Th1 and Th17 pathways and indicate a possible role for chronic inflammation and exhaustion in immune dysregulation. These findings serve as a first step towards the development of biomarkers for immune dysregulation in CVID.
…and the T-helper (Th) serum cytokine profile observed in immune dysregulation in CVID is mostly found to be Th-1 driven…
…In addition, cytokines and chemokines associated with Th17 activation were upregulated, including IL17A (adj. p = 0.011, FC = 2.44), IL12B (also known as IL12p40, a subunit of IL12 and IL23; adj. p = 0.044, FC = 1.64) and mucosal tissue homing chemokine CCL20 (adj. p = 0.043, FC = 2.39). IL-6 production, which would be consistent with activated Th17 cells, was upregulated…
Stattic, rescued these effects in vitro and in vivo. Moreover, survival analysis showed that patients with low CD8 and CXCR3 expression and high IL-17A levels had significantly worse prognosis.
Our studies establish a crucial role for Gpx4 in protecting activated Treg cells from lipid peroxidation and ferroptosis and offer a potential therapeutic strategy to improve cancer treatment.
Before diving deeper into Th17, months ago I raised a question.
We found substantially higher frequencies of M. tuberculosis–specific effector and memory CD4+ and CD8+ T cells producing IFN-γ in the airways compared with peripheral blood, and these frequencies were maintained throughout the study period. Moreover, M. tuberculosis–specific IL-17+ and IL-17+IFN-γ+ double-positive T cells were present in the airways but were largely absent in the periphery, suggesting that balanced mucosal Th1/Th17 responses are associated with LTBI.
Th17 cells play vital role during pathogenesis of leprosy reactions. Previously, we have reported that IL-23 is involved in Th17 cells differentiation. Subsequently, our group also showed that IL-6 induces Th17 cell differentiation along with TGF-β in leprosy reactions
Th17 cells are important players in host defense against pathogens such as Staphylococcus aureus, Candida albicans, and Bacillus anthracis
This is the first study describing that innate and Th1/Th17 adaptive immunity play a crucial role in BB disease. Furthermore, innate mediators are particularly important in acute BB disease, and TNF-α is associated with evolution of BB symptoms. (Disease similar to Borrelia burgdorferi)
Main Th17 cell effector cytokines were upregulated in laboratory-confirmed A(H3N2) influenza and PIV. Excessive amounts of Th17 cytokines may be implicated in the pathogenesis and immune control of acute influenza and PIV infection in humans and may predict the severity of disease.
There is also extensive literature on the immune suppressive effects of that list of diseases. My point with the question was pretty straightforward, and this is simplifying it. Using multiple mechanisms and pathways, the vaccine will elicit a strong Th17.
Notably, a motif of ∼20 amino acids enclosing this insert unique to SARS-CoV-2 has sequence and structure features highly similar to those of the toxin SEB
We established that S. aureus bloodstream infection severity is mediated by CD4+ T cells and interferon-gamma (IFNγ) is produced to very high levels during infection in a SAg-dependent manner. Bacterial burden and disease severity were reduced by antibody blocking of IFNγ, phenocopying isogenic SAg deletion mutant strains.
These results suggest that superantigenic S. aureus are particularly efficient in stimulating IL-17 production and that the cytokine is produced from memory T cells.
Here is a decent article on what are superantigens.
At this point, my argument, and the evidence itself, is clear. The virus to a minor level (populational), using different mechanisms, and the vaccine using others, induce similar immune responses, and similar pathological effects, mostly because of the S (spike) protein.
The mRNA is faster and worse than the virus on inducing its pathological effects because you are producing almost a trillion units of Spike proteins, which in turn are severe inflammatory, allergenic, and with antigens from diseases that can all end up in a dominant immune response, you do not want to give the circumstances.
I named this whole pathway “Hermesian Pathological Signaling”. From Hermes, the Greek god, among other aspects, speed. Another reason to call it Reverse AIDS, is from this paper (good read btw).
I repeat the question I made once, given what you’ve read so far, are breakthrough infections harmless ?
You don’t need a severe case of Covid-19 for the stimulation of the necessary cytokines and everything else to produce enough quantities of specific cells and their proteins to keep shifting and causing transient immune dysfunction. The vaccinated encounter themselves in a perpetual state of this.
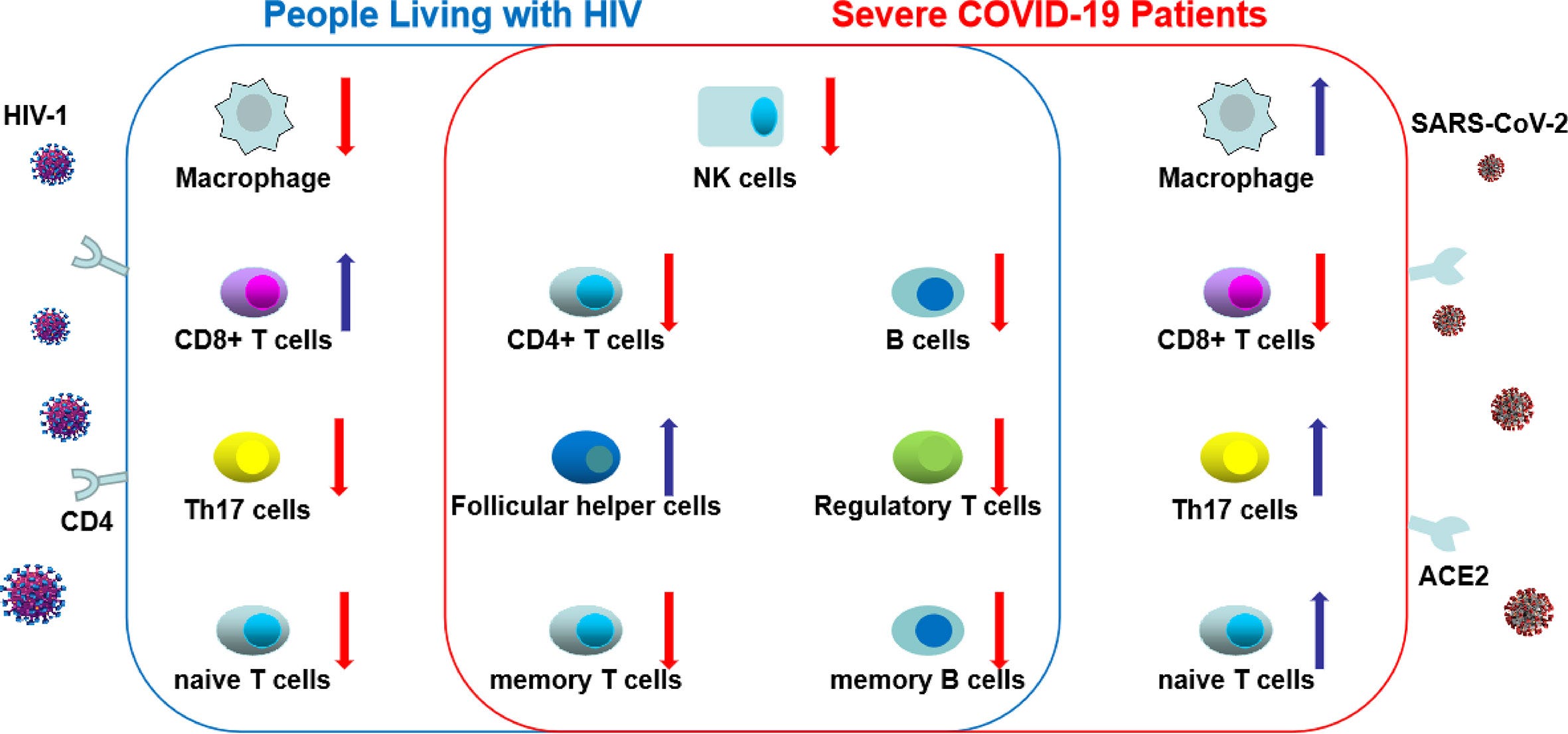
Another reason to compare the two diseases is for their uncanny similarity in many immune effects and suppression.
Recent studies have shown that the tryptophan-kynurenine pathway (Trp-Kyn) is altered in COVID-19 patients. A study conducted by Thomas et al. analyzed serum metabolites of COVID-19 patients and found that tryptophan (Trp) levels were reduced, and L-kynurenine (Kyn) was elevated [5]
A study performed by Fraser et al. reported similar findings (elevated levels of Kyn in COVID-19 patients) [6]. Another study reported that Kyn levels were elevated, along with kynurenic acid (Kyn-A) and quinolinic acid (QA) in the serum of COVID-19 patients [7].
Several studies also reported elevated levels of genes involved in tryptophan metabolic pathways [11, 12]. The study conducted by Policard et al. reported that indoleamine-pyrrole 2,3-dioxygenase (IDO-1) is significantly upregulated in COVID-19 patients [11]
One-sentence summary The current meta-analysis study revealed a significant increase in peripheral blood IDO activity and kynurenine levels and a significant reduction in tryptophan in COVID-19 versus controls and in severe/critical COVID-19 versus mild/moderate COVID-19.
Blockade of gp120/CD4 interactions with anti-CD4 Ab inhibited HIV-mediated IDO induction. Thus, induction of IDO in pDCs by HIV may contribute to the T-cell functional impairment observed in HIV/AIDS by a non–interferon-dependent mechanism.
his review article will briefly summarize the evidence linking Th17 cells to brain diseases associated with cognitive impairment, including multiple sclerosis (MS), ischemic brain injury and Alzheimer’s disease (AD). We will also investigate the mechanisms by which these cells enter the brain and induce brain damage, including direct effects of IL-17 on brain cells and indirect effects mediated through disruption of the blood-brain barrier (BBB), neurovascular dysfunction, and gut-brain axis.
Dysregulated IL-17 production and signaling have been involved in different autoimmune diseases (Gaffen et al., 2014), but the mechanisms are not yet fully understood. Recently, several pieces of evidence have revealed that blocking the activity of IL-12 and IL-23, IL-1, or IL-6, which are critical for Th17 cell differentiation and propagation, is effective for the treatment of inflammatory diseases, such as MS, IBDs, RA, and psoriasis.
There are recent evidence supporting a definitive role of Th17 cells in the etiology of type 1 diabetes (T1D). In addition, IL-17 has been shown to play a crucial role in inflammation, insulin resistance, and type 2 diabetes (T2D).
The predominant inflammatory cells were CD4+ lymphocytic aggregates (77% of cases), combined with co-staining of CD4 IL and 17A/F in 44–48% of all cases, suggesting a Th17-mediated inflammatory process.
(It’s my opinion this is mediated by the massive microbiome change PPIs cause btw)
In conclusion, SARS-CoV-2 vaccine-associated SAT is a novel entity, which shares epidemiological and clinical characteristics with the classic post-viral SAT but could be triggered by peculiar mechanisms. It is possible that patients with a previous history of thyroid disease may be more prone to develop SAT after mRNA vaccines,
The reader could to a test, every time you see a paper of an adverse event that you didn’t hear before, search that pathology th17. You will be surprised. Reductive, yes, but it’s for simplicity's sake and to make research far easier for the layperson.
It’s unusual for me, but I will leave the reader with a working hypothesis. What happens when you keep vaccinating people with dysfunctional immune systems, they keep getting infected, and keep developing secondary infections ? Or do they stop getting the vaccine, and their dysfunctional immune system recovers ?
immune reconstitution inflammatory syndrome - IRIS, it’s also present when the patient recovers from immune suppressive states
IRIS may occur at any stage in the progression of immunodeficiency and manifests with weakened immune system. IRIS is associated with various inflammatory processes as the outcome of immunological reaction against a variety of opportunistic infections (OIs).
I hope messing with Toll-Like Receptor, and causing a state of immune suppression for weeks doesn’t make you more susceptible to all types of secondary infections.
And for last, a little something.
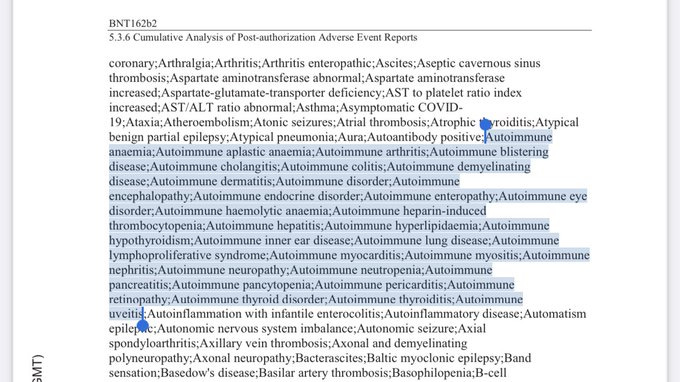
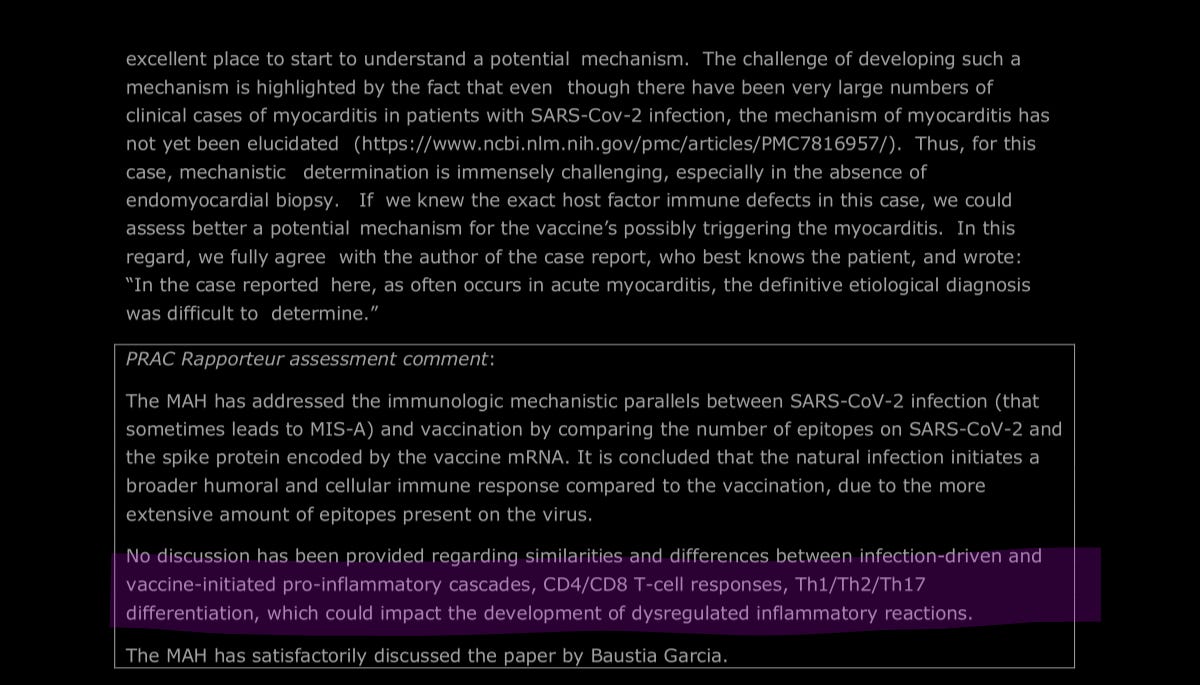
Post-publication edit. I hate losing this document and screenshot and just remembered it today, here is the link for the EMA document.
MAH - MODERNA
If you enjoy or take value from independent interdisciplinary analysis, consider becoming a free or paying subscriber, shifting to doing it full time and with higher quality. Sharing also helps me tremendously. Appreciate all supporters.
Hi Jonathan. I have two young adult children. My son got the shot, my daughter did not. My daughter and I both had the Beta Covid. We are not getting the shot. I am very worried about my son who is 26 and a smart robotics engineer. Lots of smart lovely people have been fooled with their trust in government.
I try hard to understand your very amazing in-depth posts. Thank you for them. I just do not understand.
I want to know if my son will be OK or not? Is there anything one can do after two shots of this Pfizer? I have begged him to not get boosters.
Please is there a straight forward answer?
Sorry for not having the mental gymnastics ability to make sense out of your info. Explain it to me like you would a child - and the straight goods. I need to know the truth and accept it and be as much of a support to the people around me who it seems will become sick.
I appreciate the time and effort you must put in here to works like this. Can you explain in a few sentences to the unscientific mind, like you would to a five year old or golden retriever, what is happening with the vax spike protein in the body, if it goes to all organs or just some, and why some people have adverse reactions, some die and it appears nothing happens at all in others? Are some doses saline?











Hi Jonathan. I have two young adult children. My son got the shot, my daughter did not. My daughter and I both had the Beta Covid. We are not getting the shot. I am very worried about my son who is 26 and a smart robotics engineer. Lots of smart lovely people have been fooled with their trust in government.
I try hard to understand your very amazing in-depth posts. Thank you for them. I just do not understand.
I want to know if my son will be OK or not? Is there anything one can do after two shots of this Pfizer? I have begged him to not get boosters.
Please is there a straight forward answer?
Sorry for not having the mental gymnastics ability to make sense out of your info. Explain it to me like you would a child - and the straight goods. I need to know the truth and accept it and be as much of a support to the people around me who it seems will become sick.
I appreciate the time and effort you must put in here to works like this. Can you explain in a few sentences to the unscientific mind, like you would to a five year old or golden retriever, what is happening with the vax spike protein in the body, if it goes to all organs or just some, and why some people have adverse reactions, some die and it appears nothing happens at all in others? Are some doses saline?