
Failing Memory B cells from mRNA
It ain't rocket science bruh.

I thought of writing about the polio situation but I rather write this one, quicker, I won’t break down the entire paper. This is in line with other papers I covered so far here.

Memory B cell responses to Omicron subvariants after SARS-CoV-2 mRNA breakthrough 2 infection
The entire paper is rather complex, and the writing style doesn’t make it easier to understand too. But in line with many other papers measuring other markers for the immune response, and in this case, they are measuring memory antibodies, basically how effective your immune memory works against different infections.
The findings in the image (which we will lightly break down below) are straightforward to understand if simplified. In very simplified terms:
Delta breakthrough infection equals the third dose of mRNA vaccine
Another breakthrough infection with BA. 1 increases the plasma and memory
responses for that variant
A fourth exposure didn’t

Per my gross simplification, a Delta breakthrough infection is as effective as a “booster” dose and boosts strain-specific responses, so if you had a breakthrough infection with it there was absolutely 0 need to get a booster, but in contrast, Omicron breakthrough infection elicits a far weaker response and breadth of immune memory.
In line with a paper I wrote about and retweet often, variant-specific mRNA vaccines might “boost” the usual markers they use to sell the short-lived vaccine efficacy, but it is not better than using the original Wuhan Spike-centric mRNA vaccine. Not only in line with findings from other researchers but in line with mine and other observations, since the Wuhan Strain was, quite literally, akin to a vaccine for many different coronaviruses. I am not arguing the “LAV” scenario, but talking from an immunogenic (capacity to generate an immune response) standpoint.
Worth praise to write the purple highlighted part in a scientific paper these days. “Designing vaccines with a broader general activity against coronaviruses” translating into STOP USING THE DAMN SPIKE.
The following paper is correlated with the one above, also on the topic of memory B cells.
Antibody feedback regulation of memory B cell development in SARS-CoV-2 mRNA vaccination
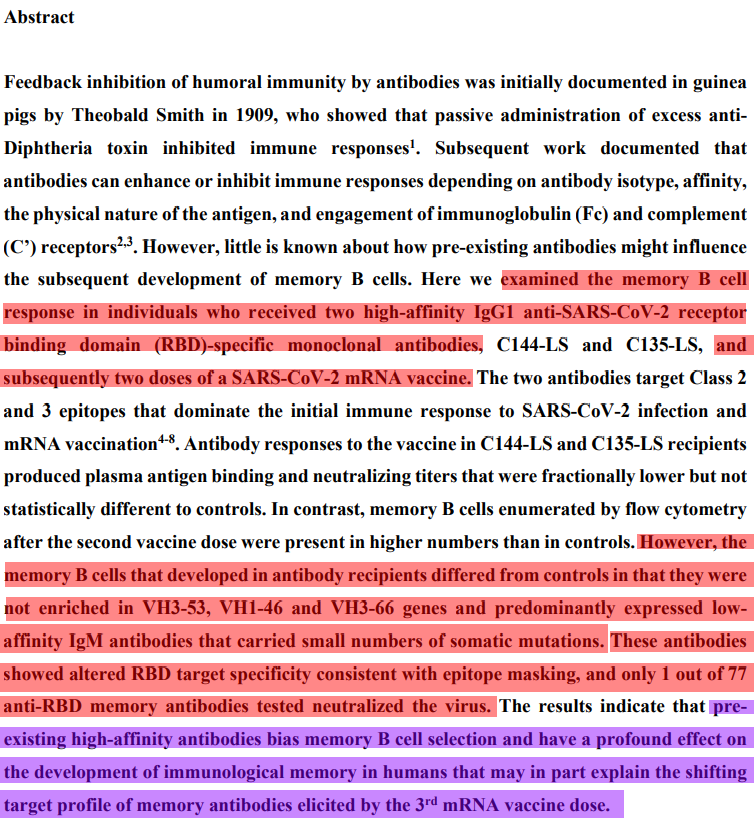
In this paper, the authors decided to measure if the treatment of people infected with SARS-CoV-2 and given a specific monoclonal antibody treatment after 2 doses of the mRNA vaccine could affect the development of memory B cells. What they found was the following.
The memory B cells (these are the antibodies making cells) differed from antibody-treated people and the ones without with
They had fewer genes closely related to antibodies that neutralized the Receptor Binding Domain
They were of low affinity with a small number of somatic mutations, meaning they were less diverse, therefore less neutralizing efficacy
In line with the piece I referred to above, pre-existing B cells “anything” will compete with the mRNA elicited B cells, in this case, even competing with the memory B cells.
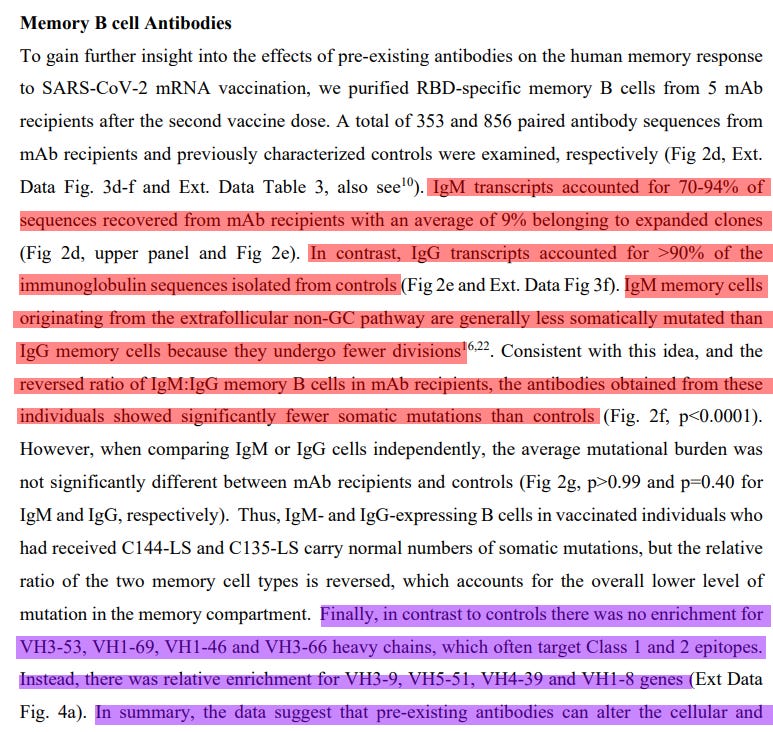

Monoclonal recipients (that were vaccinated after) had a skewed presence of IgM, these are Immunoglobulin M, usually, the first Igs produced by antibodies, short-lived, and sometimes they are no as diverse (important) or specific (even more so), which by the author’s tests leads to poor binding to the RBD. IgGs come after, are long-lived, and are usually the actual measure of an immune response, among many other things.
They also found a change in the genes expressed, which affects the class of epitopes (the little pieces the antibodies are made to bind), which is even more important. Change in class can dictate the effectiveness of the immune response, and clearance at some level. In line with the Pre-existing Immunity, they find using a different design, pre-existing antibodies can alter the composition of these cells.


I will grossly simplify. The monoclonal treatment which is pure antibodies will glue themselves into certain epitopes of the RBD which impede the body from recognizing those epitopes, which will hinder mounting an effective immune response.
The blue highlight speaks for itself. It is a few times. Especially the last 4 lines. This is the second time within weeks I tell you this. If you are curious-minded, scientific literate, or clinician/scientists, you should, no, you must research about non-canonical functions of antibodies.
I wish everyone a very good weekend, if I publish tomorrow will be totally unrelated to Science or anything else I cover here. Go enjoy your weekend.
A very big thank you to all supporters here and those who use KoFi =) !
That monoclonal antibodies and/or convalescent plasma was used in this scenario was a bizarre development from the beginning. The only precedent I am aware of in infectious disease is in the event of potential rabies exposure. The last I knew, rabies had one recorded survivor, and that individual would have been better off not surviving. We use anti-D to prophylax pregnant Rh- women, because sensitization during pregnancy with a Rh+ infant is nearly 100% fatal to the infant. Two scenarios with clear risk/benefit. We otherwise use mAb therapy for cancer patients. If any of you all know of other common monoclonal antibody therapies, please educate us.
Regarding failing memories......my friend is in a bad place with schizophrenia.doctors pumping him full of drugs.niacin helps him before but they wont allow him to mix drugs. Anyone got any insight?( Not medical advice obviously.)
My research suggests schiz patients have increased ROS and neuroinflamation and are Also deficient in gluthatione.
My thinking is he needs fasting lowcarb keto diet.tryptophan to raise gluthatione.and NMN (niacin)as a nad+ booster.