
COVID vaccines increasing eye clot risk up to 2 years
Massive safety signals and how one may address it

3 days ago a quite important paper was published in Nature, and the following day after the publication it went viral, as one would expect.
First, an explanation, Retinal Vascular Occlusion refers to the blockage of the blood vessels in the eye structure (retina in this case) which can lead to vision loss. In this study with a big group of people following up for 2 years, the researchers found that vaccinated people had a significant chance of developing RVO than non-vaccinated and this trend lasted up to two years, 2 weeks after vaccination is the biggest risk, and this higher risk persisted for 12 weeks, both these dynamics in regards to Moderna’s and Pfizer’s vaccines (it is a feature of mRNA…more on this in this piece), the adenovirus had elevated risk of RVO after the first dose, but it wasn’t a significant increase.
“Ultimately, 745,041 vaccinated and 3,874,458 unvaccinated individuals remained. We matched 739,066 vaccinated cohorts to the unvaccinated cohort at a ratio of 1:1.”
A 2.19-fold increased risk of retinal vascular occlusion after COVID-19 vaccination was observed. The incidence of RVO was the same among all ages, gender, and races.
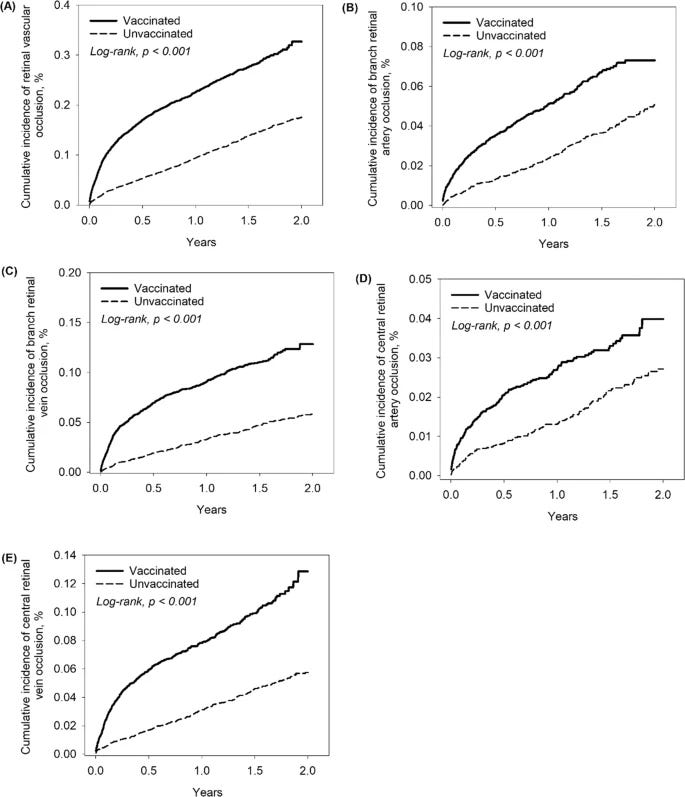
The risk of the same events taking place in the unvaccinated exists, but per the graphs above, it is much lower than among the vaccinated. The many shapes and types of clotting (no pun intended) are a well-known, widely observed effect of the viral infection, its cascade effects, and the vaccination, even though a massive concerted effort has been made the last 2 years to hide this “mildly annoying vaccination side-effect”. For the sake of argument of both sides, it has been widely observed that the Spike alone can induce the formation of many types of clots via different mechanisms, it can directly interact with cells to make the body secrete von Willibrand Factor, an essential part of the coagulation process, one under a tight balance, among quite a few other remarkable mechanisms.
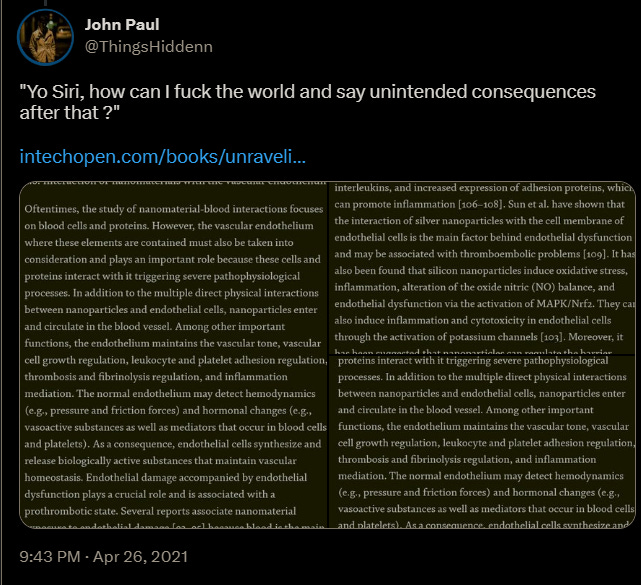
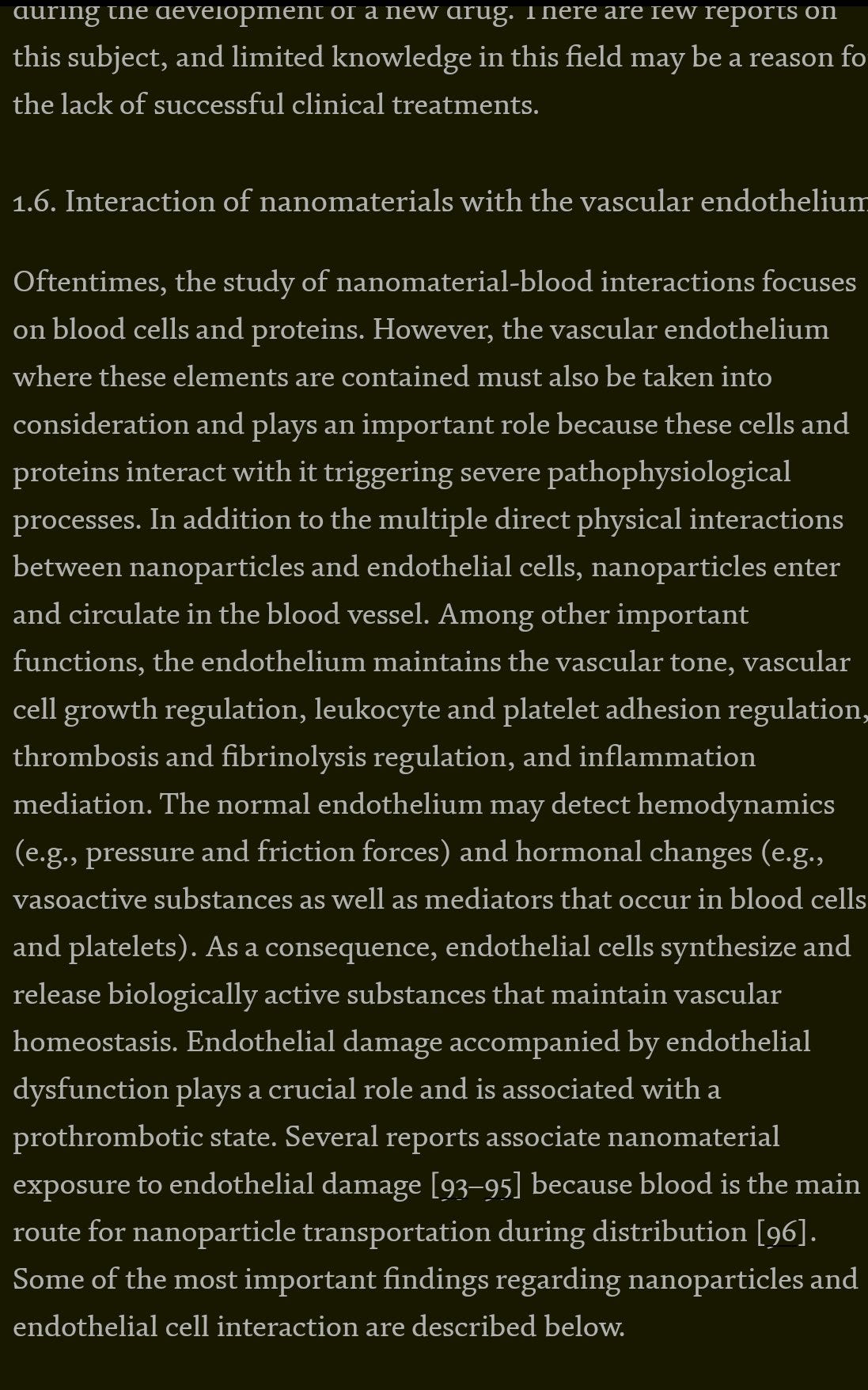
It is a feature of nanomaterials to induce clotting cascades. Source of the following, and my April 2021 tweet about it.
The concern here is both the region, the size of the structure affected, and what it entails, RVO has been known to be both hard to diagnose in a timely manner, and the damage done in the region, the eyes have quite the fragile microvasculature. The chemical composition and structure of the materials of the mRNA alone don’t explain what we just read, but they serve as the primary injury, as an initiator of a hit-and-run effect, making the circulatory system both prone and more susceptible to secondary injury.
The “real” problem is the probable composition of these clots.
SARS-CoV-2, the brain, and amyloid fibers

This is a rather shorter post, that will serve as a build-up to my Amyloid one, that will be lengthy and complex. You better start understanding these, and many other of my posts, otherwise you won’t understand why I call the amyloidogenesis, bullshit.
Besides some other hypotheses that I am working on, the only probable explanation for the long-term presence of micro clots leading to different vascular injuries is the one described above, by which amyloid-based clots are formed, and these are resistant to the body's natural “decomposition” method, rather concerning since Amyloid Beta (the neurotoxic proteins partially responsible for neurodegeneration) directly interacts with fibrinogen forming structurally abnormal clots. The following paper titled Aβ peptide and fibrinogen weave a web of destruction in cerebral amyloid angiopathy is a great resource to understand the complexity of this interaction. And the following is what I call foreshadowing for an article to come…
“Indeed, both molecules may be present as monomers or fibrillar polymers and the relative amount of each species could be quite heterogenous.”
To add salt to injury, doesn’t take too long to find connections between Galectin-3 and its interactions with Amyloid proteins, Gal-3 and its weird partnership with von Willibrand Factor potentially modulating thrombus (clot) formation, and for last gut-derived endotoxins stimulates factor VIII (a different protein, with similar effects as vWF) secretion from endothelial cells influencing hypercoagulability. While there is a highly complex, multifaceted nature to the clotting issue in regard to the virus and Spike, my observations lead me to affirm it often boils down to the NTD and the RBD (parts of the Spike Protein).
Bringing all this context to the readers attention is necessary because the occurrence of RVO is not a contained “problem”, RVO can be used as a sign of systemic vascular/circulatory disease. Higher mortality has been observed too.
Incidence of Retinal Artery Occlusion and Related Mortality in Korea, 2005 to 2018
Findings Based on claims data from 2002 to 2018 in Korea, this cohort study found that the incidence of retinal artery occlusion was 7.38 per 100 000 person-years, and that mortality was significantly higher in patients with retinal artery occlusion (standardized mortality ratio, 7.33), most commonly due to cardiovascular or cerebrovascular disease.
Meaning These findings suggest that the risk of cerebrovascular or cardiovascular disease in patients with newly diagnosed retinal artery occlusion must be investigated.
It can also influence the development of (vascular) dementia.
Relationship between Retinal Vascular Occlusions and Cognitive Dementia in a Large Cross-Sectional Cohort
Individuals with retinal vascular occlusions have a higher prevalence of dementia. However, this association is secondary to shared underlying risk factors in this population, such as older age and stroke.
It is better to address these pathological effects in this piece rather than in a standalone one, and I will make it brief and short.
Before going into the supplementation, I would like to reinforce that the vaccinated must (this one isn’t a suggestion) supplement proteolytic enzymes for at least a few weeks, 4 to 8 weeks more if necessary. Serrapepatase and Natto or Lumbrokinase. Slowly increasing the dosage as you feel more comfortable until you hit roughly 400.000-600.000 units, every other day.
Attention is necessary when using high dosages of these enzymes because they will dissolve any unwanted protein and this includes bacterial and fungal biofilms this can lead to major discomfort or outright “allergic reactions” that aren’t fatal but ain’t pleasant. Start low, increase slowly, even if you have to take the enzymes for a longer period of time.
I have personal experience with the clot-dissolving properties of these enzymes and have suggested them to many people in a similar position. It works, but this isn’t a targeted drug, it is a (systemic) supplement, natural, so it takes time. Following are some of the options one may use.
Long-term use of Niacin can ameliorate and help with what we just went through, ameliorating and helping the eye to heal, 500 mg was the dosage in the paper linked. (I personally take 250 mg daily).
B12 and folate deficiency are directly correlated with RVO, and supplementation will also help.
Aspirin has just too many uses to list, it deserves an entire (complex) substack on its own. I have started recently taking 500 mg twice a day, but it is too soon to talk about any improvement, but I would highly advise short-term usage of aspirin, among the vaccinated long-term should be heavily encouraged.
Olive Leaf Extract can also be helpful to treat and heal the endothelial dysfunction itself, and should be considered by anyone with any signs of circulatory problems (vaccinated or not).
NAC is also fairly helpful via a different mechanism than the ones described above. Niacin dilates the body vessel, among dozens of other effects, Aspirin “thins” the blood but it does so much more, similar to Niacin.
Metformin has a direct preventive effect in diabetics, but given its many, many other pathways and effects, it will also work (especially allied with other supplements).
If supplementation can’t achieve the necessary recovery, the “last resort” I suggest is peptides. And to be abundantly clear these suggestions are but a few, just the ones I am rather confident on and have synergy among themselves and many of my other suggestions.


Thank you to my supporters, and also readers and people who share my substack.
Great post ! my wife's friend (covishield 2 doses) developed serious eye problem (forgot the name) and taking daily steroid as otherwise she will lose vision anytime in coming months or years, this steroid too wont help in long run too but atleast the red ,popping out eyes and itching and all things wont happen(this is what the doctor said) , soon after her daughter developed vision issues and got high power specs ( i dont think its related but mentioned still, the child is not vaxed).. ..one thing would like to add regarding use of aspirin, one knowledgeable doctor told me that if someone is taking aspirin for more than 21 days they must take famocid(or anything similar ) too, else there might be problems, then one of my friends mom was advised aspirin low dose after one operation for 6 months, she developed diverticulitis, hinted them about aspirin long term side effect and diverticulitis and then it was found that aspirin was the culprit, doctor did not recommend any antacid with it... i am not expert, but just try to understand the happenings with some logic, maybe this info will be useful... Mnay thanks for your articles...also can i have your email? thanks again
Another outstanding effort! BTW I sent you a message via Turanota.