

Given the last 4 weeks and the higher quantity of significant papers being published, I will do something rather unusual here, I will highlight the most important sections of the papers, attempting to make them simpler, rather than intricate. The main goal of this one is proving a “small guide” for any person suffering from conditions similar to Long Covid on what to test.
Also since I am not fond of “substack baiting”, in regards to one of the most important dynamics of SARS-CoV-2 and Long Covid, here are two recent papers on Herpes reactivation and Covid vaccines, with mRNA being overrepresented in the reactivation of said viruses.


Biomarkers in long COVID-19: A systematic review
Methods: A systematic literature review in PubMed, Embase, and CINAHL was performed on 18 August 2022. The search keywords long COVID-19 symptoms and biomarkers were used to filter out the eligible studies, which were then carefully evaluated.
Results: Identified from 28 studies and representing six biological classifications, 113 biomarkers were significantly associated with long COVID: (1) Cytokine/Chemokine (38, 33.6%); (2) Biochemical markers (24, 21.2%); (3) Vascular markers (20, 17.7%); (4) Neurological markers (6, 5.3%); (5) Acute phase protein (5, 4.4%); and (6) Others (20, 17.7%). Compared with healthy control or recovered patients without long COVID symptoms, 79 biomarkers were increased, 29 were decreased, and 5 required further determination in the long COVID patients. Of these, up-regulated Interleukin 6, C-reactive protein, and tumor necrosis factor alpha might serve as the potential diagnostic biomarkers for long COVID. Moreover, long COVID patients with neurological symptoms exhibited higher levels of neurofilament light chain and glial fibrillary acidic protein whereas those with pulmonary symptoms exhibited a higher level of transforming growth factor beta.
Conclusion: Long COVID patients present elevated inflammatory biomarkers after initial infection. Our study found significant associations between specific biomarkers and long COVID symptoms. Further investigations are warranted to identify a core set of blood biomarkers that can be used to diagnose and manage long COVID patients in clinical practice.
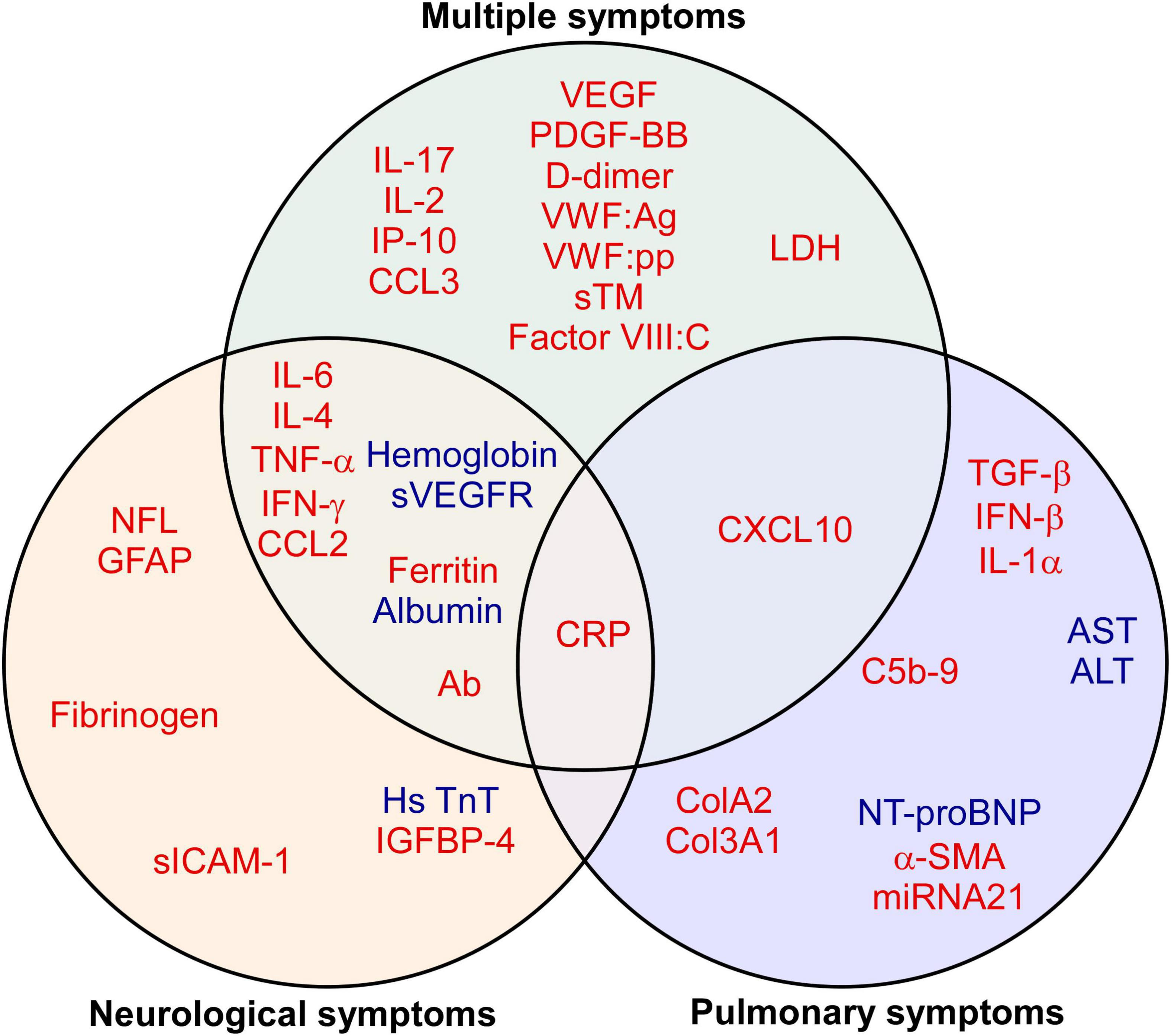
By doing a meta-analysis (reading scientific papers related to a subject and finding trends/common denominators) the authors found markers that are grouped into 3 different types of Long Covid. Given the complexity of interactions and all the cascade effects each of these proteins may represent, there is a somewhat common overlap between the markers, but a distinctive profile surfaces.
IL-6, TNF-alpha, and CRP (C-Reactive Protein) are universal inflammatory markers, and it is common to find high levels of any of these markers in severe patients and after a severe infection or hospitalization, consistent with literature prolonged presence of the 3 markers implies systemic inflammation and often neurological symptoms in Long Covid.
Neurological sequelae and symptoms are the most common in Long Covid, and here the authors found higher levels of specifically two neural peptides that may serve as biomarkers for neuronal degeneration and damage. NFL, and GFAP. Here is where I attempt to add and connect dynamics outside the scope of the paper.
Higher levels of NFL are associated with Varicella-Zoster Virus (Herpes Zoster) infection in the central nervous system. Similar to EBV, another source linking NFL, EBV, and the role of Epstein Bar in the development of Multiple Sclerosis. This trend repeats itself with other members of the family, such as HHV-6 and CMV, all these viruses having a role to play in neurodegeneration, neurological inflammation, and of course, Long Covid.
An inflammatory marker on its own, Ferritin and its dysfunctional levels, sometimes very low, sometimes very high has been one of the hallmark markers of SARS-CoV-2 infection, and to an unexplored level vaccination, and you guessed it at this point, higher levels of ferritin, especially in regards SARS-CoV-2 and HHV-6 co-infection is correlated with higher levels of ferritin. In many other clinical scenarios, HHV-6 infection and reactivation will skyrocket ferritin levels.

IFN-y (gamma) is well known to most of my readers by now. So in case you or someone with Long Covid has persistent symptoms, especially neurological to this point, and persistent higher levels of these, it is worth talking to the healthcare provider and testing for active or viral reactivation of Herpes Viruses, of course, sometimes it is not as simple. I had two of my readers contact me, and after months of back and forth (them with doctors, with me attempting to provide some guidance and clues), it was found that both persons had different active infections of E. Colie (157) and Amoeba. Shiga toxins are the main problem with E. Coli and for simplicity's sake will have similar effects as endotoxin (LPS). An interesting fact, Shiga toxins can interact with LPS and similar to the Spike Protein create a compounding inflammatory effect.
Attention was brought towards other markers, many of them related to pulmonary damage (fibrosis especially) such as TGF-Beta, and many endothelial markers such as vWF, and VEGF, but of special interest to me IL-17. All of these are very important new markers for sepsis, but TGF and IL-17 can also be markers for active fungal infection, something unbelievably overlooked in regard to all this.
To summarize, if you or a person you know who suffers from Long Covid took any decently enough protocol and saw mixed or little improvement, or has a persistent but significant symptom after months, all these markers and potential latent pathogens (viral, or fungal) are worth exploring. You can find more about fungal infections and SARS-CoV-2 below.

The plasma metabolome of long COVID patients two years after infection
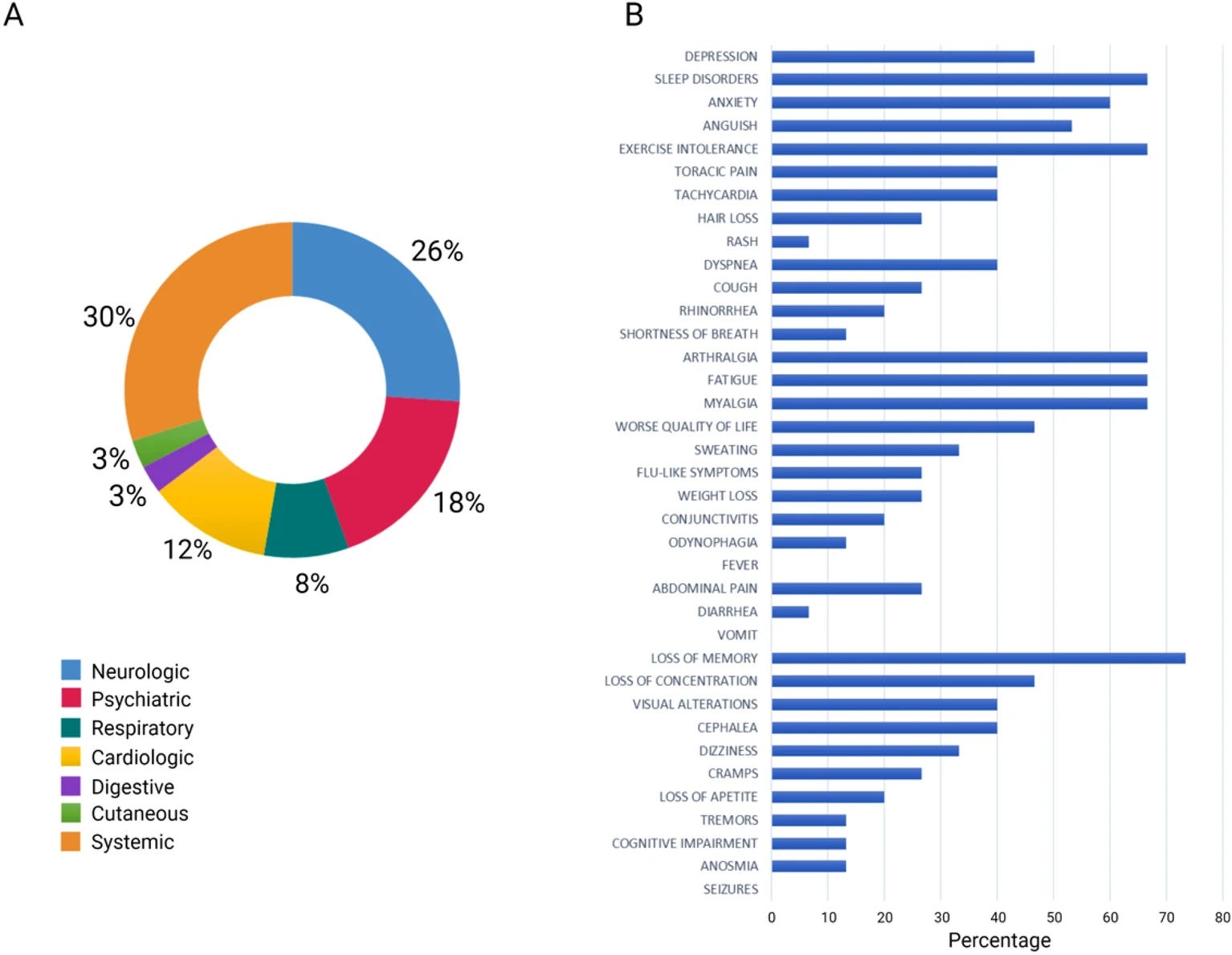
The metabolome is a term used to describe the comparison of many low molecular weight molecules (metabolites) that participate in metabolic reactions. Metabolites are the byproducts of metabolic reactions often initiated by enzymes inside cells. Many metabolites are bioactive, such as the ones participating in the breakdown of Tryptophan (the Kynurenine Pathway). One of the advantages of this study is the fact these symptoms were measured long-term, only symptoms that remained for over 20 months, and a clear correlation with the 3 different groups of Long Covid patients in the paper above is easy to spot.
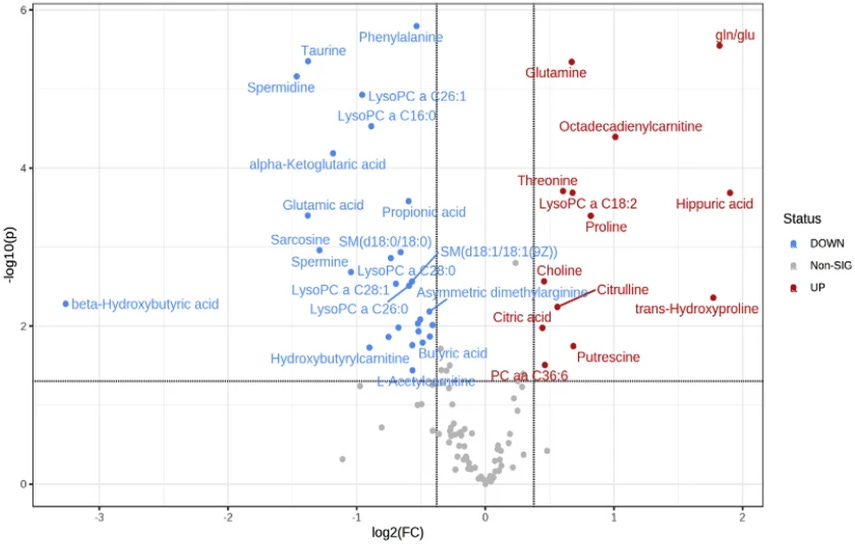
When comparing the metabolites between others and people with Long Covid, 53 plasma metabolites were found to be significantly different, with 13 being upregulated, and 32 down-regulated. Phenylalanine, taurine, glutamine, and spermidine had lower concentrations in Long-Covid, while the glutamine/glutamate ratio was increased. To be certain these altered levels were dysregulated when compared to “normal levels” a group of negative SARS-CoV-2 samples was used, collected in 2020, and added to the analysis, the trend remained, meaning these metabolites are persistently dysregulated in Long Covid.
The authors divided the Long Covid group into 2 groups, Group A belonging to anyone with up to 5 symptoms, and Group B - anyone with more than 5 symptoms. The best marker to differentiate Group B from everyone else was Lactate/Pyruvate ratio.
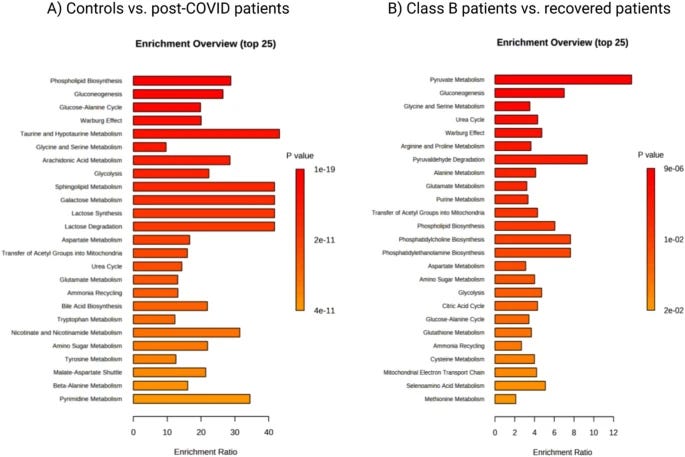
Their next step was pathway analysis. The top 5 metabolic pathways significantly dysregulated in post-Covid patients compared to control were phospholipids biosynthesis, gluconeogenesis, the glucose-alanine cycle, taurine, hypotaurine metabolism, and the Warburg Effect. When comparing Group B with recovered, the pathways were: pyruvate metabolism, gluconeogenesis, glycine and series metabolism, urea cycle metabolism, and the Warburg Effect.
Before going any further, here is a tidbit I preferred to state midway. All patients were “fully vaccinated”, and this will be important when I write my closing remarks.
There is no consensus, proper guidelines or even testing to classify and differentiate patients with Long Covid, and sometimes studies will only use questionnaires with some biomarkers, these are often studies I don’t bother writing about because of a lack of comprehensive or novel findings. Here the authors used both, questionnaires and molecular biomarkers to effectively find a way to correctly classify patients.
In line with clinical observations, dozens of papers published so far, and epidemiological evidence, they found one of the main dysregulated metabolites was glucose and pathways involved with glucose. Abnormalities in glucose metabolism, or glycemic levels (how much sugar you have floating around in your blood) have been observed after infection, sometimes even months after infection poor glycemic control is still present.
Taurine and spermidine were significantly decreased in Long Covid but tended towards normal levels, low levels of both are observed in ME/CFS patients too. Taurine has roles in skeletal muscle, the central nervous system, and energy metabolism. They also found increased levels of kynurenine, and this also trended into normalization in the tryptophan and kynurenine/tryptophan ratio in Long Covid. This indicates that although lower in magnitude compared to other metabolites, the inflammatory conditions found in LC contribute to the persistent activation of this pathway and account for some of the persistent physiological symptoms.

Another important pathway that is dysregulated is the glutaminergic pathway, which glutamine and glutamate belong to. Glutamine depletion is observed during Covid infection and it is linked to various functions such as energy production, virus synthesis, immune function, and pH balance. Dysregulation of this pathway is linked to the Warburg effect, diabetes, and many inflammatory diseases. After Covid, increased glutamine and decreased glutamate may indicate recovery, but in Long Covid with persistent (months long) symptoms it shows ongoing immune dysregulation, affecting the glutamine/glutamate balance. An imbalance in this ratio can lead to neurological issues. Not directly cited by the authors, it also plays a role in both sepsis and cancer.
Patients with 5 or more symptoms (Group B) had increased levels of lactic acid, similar to ME/CFS patients. This indicates mitochondrial dysfunctions. In the author’s own words.
Increased level of the lactate/pyruvate ratio in class B patients is another important indicator of mitochondrial dysfunction. The lactate/pyruvate ratio has been proposed as a marker for mitochondrial disorders since it indirectly reflects the NADH/NAD + redox state, lipid metabolism (fat oxidation), and ATP generation. In our study, both markers (lactate and the lactate/pyruvate ratio) were found positively correlated with fatigue, myalgia and arthralgia

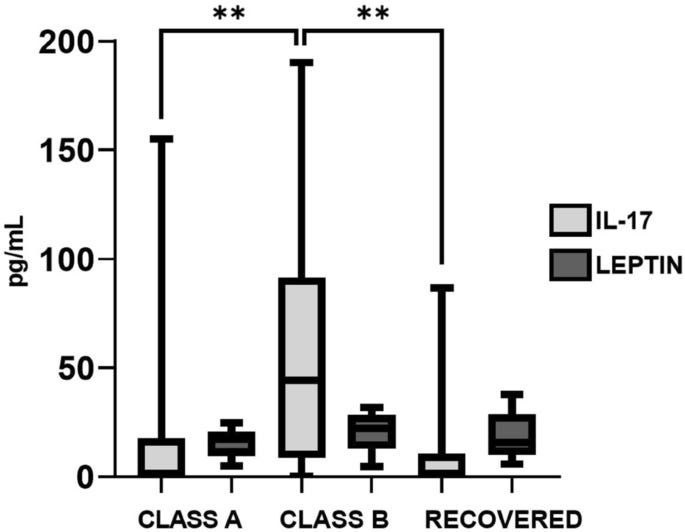
The author’s proposed interventions are very closely related to mine, which I proposed back in mid-2021, which is good since consistency is key in my opinion, and now with further evidence towards said supplementation. You can find my suggestion here, but be advised I need to rewrite most of it and make it simpler to understand, but it is a good starting point. Midway through this paper I wrote that I omitted that every person in this study was vaccinated, for a reason, I didn’t want to take away their findings and pin it all on the vaccines, but it is important on many levels. The authors found IL-17 to be abundant in Group B.
Interleukin-17 and its “parent” cell T Helper 17 (Th17) were my primary interest, and the starting point of my reverse engineering of the immunological response of both virus and vaccine, but especially the last one. Inside the Substack below you will find my usual analysis and 3 other substacks covering the subject.
In case you wondered at any time, the preferred metabolism of Th17 cells is glycolytic, to be precise, the Warburg Effect. (Yes I will write about it at a point in the near future, since…)



Here is a short guide on how one should address Long Covid biomarkers, often what I suggest to people in the last 2 years.
Stage 1 - If there are high levels of inflammatory markers such as the ones in the first image, more testing is needed, with special attention to IL-6 and IL-12
Stage 2 - Testing levels of TNF-Alpha and IFN-Gamma, also VEGF, if those are high
Stage 3 - High levels of these may indicate the presence of latent or chronic infection, with special attention to all mentioned in the Latent Infections substack
Stage 4 - If negative for most latent or chronic infections, testing for dysbiosis, gut permeability, and your microbiome is helpful, the answer may reside here such as in the E. Coli case
At some point, it is beneficial to test for autoantibodies, of significant interest if symptoms are months long, and there are severe ups and downs.
I will leave the third paper that I would have covered here, for the day after tomorrow.

If you chose to become a supporter, thank you ! And thank you for reading too.
I will publish another post on viral persistance and Long Covid, and days later probably something else, but it is time for me to stop chasing the hamster wheel of my own making, so I can focus completely on Endotoxic Tolerance and perhaps Warburg Effect, since without Endotoxic Tolerance, I can't publish the "final" section of this part of the puzzle.
As with all social media sites, Substack severely punishes authors that don't publish with consistence, alas sacrifices must be made.
Thanks John. Reading around the subject taurine and spermidine are associated with gut bacteria and inflammatory Prevotella bacteria too, also due to gut dysbiosis.
Indoles from gut bacteria too are a contributory factor we've looked at before and glutamine depletion due to viral replication.
***
Evidence for Altered Glutamine Metabolism in Human Immunodeficiency Virus Type 1 Infected Primary Human CD4+ T Cells
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5709700/
Inflammation-type dysbiosis of the oral microbiome associates with the duration of COVID-19 symptoms and long COVID
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10017104/