
The hidden complexity of latent infections
SARS-CoV-2, Long Covid, cognition

To have a complete context of everything we are about to go over here, you must read basically all my recent SARS-CoV-2 pieces and any piece suggested inside, such as the complexity of the cascade. This is a standalone piece, but for the “big picture”, that would be advisable. This piece also ended up being big and might not show up properly in your e-mail.
For easier understanding, for the visual learner, and also working as a summary of the most important points.

While parts of this piece sat here and new evidence surfaced, changes were made, so at points, I just briefly mention or cover a paper or mechanism, such as the first, and incredibly important concept to keep in mind in the long term.
In this remarkable paper, we find the duality of autoantibodies. Here the authors discovered that antibodies against specific chemokines (little cytokines that literally move your immune cells to where they are needed) and these autoantibodies against these specific chemokines were found to be both favorable against disease severity and negatively correlated with the development of Long Covid even at 1-year post-infection.
The research is remarkably well done, and one of the points that peaked my attention the most was the one where they analyzed the pattern of chemokine antibodies in Covid-19, HIV-1, and certain autoimmune diseases, demonstrating very distinct profiles in each.
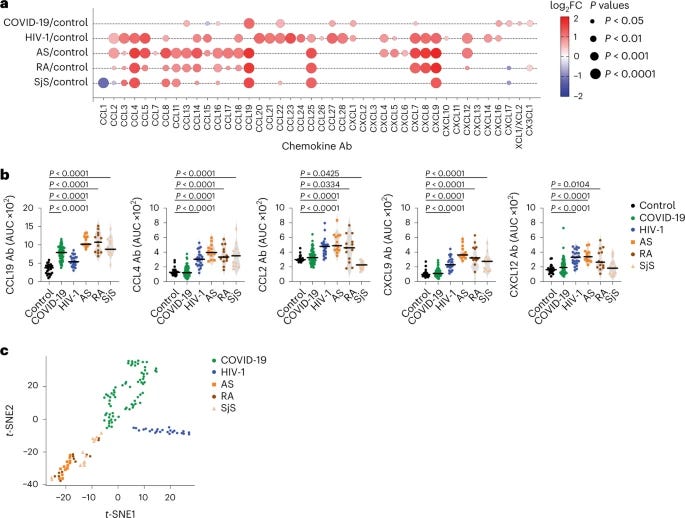
Autoantibodies to CCL21, CXCL13 and CXCL16 were increased in recovered individuals compared with those with long COVID 1 yr post-infection. These chemokines are important for tissue trafficking and activation of T and B lymphocytes. It is possible that their respective autoantibodies positively impact the long-term outcome of COVID-19 by antagonizing or otherwise modulating the activation, recruitment and retention of these cell types. Persistent immune responses have been proposed as a mechanism for long COVID, and chemokines have been implicated in its pathogenesis.
These autoantibodies against specific chemokines not only can help predict disease stages (or in simple terms if a person is shifting from moderate to severe infection), but also limit damage to your organs and muscle, both short and long-term, basically a defense mechanism of the body to protective itself in the long run.
This has been one of my running internal debates for months, about how autoantibodies have a bad reputation and are often miscategorized, yes the quality of life of people who developed certain autoantibodies decline, at points drastically but… you are still alive. This is a very complex topic, but many of the chemokines cited in the paper in regard to other diseases all often have a duality in function (which I referred to in the past few months as non-canonical functions).
Since I changed user names on Twitter one too many times, I can’t find my 2020 or 2021 tweets about this particular matter. I also have quite a number of Substacks mentioning the interplay between latent viruses and different diseases.


In this interesting paper researchers uncovered the dysregulated levels of autoantibodies against neuronal and nervous systems in Covid-19 patients, it had a total of 246 participants, 169 “infected” and 77 controls (healthy people, never infected). The authors raise an interesting point of epitope spreading, when the immune system “broaden” the antigens it can target, meaning it can target other “parts” of the virus and if those parts are closely related (mimic) antigen of our own cells, it can set off autoimmunity, or fuel inflammatory processes. The other point is the presentation of cryptic antigens, hidden antigens that can be exposed when there is an alteration of the normal state of proteins.
COVID-19 patients were found to have dysregulated autoantibody levels correlating with the disease severity, e.g., IgG to dopamine 1 receptor, NMDA receptors, brain-derived neurotrophic factor, and myelin oligodendrocyte glycoprotein. Elevated levels of IgA autoantibodies against amyloid β peptide, acetylcholine receptor, dopamine 2 receptor, myelin basic protein, and α-synuclein were detected in COVID-19 patients compared with healthy controls. Lower IgA autoantibody levels against NMDA receptors, and IgG autoantibodies against glutamic acid decarboxylase 65, amyloid β peptide, tau protein, enteric nerve, and S100-B were detected in COVID-19 patients versus healthy controls. Some of these antibodies have known clinical correlations with symptoms commonly reported in the long COVID-19 syndrome. Conclusions: Overall, our study shows a widespread dysregulation in the titer of various autoantibodies against neuronal and CNS-related autoantigens in convalescent COVID-19 patients. Further research is needed to provide insight into the association between these neuronal autoantibodies and the enigmatic neurological and psychological symptoms reported in COVID-19 patients.
Later on, they proposed that some of the antibodies may be exactly as I described at the start of this piece, it may as well be a compensatory response towards stimuli, the viral infection, or tissue damage. The fact that any person develops autoantibodies regardless of disease severity is in line with the first paper, a protective response towards a substantially aggressive cascade. Here is where I diverge from their paper and propose something else, in line with the theme.
First and to “take some things out of the way” bear in mind a lot of the proteins related to neurodegeneration have antimicrobial effects, meaning they often are produced in response to viral or bacterial (dare I say, fungal) infections.
Our results are in correlation with recent observations indicating antibodies against NMDA receptors in the cerebrospinal fluid of eight COVID-19 patients suffering from autoimmune encephalitis [22]
Herpes Simplex Virus-1 encephalitis can trigger anti-NMDA receptor encephalitis, in simple terms virus awakens > gets treated > weeks go by > gets reactivated > triggers encephalitis again by setting off autoantibodies against NMDA. Another case report, this time faster than others, notes these are both young adults. Another case report with 2 people and a quote “HS (herpes simplex) virus infects neurons produce a higher likelihood of contracting anti-NMDA receptor antibody encephalitis”
A case report for the same autoantibodies and HHV-6. EBV reactivation setting of anti-NMDA receptor encephalitis. Humoral cross-reactivity between α-synuclein and herpes simplex-1 epitope in Parkinson's disease, a triggering role in the disease?
The list goes on not only with a sufficiently strong correlation between latent viruses, autoantibodies, and the development of autoimmune diseases, a classical case would be Epstein Barr Virus and Hashimoto’s disease (autoimmune thyroid disease).
This paper is rather complex and incredibly significant and I may later come back to it on its own, or build upon this entire piece with more emphasis on this one. This serves as an annotation for anyone to further read into it because it deserves special attention.
The authors here have been doing research on what some call “post-viral syndrome”, or as it is referred ME/CFS and Long Covid, and postulated for some time that herpesviruses reactivation are one of the key mechanisms which both ME/CFS and Long Covid develop, this is a line of thought corroborated by many other groups. Here they found evidence of frequent HSV-1 and EBV reactivation in both conditions and also found that ME/CFS patients have a depletion of natural IgM (nIGM).
Before going any further one specific finding needs clarification. The enzyme dUTPase, also known as deoxyuridine triphosphatase, is an essential enzyme involved in DNA metabolism, its activity is crucial for maintaining the fidelity of DNA synthesis and preventing the incorporation of uracil into DNA, uracil-DNA is recognized by DNA repair enzymes, but if they are left unrepaired it leads to mutagenesis and genomic instability. In simple terms, dUTPase is essential for life, but in regards to pathogens they are not only essential for their viability, but they are active biological enzymes inside humans, and they play a (significant in my opinion) role in human disease.
Increased HSV-1 and EBV reactivation in ME/CFS and long COVID
Reactivation of different herpesviruses including HHV-6, HHV-7 and EBV is frequently associated with ME/CFS development. To test the possibility that these dormant viruses are being reactivated in long COVID patients and are producing dUTPases, we examined the humoral response against the viral dUTPases of EBV, HHV-6 and HSV-1 in a cohort of patients (n=278) at least after 6 months of first SARS-CoV-2 infection. Only 6% of the patients of this cohort were hospitalized during the acute SARS-CoV-2 infection while rest of the 94% of the patients had mild to moderate SARS-CoV-2 infection without the need for hospitalization
The results of their tests showed higher antibody responses against EBV and HSV-1 dUTPases in both ME/CFS and Long Covid patients. Higher antibody (IgG) response to HSV-1 dUTPase was detected in both mild and severe Long Covid patients. A modest increase of IgG against HHV-6 dUTPase was observed in ME/CFS, but not in the group of SARS-CoV-2 infected patients, which had decreased IgG response against said dUTPase in comparison to healthy controls. These point towards an increase in EBV and HSV-1 reactivation in both ME/CFS and SARS-CoV-2 patients.
The authors previous work with dUTPase belonging to herpesviruses demonstrated they have a ligand function, uncovering a novel function with immune and neuromodulatory effects, independent of its enzymatic reaction, they decided to research further effects, since this anti-dUTPase antibody response was found 6 months after the first SARS-CoV-2 infection which suggests reactivation contributes to developing Long Covid. The authors found that the dUPTase of both EBV and HSV-1 deeply affected the host cell cytoskeleton and alter mitochondrial architecture as well as function.
Remember my Mitochondria centered substack, cell shape is important, especially in regards to mitochondria shape, directly influencing its function. EBV had a strong impact on mitochondrial health and bioenergetics. This comes to corroborate many observations in the last 3 years, as both the Spike and latent viruses will directly affect mitochondrial function.
One of the most remarkable points of this research was that both ME/CFS and Long Covid patients tested by the researchers had increased amounts of circulating fibronectin which directly correlates with disease severity, and in the case of SARS-CoV-2 patients they found a decreased in natural IgM (antibodies) against fibronectin, which can work as a way to distinguish SARS-CoV-2 infected but not suffering from Long Covid with those who do and severe ME/CFS.

I will reiterate that this paper deserves a second reading and your attention, it has a lot of clues to what SARS-CoV-2 might be doing “under the hood” and also hold clues to how, potentially, the mRNA rewired the B cell response in many.
The last paper also gives us a lot of “clues” to one of the main “roots” of Long Covid and the long-term consequences of Spike exposure, viral or synthetic, but this was done with patients before any vaccines were available. In this paper, the authors collected and assessed the immune activation at up to a year in 63 patients ranging from mild to severe disease to find if there was an association between said activation and Long Covid. At 3 months in patients with severe disease displayed persistent activation of CD4 and CD8 cells, and elevated plasma of IL-4, IL-5, Tumor Necrosis Factor Alpha, and… Interleukin-17.
Here the authors found distinct immune responses both at 3, 8, and 12 months, severe Covid patients have a distinct inflammatory response that lasts well over 3 months after being in a hospital, and this inflammatory response persisted. Each subgroup of patients had a distinct immune response towards SARS-CoV-2, with moderate patients having a strong immune response towards the virus, and higher Receptor Binding Domain-specific antibodies compared to mild patients, showing that moderate infection here elicits a stronger and more protective (long-term) immunity. Since severe patients had a persistent activation of CD4, CD8, therefore, a persistent inflammatory reaction, the authors thought it could be bystander driven.
The higher responsiveness of CMV-specific T-cells, which are highly differentiated cells, has been proposed as a mechanism to explain why these cells are commonly activated/proliferating during acute viral infections such as dengue, HBV, and COVID-19 (Sandalova et al., 2010; Rivino et al., 2015; Gregorova et al., 2020). It may be possible that the low-level proliferation of CMV-pp65-specific CD4+ T-cells observed in this study is driven by cytokines which are still elevated at 3 months. Our data does not support the persistence of SARS-CoV-2 antigens at 3 months for two reasons. Firstly, we would expect that the persistence of SARS-CoV-2 antigens in vivo would result in the activation of SARS-CoV-2-specific T-cells, however we did not observe expression of markers of activation nor proliferation in spike-1-specific T-cells in our ICS analysis. Secondly, we did not detect any SARS-CoV-2 RNA by RT-PCR - however we cannot exclude that SARS-CoV-2 antigens may still be present but are sequestered in specific sites to which T-cells do not have access.
And they chose to test another member of the Herpes family, CMV, and found that yet again, a latent virus may be the culprit in the persistent immune response following SARS-CoV-2, and they may be involved in the inflammatory processes here. It is interesting that they don’t totally disregard the viral fragment theory, but they did not find the persistence of viable fragments or in their tests SARS-CoV-2 antigens here. However, I don’t agree with their conclusion, completely disregarding any association between SARS-CoV-2 and Long Covid, since similar to other aggressive respiratory infections, or Sepsis, the primary hit leads to the reactivation of a secondary pathogen that throws the body into a confused feedback loop (the run in Hit and Run effect).
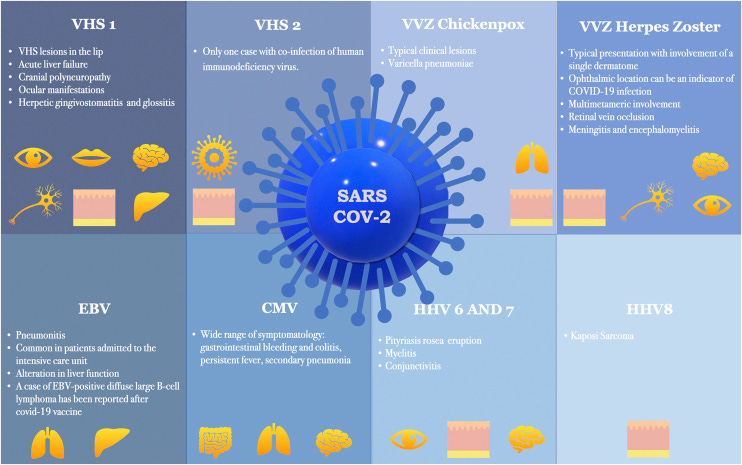
Besides Sepsis reactivating multiple latent viruses, Covid-19 and its vaccines do the same. SARS-CoV-2 literature has quite a number of papers covering herpesviruses reactivation, the most recent being quite well written.
“COVID-19 infection and vaccines: potential triggers of Herpesviridae reactivation”

Since the onset of the COVID-19 outbreak, numerous articles have highlighted a possible link between COVID-19 vaccination or infection and Herpesviridae co-infection or reactivation. The authors conducted an exhaustive literature review on this topic, the results of which are presented individually for each member of the Herpesviridae family: Herpes Simplex Virus (HSV) types-1 (HSV-1) and 2 (HSV-2); Varicella-Zoster Virus (VZV); Epstein-Barr Virus (EBV); Cytomegalovirus (CMV); HHV-6; HHV-7; and HHV-8. These human herpesviruses can serve as prognostic markers for the COVID-19 infection and may even underlie some of the clinical manifestations initially attributed to SARS-CoV-2. In addition to SARS-CoV-2 infection, all corresponding vaccines approved to date in Europe appear capable of inducing herpesvirus reactivation. It is important to consider all viruses of the Herpesviridae family when managing patients infected with or recently vaccinated against COVID-19.
Herpes Simplex Virus 1 (HSV-1) Reactivation in Critically Ill COVID-19 Patients: A Brief Narrative Review
Key Summary Points
Systemic or pulmonary reactivations of HSV-1 have been reported in patients with COVID-19, frequently posing a dilemma for clinicians in terms of their clinical relevance
Prevalence of HSV-1 reactivation may be as high as > 50%, but with large heterogeneity across studies, likely reflecting the different definition, samples and/or cut-offs employed for defining reactivation
Various approaches ranging from prophylaxis to selected antiviral treatment of patients with clinically manifest reactivations have been adopted across different centers
This lack of standardization hampers comparability and generalization of research findings and in turn the understanding of the best approach to patients with COVID-19 and HSV-1 reactivation in clinical practice
Is viral reactivation only important for developing Long Covid ? Absolutely not, the reactivation of many herpesviruses and other polyomaviruses have disproportionally significant and severely overlooked roles in the long-term development of many diseases, which I will glance over but welcome anyone to look further, you will find a strong correlation between these pathways and what SARS-CoV-2 arguably induces on its on.
Herpes Zoster reactivation is known to cause neuropathic pain and can cause unbearable itching.
HHV-6 reactivation in ME/CFS patients activates a multisystem, proinflammatory, cell danger response that protects against certain RNA and DNA virus infections but comes at the cost of mitochondrial fragmentation and severely compromised energy metabolism. HHV-6 viremia affects T cell reconstitution after allogeneic hematopoietic stem cell transplantation, it wouldn’t be far-fetched to deduce it may play a similar role in infection, this could explain why some people have a hard time recovering CD4 cells, among other reasons.
In the latent phase, HHV-6B may be involved in the onset of depression.
This study show a marked elevation in CSF KYNA from patients with HSE, most pronounced during the acute phase of the disease and slowly declining along the recovery. We propose that brain KYNA might potentially protect against neurodegeneration while causing a long-lasting loss in cognitive function associated with the disease. In simple terms, the body produces a lot more Kynurenic Acid (from the Kynurenine Pathway) in response to Herpes Type 1 encephalitis, while protecting from damage, it causes long-lasting loss in cognitive function.
HHV-6 and HHV-7 immune suppressive activities may also indirectly contribute to fungal, bacterial, or human cytomegalovirus (HCMV) infections (Boeckh and Nichols, 2003; Ljungman, 2002. Reactivation of HHV-6 as the cause of acute liver injury during drug reaction.
The Role of Human Herpesvirus 6 Infection in Alzheimer’s Disease Pathogenicity—A Theoretical Mosaic is an intriguing paper to read, showing both sides of the argument.
Cytomegalovirus and Epstein–Barr virus co-infected young and middle-aged adults can have an aging-related T-cell phenotype. EBV dUTPase can induce impaired learning and memory.
Epstein-Barr Virus Infection Induces Indoleamine 2,3-Dioxygenase Expression in Human Monocyte-Derived Macrophages through p38/Mitogen-Activated Protein Kinase and NF-κB Pathways: Impairment in T Cell Functions (Meaning EBV directly activates the Kynurenine Pathway and creates a metabolic trap while causing T cell dysfunction)
Experimental data show that HSV-1 infection of neurons activates neurotoxic pathways typical of AD, and repeated HSV-1 reactivations in the brain of infected mice produce an AD-like phenotype. Overwhelming Evidence for a Major Role for Herpes Simplex Virus Type 1 (HSV1) in Alzheimer’s Disease (AD); Underwhelming Evidence against
HHV-6 meningoencephalitis in an immunocompetent patient with influenza virus co-infection
These data support the notion that Aβ might play a protective role in CNS innate immunity, and suggest an AD etiological mechanism in which herpesviridae infection may directly promote Aβ amyloidosis. Another interesting paper here “Our data established that H4 neuroglioma cells produced Aβ42 in response to HSV-1 infection thus inhibiting secondary replication. This mechanism may play a role in the etiology of AD.”
(This is one of the many reasons I never took any of the “amyloid” people seriously, for lack of a better way of saying this, they had little idea of the complexity of amyloid formation, and function).
Host-Immune Interactions in JC Virus Reactivation and Development of Progressive Multifocal Leukoencephalopathy (PML) (if you search for PML and Covid-19 you will get many results).
The oncogenic roles of JC polyomavirus in cancer
Lipopolysaccharide enhances HSV-1 replication and inflammatory factor release in the ARPE-19 cells
This is but a fraction of the complex relationship between SARS-CoV-2, its Spike Protein, and latent viruses from the Herpes and Polyoma family, with a keen interest in John Cunningham Virus (JCV), a virus that can remain latent in the spleen, lymph node, bone, kidneys, and the brain, and can induce lymphadenopathy when reactivated.
What is discussed here will also be important when I write my (short, I promise) T-Cell exhaustion, I will remind my readers of this piece when I publish it.
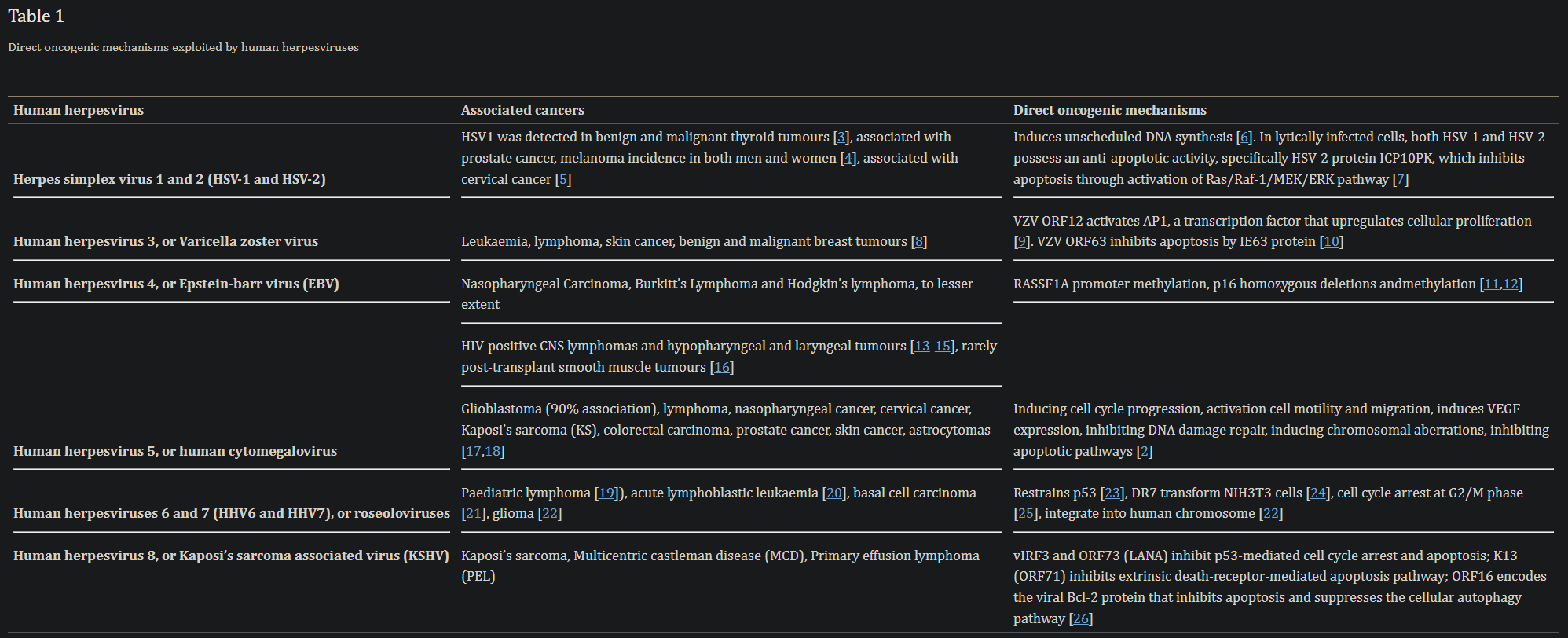
What was discussed and covered here has clear implications not only for Long Covid and ME/CFS, but for the long-term health of a sizable portion of the global population, with severe implications towards cognitive function, and hidden trends towards the massive increase in cancer via, once again, other pathways. And hidden among these are the interactions of SARS-CoV-2 with Endotoxin, its immunological shift, sepsis, and Endotoxic Tolerance.
A “sequel” to this piece is inevitable sometime in the near future. And in case you are worried, I crosschecked most of my suggestions in regards to treating yourself from “Covid After Effects” and it covers and hinders most of the pathways here.

Your support is greatly appreciated.
If you have Long COVID, or you tried many types of supplements and treatments and had some or little improvement you should seriously consider getting tested for herpes viruses such as EBV, CMV and human herpes viruses (HHV).
Coxsackieviruses also play a role in Long COVID and long term dysfunction, and presence of autoantibodies.
Great work here JP! TurboCancer is what resulted in our learning about fenbendazole. Close relative, with no breast tissue from 2009 masectomy, developed metastatic Breast cancer “everywhere” in late 2021 after two moderna covid shots. Lung, bone, kidney, pancreas. At 83, she refused all treatment and went home to hospice care. Nothing to lose so she took fenbendazole (222 mg per day)...available from pet store or amazon. Cancer gone in 4 months, she felt and looked better in 1 month! Read her Case Report at https://fenbendazole.substack.com
No side effects! We don’t have to die from most solid tumor cancers any more! Fenben is cheap, OTC, side effect free antiparasitic medicine that cures...cures! cancer. Even kills cancer stem cells spawned by traditional chemotherapy. It will change your life to know that you can not worry about cancer. Read the Substack, all the science and supporting findings are there. Not selling a thing, not even subscriptions. This is a pay-it-forward effort to help others eradicate their cancers.