


How SARS-CoV-2 Fragments Fuel Long-Term Disease
From Spike to Stroke

In light of recent findings, we shoot straight from the hip today. Fast, direct, and to the point, as I continue to write my ever-encompassing and growing Cognitive Strike Part II. To start, something I have been writing and covering recently, the ever-lasting nature of SARS-CoV-2 fragments.




Measurement of circulating viral antigens post-SARS-CoV-2 infection in a multicohort study
Methods
Plasma and serum samples were collected from adults participating in four independent studies at different time points, ranging from several days up to 14 months post-SARS-CoV-2 infection. The primary outcome measure was to quantify SARS-CoV-2 antigens, including the S1 subunit of spike, full-length spike, and nucleocapsid, in participant samples. The presence of 34 commonly reported PASC symptoms during the postacute period was determined from participant surveys or chart reviews of electronic health records.
Results
Of the 1569 samples analysed from 706 individuals infected with SARS-CoV-2, 21% (95% CI, 18–24%) were positive for either S1, spike, or nucleocapsid. Spike was predominantly detected, and the highest proportion of samples was spike positive (20%; 95% CI, 18–22%) between 4 and 7 months postinfection. In total, 578 participants (82%) reported at least one of the 34 PASC symptoms included in our analysis ≥1 month postinfection. Cardiopulmonary, musculoskeletal, and neurologic symptoms had the highest reported prevalence in over half of all participants, and among those participants, 43% (95% CI, 40–45%) on average were antigen-positive. Among the participants who reported no ongoing symptoms (128, 18%), antigen was detected in 28 participants (21%). The presence of antigen was associated with the presence of one or more PASC symptoms, adjusting for sex, age, time postinfection, and cohort (OR, 1.8; 95% CI, 1.4–2.2).
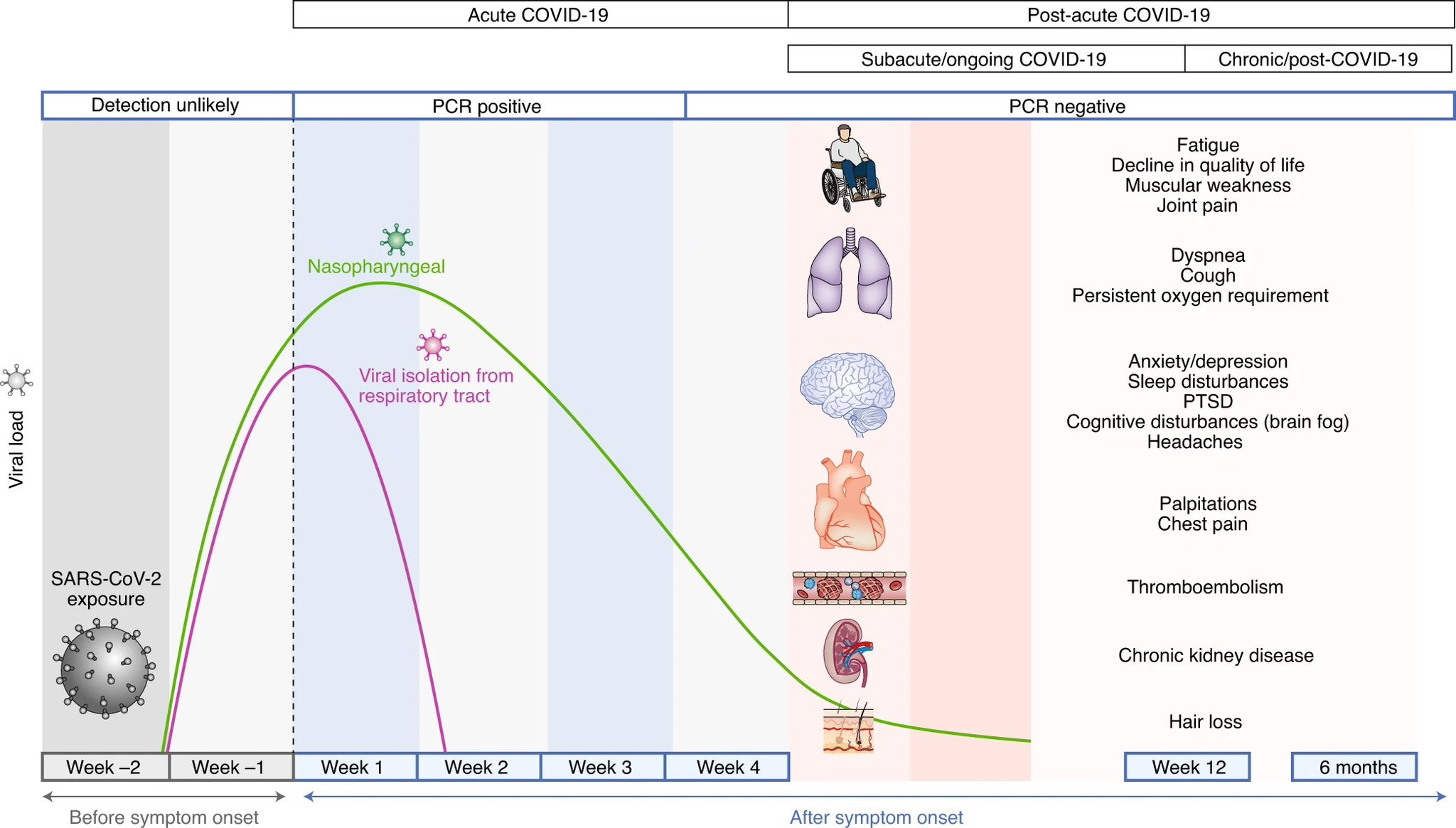
One of the most important underlying subjects of my research, since early 2020 has been the persistence of SARS-CoV-2 (the virus), but later on given all the non-linear dynamics at play, its fragments. Small little pieces that “glue” themselves with other proteins, with a lot of “odd things” inside the body and persist, sometimes for far too long.
Viral fragment, and especially antigen persistence is not unique to SARS-CoV-2 or other common cold coronaviruses, many influenza strain’s antigens persist for months in specific places in the body. The uniqueness of SARS-CoV-2 comes from persisting in the oddest of tissues.
In line with mounting evidence, both direct and indirect, related to this, the authors found that up to 20 of 706 people had Full Spike, S1 (Half of the Spike Protein), or Nucleocapsid. Out of this, 20% had Spike positive from 4 to 7 months after infection. Lasting symptoms of cardiopulmonary, musculoskeletal, or neurologic were present in over half of the people in the study, and almost half were antigen-positive.
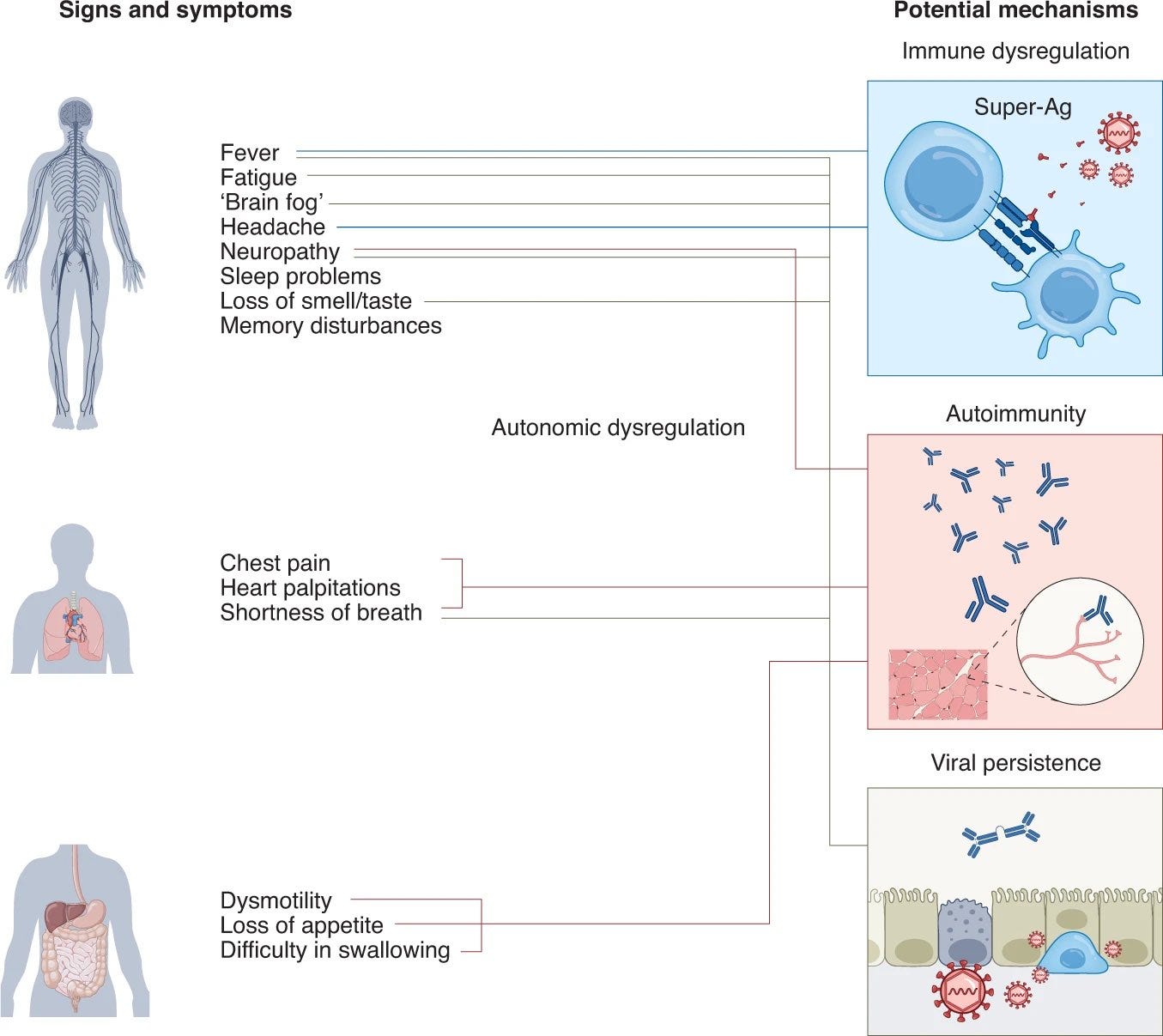
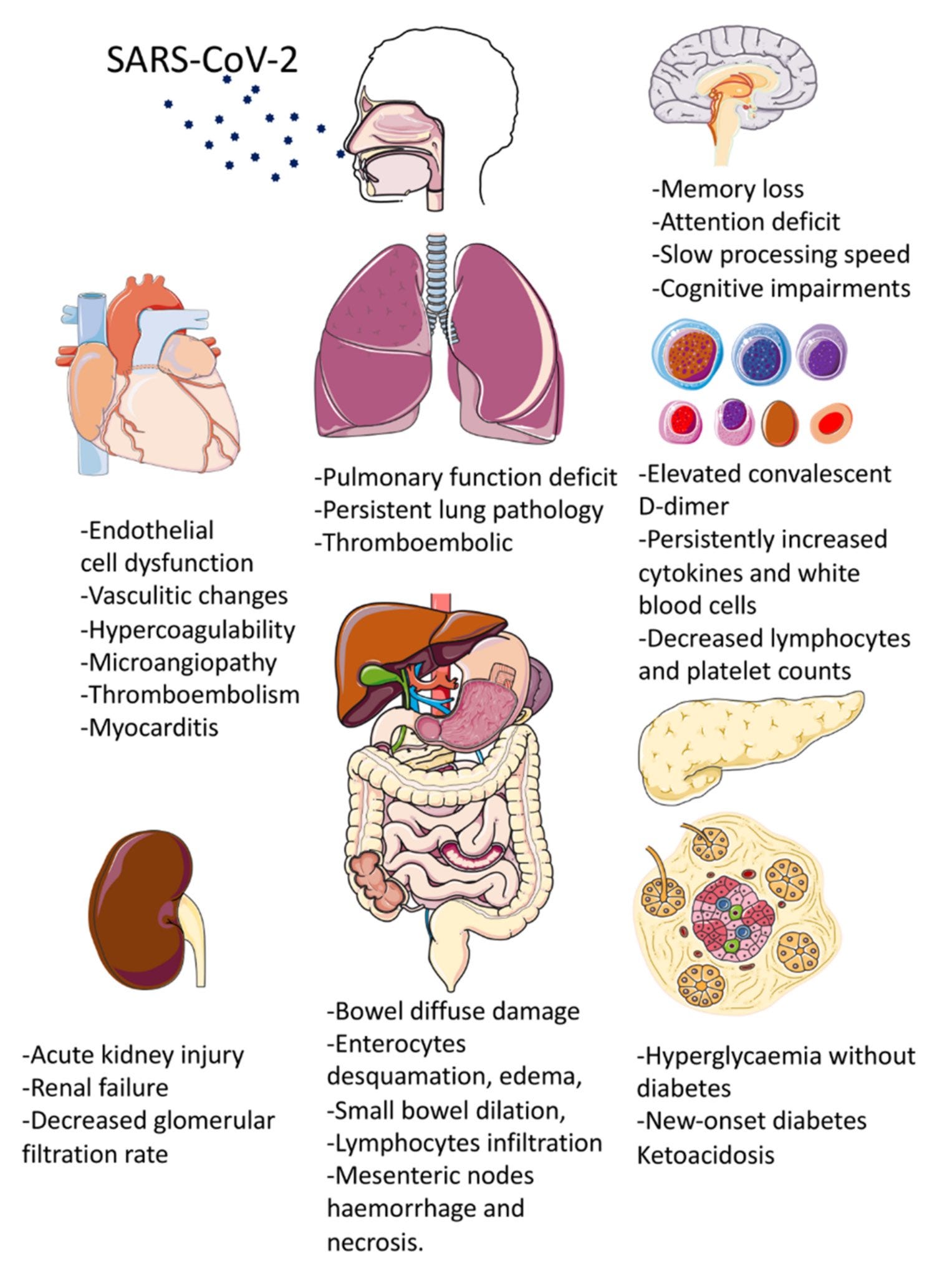
The proposed mechanisms in the images above are also interesting, after many years of waving away the potential for the FCS (an almost perfect analog for one of nature’s most potent toxins) as one of the causes of persisting, lasting dysfunction. The last image speaks for itself…
And of course, the mRNA vaccine also induces the persistence of Spike Protein antigens. It was quite literally one of the selling points, the lasting nature of the protein produced by the vaccines, so “you get a very potent, long-lasting immune response”, blatant marketing lies. The persistence of antigens and fragments not only contributes to long-term inflammation that can last months but also levels of immune dysfunction and of course, damage, per the articles linked above.
We are getting closer, and closer to finding why I specifically named SARS-CoV-2 a “Neo Polymorphic Toxin”, emphasis on polymorphic. Even the unvaccinated will have persistent remnants for weeks, which contributes to many of what my last articles covered, especially long-term. What this and all other studies will take years to point out is the cumulative, subclinical damage after each “Mild Omicron infection bro”.
Leading to the next one.


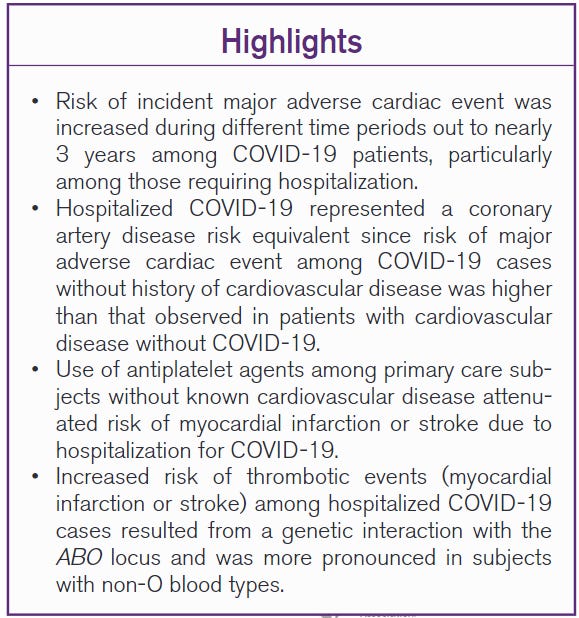
A large study using the UK biobank and thousands of cases, the authors found a similar trend to other large studies. Having Covid alone already increases your chances of having Coronary Artery Disease risk (reduced blood flow to the heart) regardless of severity, but being hospitalized for Covid quadruples your chances, and these help you develop myocardial infarction, strokes and increase all-cause mortality.
The biggest finding in this paper is that a group of patients without known cardiovascular disease had compared or even higher risk of of major cardiac events. A simple reason to explain this is that your heart is a muscle, and people with known heart disease become “more resilient” to the changes, and people without it, are more susceptible. That is why doctors will say if you have a heart attack, have one after the age of 40.
The study cut-off was 3 years, and up to 3 years your risk increases. The bitter irony here is the fact that it is pretty “easy” to separate vaccine-induced cardiac events from viral infection-induced, especially by age. The younger you are, your likelihood of developing heart damage from vaccine injury increases, also the fitter you are. Fat wants to stay with fat, including LNPs, and if you have little fat, it will seek your heart. Irony resides where out of shape (excess fat), metabolic diseased, and older people avoid this form of vaccine injury.
Missed by both sides is once again what will be named “micro alterations” subclinical (hard to see, hard to diagnose) changes and damage to different tissues and organs that don’t contribute to mortality short-term. But long-term… Also a reminder one of the articles above covers a paper that predicts a “heart disease pandemic” because the virus can create reservoirs in specific heart tissue, and Omicron is becoming a master of immune evasion. A viral IED if you will.
And nothing contributes to both Long Covid, heart disease, and everything in between than alterations in blood flow and lack of oxygen. In fancy medical jargon, Stroke.
Association between SARS-CoV-2 and Stroke: Perspectives from a metaumbrella-review
Methods
A metaumbrella was conducted, which included 34 systematic reviews, of which 4 were selected for the final analysis based on methodological quality and consistency. The analysis aggregated the results of 70 primary studies, considering different stroke subtypes and outcomes associated with COVID-19. Study heterogeneity was assessed using the I² index, and significance bias was verified using Egger’s test.
Results
The analysis showed that the severity of COVID-19 is significantly associated with an increased risk of stroke (eOR = 2.48; 95%CI: 1.55 – 3.95), particularly for ischemic stroke (eOR = 1.76; 95%CI: 1.11 – 2.80) and hemorrhagic stroke (eOR = 3.86; 95%CI: 1.79 – 8.33). Additionally, patients with cerebrovascular comorbidities had higher mortality (eOR = 2.48; 95%CI: 2.48 – 19.63), as did those who had previously suffered a stroke (eOR = 6.08; 95%CI: 3.73 – 9.91).
Conclusion
The association between SARS-CoV-2 and stroke was consistent and significant, suggesting that COVID-19 should be considered a new risk factor for cerebrovascular diseases. However, the high heterogeneity among the studies analyzed reinforces the need for further research to consolidate this relationship.
To the surprise of literally nobody, SARS-CoV-2 has a significant and consistent effect on developing stroke and is a significant risk of developing cerebrovascular diseases, and it is even worse for those who already have diseases in this class, such as any person suffering from neurodegeneration.
I have covered the capacity of the virus and its fragments to induce coagulation, many parts of the virus interact with important protein that participate in the coagulatory cascade, but are you curious to know what contributes the most to stroke, and what impedes proper recovery from stroke in health tissues around the area that suffered damage ?
Capillary damage, and capillary dysfunction. Dysfunction in microvasculature is a well-known and studied phenomenon, depending on who you ask it can be the driver of Alzheimer’s or the cause throughout decades of accumulated damage. Also a very well-documented event in… sepsis. And a few published papers from SARS-CoV-2 such as “Microvascular Alteration in COVID-19 Documented by Nailfold Capillaroscopy”.
The first and last paper covered in this article will be paramount to understanding both the Cognitive Strike one, Part II, and a significant amount of what is to come. And in regards to Cognitive Strike Part II, I leave you with this. See you in the next one.
As always, I am grateful for your support !


PSA - Substack is not sending me email notifications for almost ANYTHING, basically trying to force people to use only the app. So if I miss your comment, or something else, that is the primary reason. Will try to be more attentive, but I don't like the app, the algorithm here is atrocious for my taste.
That is just one image, there are many others who are now witnessing around them and at large. And there will be a large number of you who will live on denial until it hits you in the face (or the brain).