
Spike Protein accumulation in the brain
Long-term inflammatory cascades

Given the contents of this piece, especially after this recent study that is merely confirming many of the observations made by a lot of folks over the last 3 years, I will first share the “answer” to what we will discuss in regard to the paper, not the news article.
As an FYI, you must add serrapeptase if you want to degrade Spike Protein, Serra unlike the other enzymes, is systemic. You can read more of my thoughts behind how to deal with Spike Protein in the Substack below.

It is no secret one of my main focuses while covering, researching, and attempting to solve pieces of this puzzle, was, and still is the brain. And one argument I had since mid-2021 given what we knew back at the time was that SARS-CoV-2 was a disease accelerator, which a dear friend named “The Great Accelerator”. And while at that, I also tweeted this.

COVID-19 Infection Accelerates the Progression of Dementia

Summary: Following COVID-19 infection, all subtypes of dementia, irrespective of a person’s previous dementia type, behave like rapidly progressive dementia.
Infection with SARS-CoV-2 has a significant impact on cognitive function in patients with preexisting dementia, according to new research, published in the Journal of Alzheimer’s Disease Reports.
Patients with all subtypes of dementia included in the study experienced rapidly progressive dementia following infection with SARS-CoV-2.
“Based on the progression of cognitive deficits and the association with white matter intensity changes, we propose a new term: ‘FADE-IN MEMORY’ (i.e., Fatigue, decreased Fluency, Attention deficit, Depression, Executive dysfunction, slowed INformation processing speed, and subcortical MEMORY impairment).”
“As the aging population and dementia are increasing globally, we believe pattern recognition of COVID-19-associated cognitive deficits is urgently needed to distinguish between COVID-19-associated cognitive impairments per se and other types of dementia.This understanding will have a definitive impact on future dementia research,” Dr. Souvik Dubey concluded.
“Increasing epidemiological evidence of the association of COVID-19 and AD is the heightened risk of AD with COVID-19, and of increased COVID-19 in patients with AD points to shared pathogenesis.Dubey et al further clarify this connection in demonstrating COVID-19 fundamentally alters the course of dementia no matter the cause,” remarked George Perry, PhD, Editor-in-Chief, Journal of Alzheimer’s Disease, and Semmes Distinguished University Chair in Neurobiology at The University of Texas at San Antonio
The caption in the image from the news article is what we call foreshadowing in some ways.
The complexity of interactions of the virus and its Spike Protein with many of our important functions, its protein mimicry, these interactions were bound to accelerate many forms of pathologies, while I have a certain level of bias on the overall causative dynamic, there isn’t exactly only one, besides most of the long-term damage being mediated by different sections of the nasty Spike Protein. One reason I call the Spike Protein “The Sistine Chapel of Synthetic Biology”. If a lot of the damage is mediated by the Spike Protein, it is of no surprise that anything using the Spike as an immunogenic target would inevitably have similar effects.
The following paper is rather significant to the long-term health of many.
SARS-CoV-2 Spike Protein Accumulation in the Skull-Meninges-Brain Axis: Potential Implications for Long-Term Neurological Complications in post-COVID-19
The spike protein has been shown to affect endothelial function in vitro24–26 and in vivo27,28 and induce TLR2- mediated inflammatory responses in vitro after intraperitoneal injection in mice29, but whether such responses can also be observed in patients has not been thoroughly investigated. However, the long persistence of the spike protein has been shown in the patient’s immune cells (at least 15 months)30 and in the patient’s blood plasma (at least 12 months in a preprint)31. Radiolabeled free spike protein has been shown to cross mice’s blood-brain barrier and enter the brain parenchyma32 . However, due to the limited resolution of the methods employed, the exact routes of spike protein entry to the brain, their targets, and molecular changes associated with spike protein accumulation in brain tissue remain largely unclear33,34 .
Here, we used optical tissue clearing to identify all tissues that accumulated SARS-CoV-2 spike protein in mice and investigated the distribution of spike protein in post-mortem samples from COVID-19 patients. We also characterize the protein expression consequences of SARS-CoV-2 infections in different skull tissues from post-mortem human samples with mass spectrometrybased proteomics. We found an accumulation of spike protein in the skull marrow niches, recently discovered skull-meninges connection (SMC)35–40, meninges, and the brain parenchyma in both mouse and human samples. The human proteomics data showed dysregulation of complement and coagulation cascades, neutrophilrelated pathways, and an upregulation of pro-inflammatory proteins. Injecting spike protein to skull marrow niches directly in healthy mice triggered proteome changes and cell death in the brain parenchyma. Surprisingly, we identified lingering spike protein in the skull samples of a subset of individuals who recovered from COVID-19 and died due to non-COVID-related causes. Thus, accumulation of SARS-CoV-2 and spike protein at the CNS borders can contribute to changes in the brain, suggesting a possible mechanism for the neurological effects of SARS-CoV-2 infection.
To properly understand everything we are about to discuss, it is better to elucidate some points, both raised by the authors and previously covered here and elsewhere. Each portion of the Spike protein (SP from now) can bind and engage different cells and elicit different signals, so it can both trigger TLR (Toll Like Receptors) 2 and 4 being the main ones, TLR4 is arguably one of the most important in regards to the overall pathology of the virus, 2 is often correlated to neurological sequelae. Other authors also found that the SP could trigger TLR 7, and 8.
The authors cite two papers I covered months ago in which scientists found a persistent presence of SP, especially in people afflicted by Long Covid, the persistent presence of viral fragments is argued by many clinicians and researchers (and myself for a couple of years now) as one of the drivers of long-term inflammation and persistent immune responses, which causes different types of damage. Another point raised is the fact that free Spike (not bound/glued to anything) can pass through the Blood-Brain Barrier and induce damage.
The second paragraph can be easily explained by the following image.

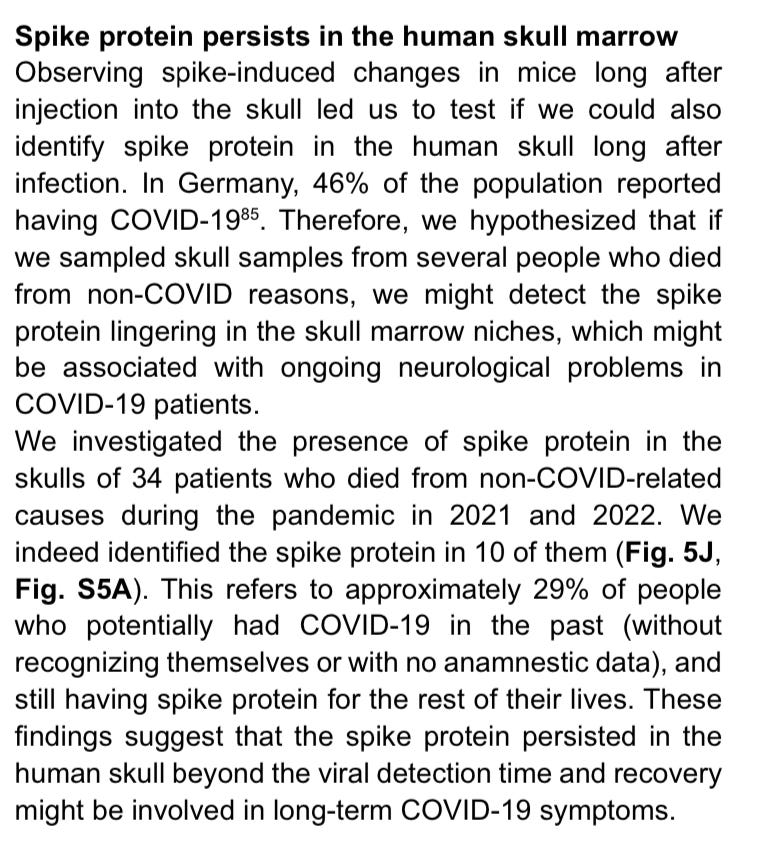
The remarkable finding of this paper is the lingering SP found in the brain of people who recovered from Covid, but died from other causes, an argument made by me and many others, persistent inflammatory signaling after Covid caused by improper clearance of viral proteins/fragments would aid damage and death by other causes.
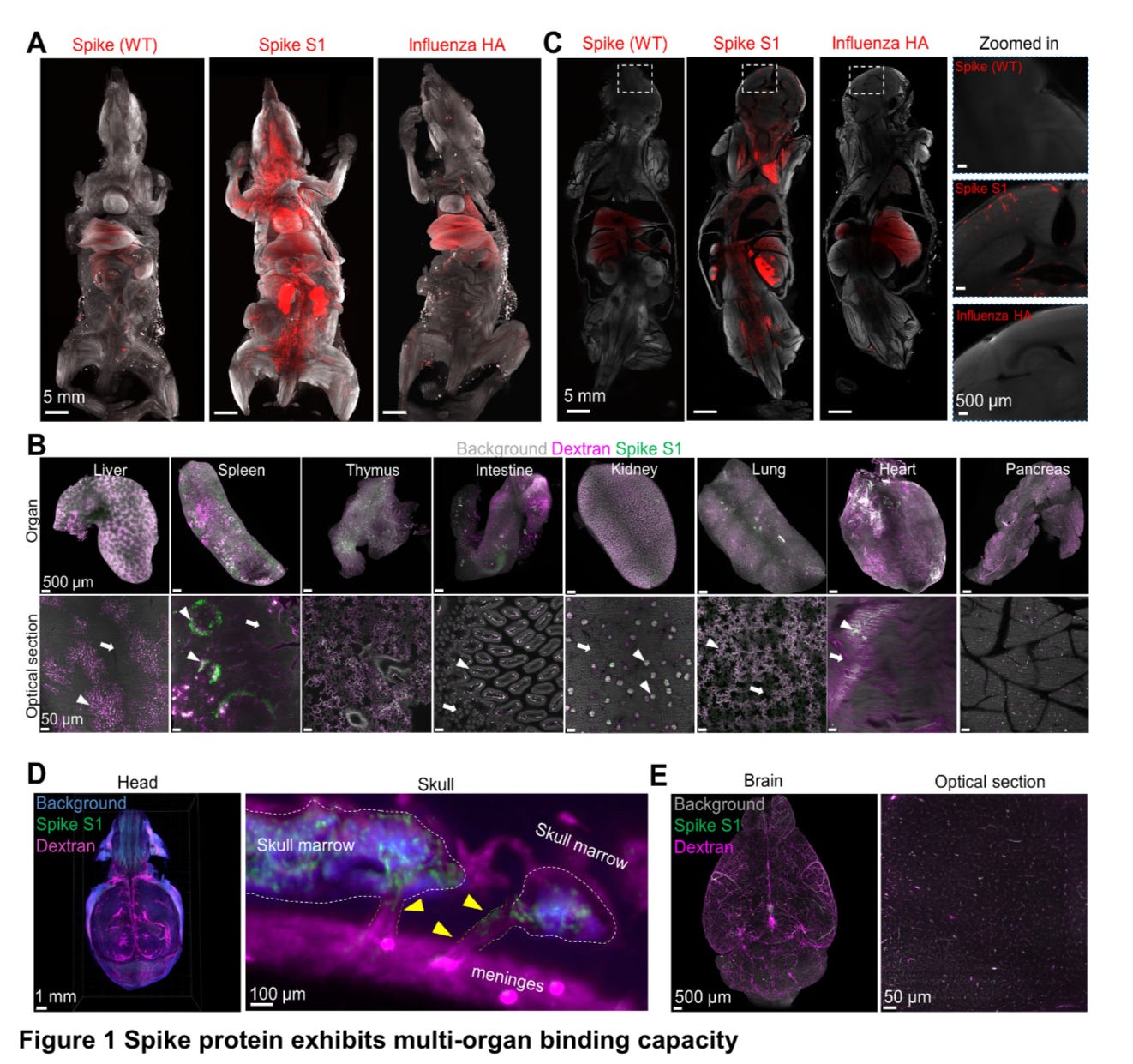
Whole body distribution of spike S1 protein in a mouse model
To test the different binding capacities and avoid bias, they used a mutated Spike Protein, used original Spike (WT) and influenza hemagglutinin (HA). After injecting mice with S1 part of the SP they found the S1 binds to most organs, including the heart, lung, liver, kidney, intestines, thymus (!!!!), spleen and pancreas, while WT and HA had more of a lung and liver preference. In each organ the S1 Spike accumulated closely to blood vessels in he liver, kidney and lungs. Spike S1 was also detected in the brain prefrontal cortex, and substantial S1 accumulation was found in the skull marrow niches (see image above to understand where the skull marrow is in relation to the cranium structure), followed by the authors suggesting that vascular smooth muscle cells (SMCs) may play a role in distributing the S1 protein through the skull, and other potential routes such as phagocytic cells (cells that clean your body from “garbage”) and extravasating from blood vessels, in simple terms, the blood vessel leaking the S1 and it goes floating around. They also found S1 in other marrow bones, such as femur, tibia indicating the S1 travels far, followed by S1 in diverse regions of the brain and spinal cord.
In the presence of S1 protein in the meninges there was a decrease in ACE2 expression, which has severe consequences for the person, from endothelial dysfunction to metabolic dysregulation , bioenergetic loss, among other deleterious effects. Without presence of the virus or viral load but presence of S1, it suggested there is a specific mechanism for S1 delivery into the brain, or a longer half-life of the Spike Protein compared to other viral particles.
While I could cite a dozen of my writings here, I don’t see the need, but I do see the need to vindicate the author’s of the paper covered in this substack, a paper widely ignored and to this one of that I hold as one of the most important ones. And the following one, within the subject of stem cells in regards to infants and mothers, finally culminating in the one below, of long-term importance to almost every human being on the planet as of right now.
The persistence of viral fragments anywhere means persistent immune activation at different levels (from low-grade to severe inflammation), which is both a mechanism for immune exhaustion, autoimmunity in said regions, and further degeneration of cognitive health.
Author’s next step was the profile of protein expression (proteomics) of SARS-CoV-2 patients in the skull marrow, meninges and brain samples, in the skull marrow 496 proteins were unregulated and 159 were down regulated, and the starting finding was that other coronavirus entry factors (meaning the receptors the virus uses to hijack many cell types) were unchanged, Neuropilin 2 (NRP2), Dipeptidyl Peptidase 4 (DPP4, CD26), Basigin (BSG, CD147), Alayna Aminopeptidase (ANPEP, CD13), and Cathepsin B (CTSB). As a personal remark, I HATE how they give a dozen different names for the same protein, makes like much harder.
Further analysis found what one would expect, the same proteins involved in SARS-CoV-2 infection were unregulated in the skull marrow. Per the words of the authors themselves:
The most strongly dysregulated part of the immune system was the complement system, which was previously reported to be activated in COVID-19. High-severity infection of COVID-19 is often associated with hyper activation followed by exhaustion of the complement proteins such as C3 and C4. Indeed, we found significant downregulation of complement components C1, C4, C5, C8 and factor H in the skull marrow of these non-survivors COVID-19 patients and decreased coagulation factor XI expression.
Here is a very brief explanation of the complement system. I will attempt to leave this section as it is, but exhaustion of certain parts of the complement system, with higher levels of certain proteins are found in certain neurodegenerative conditions. One of the proteins of interest to serve as a bio marker for such changes is Galectin-3… Galectins themselves play a significant role in the complement system. Among the myriad of inflammatory changes leading to accumulation of neutrophils, certain proteins involved in the damage of the infection were also found, such as High Mobility Group Protein B1 (HMGB1) and Heat Shock Protein HSP 90-Alpha (HSP90AA1), proteins that when present in abundance lead to coagulopathy.
Further pathway and protein analysis lead to impactful findings, such as the aforementioned HSP90AA1 protein being unregulated in the skull and meninges, and the peculiar finding of S100A8/A9 being over expressed in the meninges too, the protein S100A8/A9 (these are two different proteins, one ending with A8, the other A9, belonging to the same family) is knows as a essential starter for pro inflammatory reactions and its role in neutrophil migration. Extensive discussion among clinicians and researchers can be easily found in social media on the role and significance of both proteins in regards to SARS-CoV-2. These finding that neutrophils might move to the meninges, induce NETs formation and trigger inflammatory responses. Neutrophils are a major cell population in the skull marrow. The following paper is a extensive and comprehensive overview on NETs, how they form, work, and its double-edge nature.
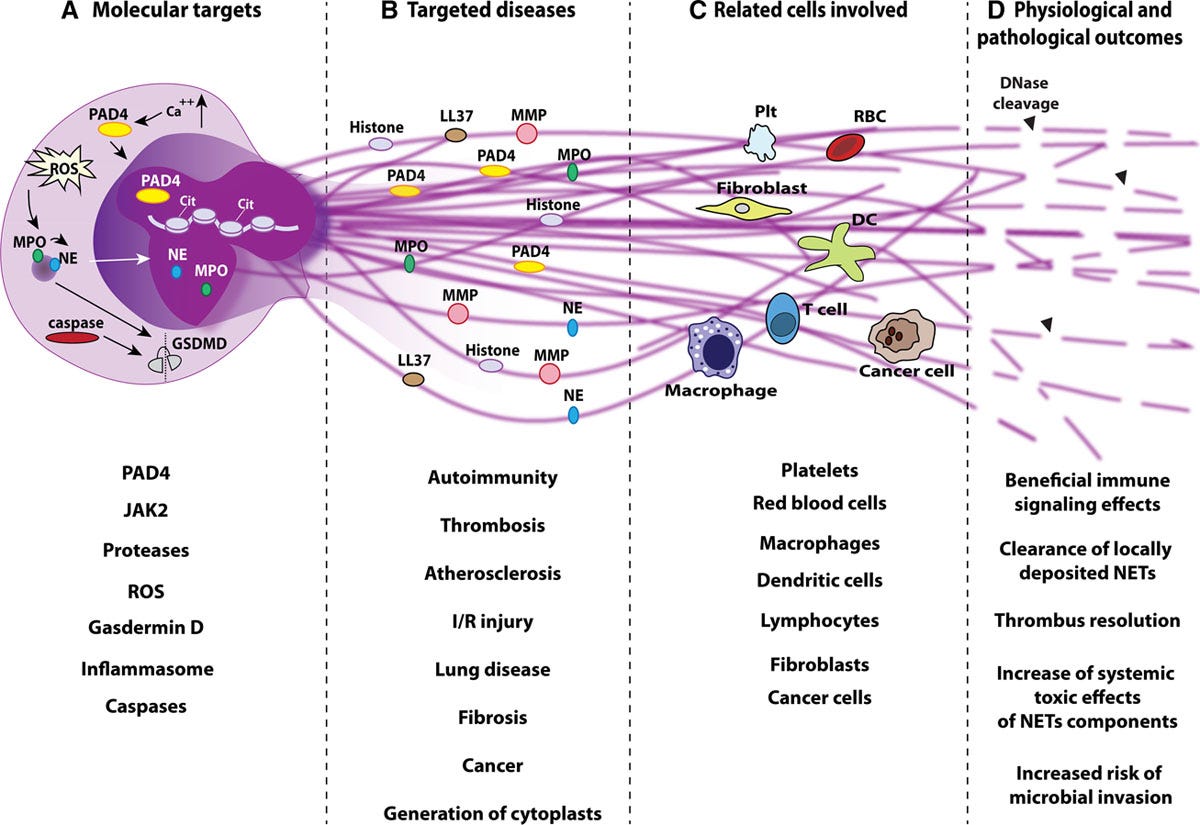
A good point the paper above raises is the mechanism by which NETs are formed and consistent with research, it is often inflammasomes, the same mechanism by which the Spike (coincidentally the S1 part) induces many inflammatory effects in different cells, and once more we go back to Endotoxins, LPS can induce NET formation pretty strongly by a mechanism that is shared by Galectin-3. In a short summary, via multiple mechanism the S1 can induce not one, multiple multiple, long-term inflammatory loops (we vulgarly call them among our circle of friend as doom loops), and stopping the signaling and mitigating the damage is paramount for long-term health and avoiding the body last resort towards long-term inflammatory signaling, that being autoimmunity.
The author’s go into further detail and investigation to elucidate all the different mechanism by which the S1 could elicit changes and potential damage in the many different regions of the cranium/brain, and to summarize the data, S1 in the blood alone can trigger protein changes, therefore inflammatory cascades in the skull marrow, meninges, and the brain cortex. S1 that is “stuck” (persistence of S1 in the region) in the skull marrow leads to long-term increased expression of certain proteins, the most important being caspase 3 (a marker for cell death) and APP (Amyloid Precursor Protein), a well recognized marker for brain injury among many other pathogenic effects, the long-term presence of S1 causes long-lasting pathological effects, this is effectively one of the mechanisms for accelerated neurodegeneration, worsening of multiple times of nervous system and brain diseases.
Besides all of the discussed significant changes in multiple regions of the brain, one remarkable finding to me, that goes above these changes that are often correlated with acute/severe infection (it is not that easy for Spike Protein and S1 to reach the brain, only in a certain but significant percentage of people naturally infected) was the dysregulation of NDUFA2 and 3 in any region of the brain with Spike present. These are mitochondrial related and the decrease or dysfunction severely affect mitochondrial function and cause significant oxidative stress. As a dear friend often said, “It is all about the mitochondria”.
I will let the last section of the paper speak for itself.
Do you know what a lot of the proteins, and pathways and mechanism we discussed in this entire piece have in common ? They create specific immune responses inflammatory loop all ending up with the same subclass of T Helper cells. A Th17 response.
And since I know I have some very strict scientifically minded readers (among a few doctors, researchers, scientists), the authors mention TLR2 as one of the receptors that can induce these responses.
To further drive my point, 3 substack directly related to Th17 responses and the virus/mRNA.
Organ rejection after vaccine, Further evidence on the Th17
Vaccine induced Th17 response - Further evidence for paradoxical immune response
And as the last one.
Pardon my crude language, but in regards to Th17, I will die on this fucking hill.
Give me a few days and I will write something about NETs and how to mitigate it, otherwise everything I wrote so far, especially in the pinned Substack with many other Substacks linked inside, titled “Things Hidden series” stands.
If you chose to support my work thank you, it helps me build this endeavor.
This substack was complex as it is, so I decided to end it where I did, otherwise I would get severely more complex, at least I connected with older pieces so reader can dive into further context and understand how far this rabbit role goes.
Tomorrow post has science is the name and source but it is about propaganda.
Happy Easter to all of you =D !
Excellent review John.
Consequences becoming apparent now😵💫