

As an odd accident by fate, many significant papers were published in late December, and they all are somewhat… well, bad, negative, but from a purely scientific perspective, significant. All of the next few articles will be interconnected, but I will publish them separately, for better comprehension. I will refer to many other articles I’ve written too.
As I wrote a couple of weeks back, we would hit the ground running. One of my earliest and longest-running propositions has been both the stealth factor and the persistence of SARS-CoV-2, even in March 2020 I was already voicing my concerns.
To our luck, the first 4 strains (Wuhan to Delta) were so aggressive and so “toxic”, that viral persistence only happened in a strictly small group of people. Mostly it is a byproduct of acute infection with failure of proper immune response or severe (ICU) infection, a byproduct of cytokine storm and immune paralysis. A tiny percentage of immune-compromised people were also able to harbor the virus for long periods (weeks to months).
While I now have an Index article, I will refer back to some Covid persistence articles.





Before we go any further I want you to bear in mind that SARS-CoV-2 uses a lot of other receptors. This will be really important soon, especially regarding the following.
The paper below has many fascinating microscopy videos of their research, if you are interested or curious I highly recommend you to watch them. It is a cell-based study, so there isn’t any “gore” as often is the case with any cardiology-related content (one of the best ways to understand the heart is quite literally seeing it…)
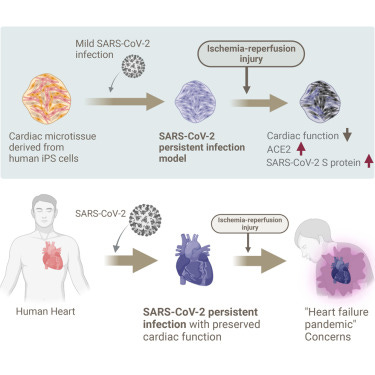
Predicted risk of heart failure pandemic due to persistent SARS-CoV-2 infection using a three-dimensional cardiac model
Highlights
Persistent SARS-CoV-2 infection model of human cardiac tissue was established
Hypoxic stress to the persistent infection model led to cardiac dysfunction
ACE2 and SARS-CoV-2 S protein expression were elevated after the hypoxic stress
One of the biggest points of contention between both sides of the conversation (pro vs anti-vaccine, with their little narrative conflicts) has been if, how long, and “how much” could SARS-CoV-2 cause heart disease or damage to the tissue. One side minimizes the clear effect of the many components of the mRNA vaccine in inducing different forms of heart damage, and the other minimizes that the virus could, in fact, cause subclinical heart damage. Both end up contributing to cardiac incidents throughout life.
Both mechanisms for disease are undisputable by now from my assessment. The authors even refer back to recent research of biopsies from idiopathic chronic cardiomyopathy studies (idiopathic is jargon for unknown, “I don’t know where it came from”) where researchers found viral genomes inside, indicating that viral infections play a role in this particular form of heart disease.
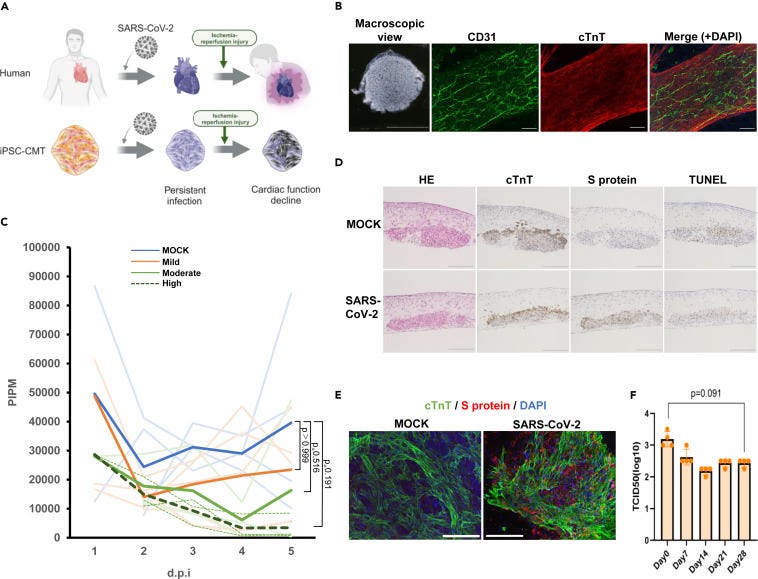
Establishment of SARS-COV-2 persistent infection model using human iPS cell-derived cardiac microtissues
Here the authors used stem cells to create something very close to cardiac microtissue, this CMT is composed of cardiomyocytes and other cell components, and they mimic the heart itself pretty well, including the vasculature (very important). Once again and somewhat importantly, this was using the original strain, not the current ones, I will get back to this later.
7 days post-infection (d.p.i. in many of these papers), all levels of infection, mild, moderate, and severe (high titers) showed deterioration of function compared to the non-infected cells. This means that the viral infection leads to less heart contraction. Mild and moderate showed a recovery trend towards day 28, but severe (high) did not, and a sustainable decrease in contractility was observed, in simple words, impaired heart function.
Analysis of the CMT tissue with mild titers showed expression of Spike Protein inside cardiomyocytes at 28 d.p.i., but no the cells didn’t go through apoptosis, the protein complex in heart muscle cells was maintained, this means that the virus (or Spike Protein) didn’t increase the rate of cell death or the heart cells were still able to function.
Endothelial cells also had partial persistent infection, meaning the infectivity is maintained and can spread at a molecular level (it doesn’t mean it will spread throughout the entire body suddenly, it will be localized), and vascular network formation was slightly compromised only when Spike Protein and CD31 (a marker for these cells) was detected. Vascular Network Formation, also called vasculo or angiogenesis is when the body creates new blood vessels. Important for transporting nutrients, and oxygen, removing waste, and supporting function.
This means mild infection can cause persistent infection of cardiac tissue without causing functional impairment. This will be a trend with many other aspects of the long-term consequences of this virus.
Next, they went to test the dynamics of the persistent infection.
Hypoxic stress under persistent SARS-COV-2 infection causes cardiac dysfunction
Since the experiment so far showed that a portion of the population mildly infected with SARS-CoV-2 could have developed a small level of cardiac dysfunction, and the body compensates for global cardiac function by other means (thus the person doesn’t suffer from heart failure) they next wanted to validate the hypothesis. In their words “However, such patients would be at marginal risk of heart failure and could opportunistically develop cardiac dysfunction and eventually heart failure under additional cardiac stress”
To do this they mimicked an ischemic heart disease, when the blood flow to the heart and tissue is compromised, thus leading to lack of oxygen (hypoxia). The hypoxia was done for 18 hours followed by normal oxygen levels for 48 hours. In the non-infected cells, recovery of total function was observed. But in the persistently infected CMT, the function (pulsating and contraction) didn’t increase.
Hypoxia leads to an increase of intracellular ACE2 in cardiomyocytes, with evidence of the co-localization of cTnT and Spike Protein being facilitated by it, thus indicating intracellular reactivation of SARS-CoV-2. Viral titers did not increase, meaning exactly what I described before, that this is effectively something that occurs only inside the cell, restricted to that “section” of the tissue. However, during this low-oxygenic state, vascular network formation was globally fragmented in the persistent cells, indicating that the reactivation of the virus contributed to the deterioration of the infected CMTs.
They close their research by measuring the level of inflammatory proteins during the hypoxic stress under the persistent infection model and found that the levels of IL-6, TNF-α, and IL-1β did not increase under hypoxic stress in the context of persistent infection, and IFN-γ was also below the detectable level. In this particular model, it means the reactivation doesn’t increase the level of inflammatory proteins.
Are the findings of this paper significant ?
Absolutely. But there are caveats, and credit to the absurd honesty of the authors, which themselves stated that this model lacks the “complexity” of a complete model or a human being, and a more complex model would lead to a better and deeper understanding of the finding here.
But by no means does it invalidate their research, it is a massive step toward a much-needed direction. Unlike many other cells such as Lymphocytes (such as T cells), which die when infected by SARS-CoV-2, we always suspected other cells and tissue would simply harbor the virus.
This is extremely significant because of something I described and forecasted months ago. Omicron subvariants are highly immune evasive, and they were always mutating towards higher and higher replication efficiency, but nothing, especially in biological systems can grow forever. I wrote the virus would soon choose to lower its own infectivity and as a trade-off mutate towards more evasion and persistence. And this is exactly what happened with JN.1, the current dominant variant.
The mix and match of immune responses (vaccines only, natural infection only, and then both) created the current variants. SARS-CoV-2 will now attempt (and achieve given my observations and notations) towards persistence. It is shedding ACE2 preference, but it literally uses a dozen other receptors, all expressed in multiple organs. ACE2 is just its preferred (easier) way to get inside cells.
Should you be worried ? Once again, yes and no. As I wrote in my Twitter for the couple of days I reactivated it, you have a few choices. You need to take care of your health year around, get infected once a year (twice tops, and at 2 times per year you need to be aggressive in the supplementation post-infection), so you are “immune” towards most of the variants that year.
Avoiding an infection for too long, given all recent clinical and published research is an assured way towards severe infection and potential hospitalization. If you take care of your health, most likely you won’t even develop symptoms from your infections.
The findings in this paper in particular are very significant because all the next articles I will publish contribute to understanding this paper and the findings here, and somewhat persistence itself.
To the second and rather intricated paper.
Prolonged existence of SARS-CoV-2 RNAs in the extracellular vesicles of respiratory specimens from patients with negative reverse transcription-polymerase chain reaction
This one will be shorter. Here the authors wanted to test the presence of virus inside extracellular vesicles (EVs, imagine very small cells that are created from normal, bigger cells), and the group of patients here were patients with and without Chronic Liver Disease (CLD).
In short, 85% of the patients who tested positive for the virus had the virus present in their EVs, the viral load was much higher in the nasal swabs than in the EVs. Even after patients tested negative for COVID-19, the virus persisted in the EVs. On day 7, 46.9% of patients who tested negative still had the virus in their EVs, and on day 14, 28.6% of patients who tested negative had the virus in their EVs.
At days 7 and 14, the viral load in the nasal swabs decreases but not in the EVs. The viral load was much higher and higher for longer in the EVs of CLD patients than people with only Covid. People suffering from chronic liver disease also had higher markers for cellular damage in both endothelial cells and hepatocytes, than people with just Covid. Remarkably, the study found that the EVs containing SARS-COV-2 RNA could infect cells in a cell line (Vero E6) at 24 hours post-infection.
The size and concentration of the EVs didn’t differ from Covid and Covid+liver disease.
Conclusions
Although this study is not directly related to liver disease, the identification of SARS-CoV-2 in EVs is a highly important and relevant to COVID-19 infection in liver disease patients and for better management of these patients. The identification of SARS-CoV-2 RNAs in the EVs isolated from patients with negative RT-PCR indicates the persistence of infection and likely recurrence of the infection, which suggests another route of transmission as EVs harbor SARS-CoV-2 RNAs. Therefore, in the case of COVID-19 where we are unable to understand the mechanism of recurrence or false negativity, we may find the prolonged association of SARS-CoV-2 with EVs, which can easily be detected even in patients with negative RT-PCR. This could pave way for future directions to determine the cause of reactivation and also post-COVID-19 mortality.
A few other new publisher papers are talking about the persistence of the virus in other organs and cells, but they one in particular deserves a singular article, given the complexity. But from my perspective the numerous data points and evidence provided by bright researchers it is almost impossible to deny that SARS-CoV-2 will persist in many places, cause dysfunction and damage, especially long-term, without causing meaningful damage. As described by a few, SARS-CoV-2 might be the world’s most successful Hit and Runner.
Sensitizing many towards secondary, and damaging “anything”. Both papers are also worrying in regards to the mRNA-derived Spike, because these mechanisms will lead to similar Spike persistence, which the body will attempt to deal with, by “pushing out” of the tissue (therefore causing damage and inflammation), or encase in its “natural biofilms”, known as Neutrophil Extracellular Traps and amyloid proteins.
The following will feel somewhat out of place but I guarantee it will make sense after I publish the next few articles. I will be brief given the size of the text so far.
Metformin mitigates insulin signaling variations induced by COVID-19 vaccine 2 boosters in type 2 diabetes
I have been a big proponent of Metformin as a means to both avoid, tackle, deal with, and recover from a myriad of dysfunctions set off by the viral infection or the mRNA vaccine's adverse effects. And Berberine is almost a perfect analog too, if you don’t want or have access to Metformin.
One side-effect of the mRNA common in many vaccinated was insulin misfiring post-vaccination, where many experienced a brief moment of pre-diabetes, which I suspect they already were on the verge of pre-diabetes, or worsening symptoms and glucose control when they were diabetics.
Contrary to their healthy counterparts in this study, pre and diabetics experience worsening of their glucose control, measured by significant elevation of HbA1c, HOMA-IR (Insulin Resistance test), triglyceride, and triglyceride-glucose index. To understand the inhibitory effect of the mRNA vaccine on glucose control, they went to test in mice. They observed impaired glucose tolerance at dose 4.
Interestingly they found that triglyceride, but not serum insulin or fasting glucose was significantly increased in the mice vaccinated weekly. This means the vaccine can induce insulin resistance rather than impaired insulin secretion. Now you may ask why triglyceride would increase, but there are a few reasons. First, pre-diabetes and uncontrolled Type 2 diabetes are often presented with higher levels of triglycerides, it is the first “stop-gap” your body may go to compensate for the excessive levels of sugar, using very complex metabolic pathways it will convert the glucose into triglyceride. The second, and to be expected and somewhat well observed by now, are certain levels of liver damage induced by the mRNA and its components, especially the LNP.
When testing Metformin effects on mice it alleviated the insulin resistance and rescued the impaired insulin signaling, so Metformin can be used directly to maintain glucose control, and much more from my observations and experience. The authors propose multiple potential mechanisms by which excessive vaccine doses (boosters) can set off these effects and induce Type 2 Diabetes. Interactions with Toll-Like Receptors, Estrogen receptors, persistence of the protein, systemic inflammatory response.
Metformin, one way or the other by a myriad of pathways also helps with all of these and much more.
I appreciate both the patience and the support of my subscribers.
My personal heartfelt message for your 2024.
First I wish everyone a blessed and productive Happy New Year, a good 2024. I think everyone can kinda feel in the air that this will be a rougher year, yet if the horrors persist, so must we.
The next 3 to 4 articles are all connected to this one, and I will write about the mechanisms for persistence too. They are all very significant too, and some were propositions from me and a friend since 2021.
Appreciate the patience, really. I don't like bad vibes in December, at all.
While this article is not “good news” it is really nice to be able to get insight into what we are up against. Thank you so much.