
SARS-CoV-2 role in Tumor Immunity and Immune manipulation
Fight cancer with cancer

Things got a lot more interesting and a hell of a lot more awkward… if you search for the word “cancer” or “oncogenesis” in my Substack, you will be met with many articles, either I am covering the mechanisms by which SARS-CoV-2 and mRNA can induce or accelerate cancer directly, but for the best part of the last 2 years, indirectly. The unseen trends and effects are often what I am looking at.
Also, there is no way I can make this “layperson friendly” while covering the insane complexity of all the different markers used to distinguish cells, the tests, chemicals, and models used, so I will go against my favored approach and simplify it. You can check the paper for all the markers, and etc, I will maintain the most impactful ones and explain them.




An AI-podcast for Galectin-3 and Latent Infections can be listened to below, as a refresher, but it is also great for the layperson.
But not merely of “Cancer inducing” or “Cancer acceleration” is SARS-CoV-2 made of, somehow there are many odd times when the viral infection simply “kills” the cancer. A few examples.
Fourteen cases of remission following viral infections and two after anti-SARS-CoV-2 vaccination
Spontaneous remission of chronic lymphocytic leucemia in a patient with SARS-CoV2 Important overall → (The main effect of SARS-CoV2 is attributed to hyperactivation of T cells.)
The problem is “the how”. The last line in the last bullet point should start activating your implicit pattern matching because very few things hyperactivate T-Cells, and one of them, sought after as a Holy Grail of vaccine research and cancer treatment is…
Staphylococcus aureus enterotoxin B (each word here is linked to a different paper)
The following article is “obligatory” reading, it will have an AI-podcast below =).

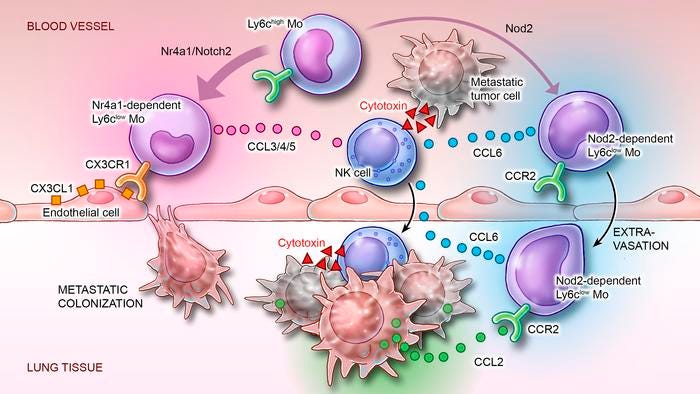
Inducible CCR2+ nonclassical monocytes mediate the regression of cancer metastasis
A major limitation of immunotherapy is the development of resistance resulting from cancer-mediated inhibition of host lymphocytes. Cancer cells release CCL2 to recruit classical monocytes expressing its receptor CCR2 for the promotion of metastasis and resistance to immunosurveillance. In the circulation, some CCR2-expressing classical monocytes lose CCR2 and differentiate into intravascular nonclassical monocytes that have anticancer properties but are unable to access extravascular tumor sites. We found that in mice and humans, an ontogenetically distinct subset of naturally underrepresented CCR2-expressing nonclassical monocytes was expanded during inflammatory states such as organ transplant and COVID-19 infection. These cells could be induced during health by treatment of classical monocytes with small-molecule activators of NOD2. The presence of CCR2 enabled these inducible nonclassical monocytes to infiltrate both intra- and extravascular metastatic sites of melanoma, lung, breast, and colon cancer in murine models, and they reversed the increased susceptibility of Nod2–/– mutant mice to cancer metastasis. Within the tumor colonies, CCR2+ nonclassical monocytes secreted CCL6 to recruit NK cells that mediated tumor regression, independent of T and B lymphocytes. Hence, pharmacological induction of CCR2+ nonclassical monocytes might be useful for immunotherapy-resistant cancers.
Most of this study, and its many detailed sections were done with mice lacking NR4A1, to prove that NOD2 induces a distinct subset of Monocytes. This will be important later on in this article.
To understand this very complex paper, we need some explanations. Monocytes are a type of white blood cell that destroys pathogens and eliminates infected cells. They do this by either “eating” them using antibodies or complement (smaller molecules that assist antibodies) or by employing a process called Antibody-Dependent Cell-Mediated Cytotoxicity, where monocytes call Natural Killer (NK) cells to kill anything tagged with antibodies. Once a monocyte enters tissue, it can transform into macrophages (professional eaters) or dendritic cells (cells that pick up antigens, the “Lego blocks” of immunity, and start the process of activating T cells).
Under specific, healthy conditions, Classical Monocytes can differentiate into Nonclassical Monocytes (NCMs) through Intermediate Monocytes (IntMCs), and this pathway relies heavily on and especially NR4A1, critical to NCM development. These are called Naturally occurring Non-classical Monocytes (N-NCMs) and they possess CX3CR1 which facilitates the capacity of these specialized Monocytes to surveil blood vessels, but lack CCR2 a protein that controls the movement of immune cells and allows these to infiltrate to infiltrate tumors (thus these can’t infiltrate tumors outside blood vessels).
In contrast, the authors discovered a unique subset of monocytes called Inducible Nonclassical Monocytes (I-NCMs). These cells, unlike N-NCMs, express high levels of CCR2 and MHC II, enabling them to infiltrate tumor sites and present antigens to other immune cells. MHC II acts like a Lego piece carrier, presenting fragments to initiate a T cell response. By treating mice with muramyl dipeptide (MDP), a mimic of bacterial cell walls and a potent NOD2 activator, the authors significantly boosted the population of I-NCMs. Remarkably, this process occurred even in mice lacking NR4A1, proving that I-NCMs arise through a distinct pathway.
To explore the genetic differences between I-NCMs and N-NCMs, the researchers used bulk RNA sequencing to analyze gene expression. They found higher levels of S100 genes, which act like alarm signals and help cells migrate to injury or tumor sites. I-NCMs also expressed MMP12, an enzyme that breaks down tissues, allowing immune cells to move into tumor environments. Additionally, these cells had elevated levels of H2-Aa and H2-Ab1, both involved in MHC II antigen presentation, further enhancing their ability to orchestrate immune responses.
NOD2 signaling can be triggered by ssRNA viruses, such as coronaviruses. To test the effects of this on the development of NCMs and if it they could create the subset of I-NCMs the authors isolated RNA from SARS-CoV-2, Influenza A and obtained commercial synthetic ssRNA. Synthetic ssRNA and SARS-CoV-2 ssRNA but not influenza ssRNA increase the numbers of I-NCMs.
NOD2, especially its deficiency has been implicated in the progression of cancer and tumor growth due to failure to regulate inflammation, however, the role of NOD2 in metastasis remains unknown. Mice lacking both NOD2 and NR4A1 had a pronounced increase in tumor seeding and progression of metastasis in the lungs, compared to mice only lacking NR4A1 and normal mice (WT).
Introducing I-NCMs in mice lacking NOD2 (thus they can’t produce these cells) prior to injecting a type of cancer cell suppressed the formation of new pulmonary metastasis. It also significantly reduced the size of the cancer already present. I-NCMs induced by MDP treatment were also able to cause the regression of established lung, breast, and colon cancer in both WT and mice lacking NR4A1 in vascularized sites but not in subcutaneous tumors.
I-NCMs don’t kill the tumors directly, instead, they secret CCL6, a protein (chemokine) that is pivotal to calling Natural Killer cells into specific tissue/places. This pathway bypasses the reliance on adaptive immune responses to fight cancer, which is often suppressed by immunotherapy-resistance cancers. Depleting NK cells negated the antitumor effects of I-NCMs, confirming their synergetic and unique role here. Even without T, B cells, and other immune cells, this pathway could still regress metastasis, therefore it is independent of other immune cells.
The Inducible nomenclature comes from the fact you can use certain substances, either synthetic or natural to “induce” these Non-Classical Monocytes, which have very pertinent and specific receptors that can help fight and reverse cancer in a very unique way. The argument from certain researchers and scientific writers is that SARS-CoV-2 could end up lowering cancer, a point I made several months ago. To be precise:
“We may experience a significant and severe increase in multiple forms of cancers, and in a decade or two, a complete reversal, with cancers suddenly vanishing without anyone realizing “why” ”. Purely hypothetical, yet…
The things hidden in conspiracy
Now while I may cite evidence here, this is entirely a hypothetical and purely, completely theoretical scenario. And layered at that. Entirely in the context of the last few articles, they are necessary to understand the following proposal, especially SARS-CoV-2 and its Spike Protein acting as a Neo-Polymorphic Toxin.
The SARS-CoV-2 Spike Protein contains two distinct regions that mimic one of the world’s most potent immune activators, superantigens. These include the Furin Cleavage Site (FCS) in the S1 subunit and a site at the end of the S2 subunit. The superantigenic properties of these regions allow the virus to bypass normal immune activation by directly cross-linking T cell receptors with MHC II molecules, triggering massive, non-specific T cell activation.
In the context of cancer, this mechanism could theoretically awaken dormant T cells or reactivate suppressed immune environments within tumors (transforming “cold” tumors into “hot” ones), effectively jumpstarting an anti-tumor immune response.
By binding and manipulating LPS, SARS-CoV-2 could drive MHC II upregulation, this enhances the presentation of tumor antigens to T cells, amplifying the immune system's capacity to recognize and fight cancer. LPS is known to make the body produce more MHC II. Since MPD and NOD2 activation lead to the induction of I-NCMs, this Spike Protein-LPS interaction could, quite literally, mimic this pathway and create an independent tumor-fighting immune response.
Severe cases of SARS-CoV-2 possess the hallmark of persistent Monocyte Activation and inducing chronic inflammation, both can deplete N-NCMs over time. Long Covid and severe Covid cases both suffer from low levels of NR4A1. Lower NR4A1 levels could predict classical monocyte’s info inflammation-driven pathways such has I-NCM. By reducing N-NCMs (which are limited to vascular surveillance), the immune system might pivot towards a more aggressive, tumor-targeting phenotype.
Deleting NR4A1 and 2 in T cells literally enhances their anti-tumor immunity and reduces CD8 T-cell exhaustion. Even in B cells, a similar effect can be observed, using a specific therapy targeting NR4A1.
It should be no surprise to anyone that Pfizer pumped millions of dollars internally into researching NR4A1, and I highly doubt this was a research done solely aimed at the receptor, but rather in the context of its mRNA vaccine too. I may revisit the NR4A1 on its own sometime early next year because it is of the utmost importance.
I am left wondering, in the past few days. What were the WIV and the PLA scientists aiming to do with SARS-CoV-2, given the amount of evidence, I now believe more firmly that the virus was at the early stages of developing a truly universal “vaccine”. A vaccine against all diseases that burden the Chinese healthcare system and plague its society.
And perhaps the PLA hand was forced into “leaking” the virus to fight another hidden pandemic, since SEB, and LPS exposure have profound effects on our immune response against Influenza. Sounds crazy, right ? The paragraph above and this one are in regards to some of my Conspiracy Sunday articles.
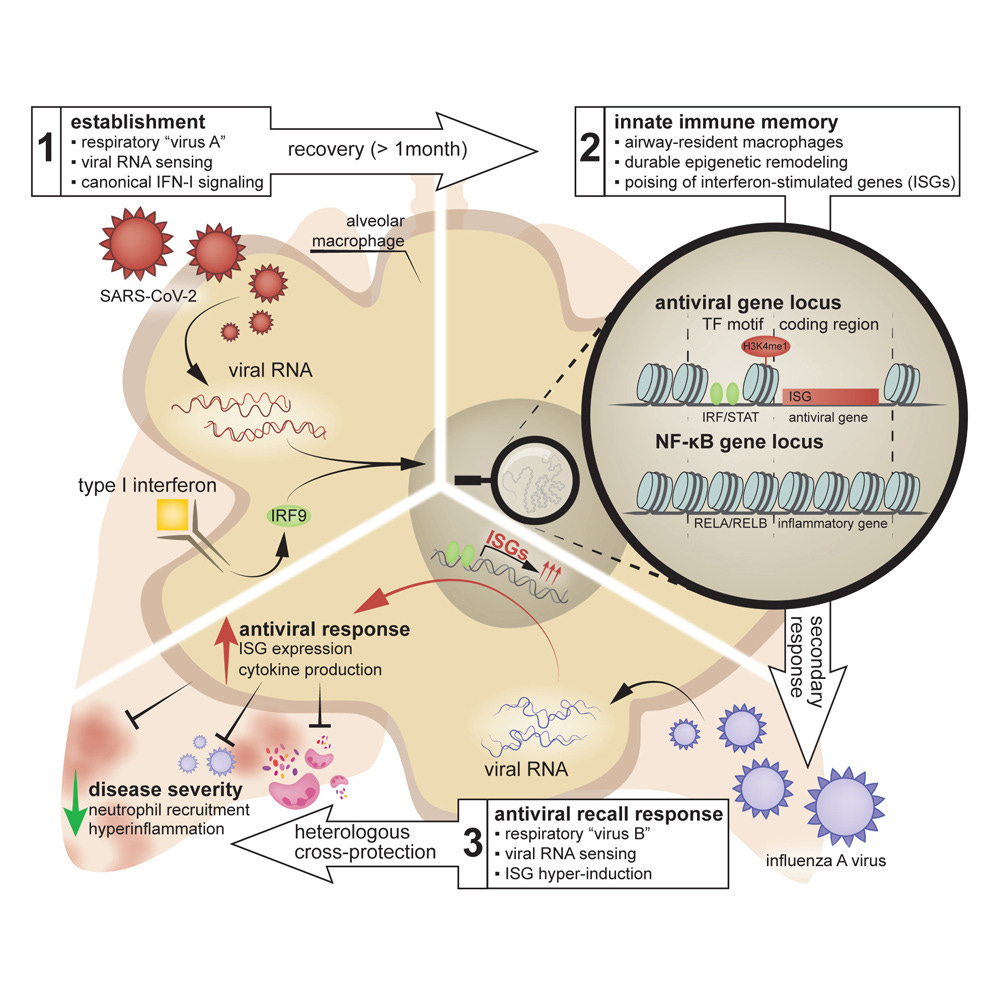
Antiviral innate immune memory in alveolar macrophages following SARS-CoV-2 infection ameliorates secondary influenza A virus disease
It gets crazier from here.
Your support is greatly appreciated and enables me to continue my journey of endless curiosity and boundless learning.

I wish everyone a great week ahead. While I do have a lot to write above, we are getting close to Christmas, so articles may lag, may not.
It depends on the vibes =P.
Holy Toledo! Is there a difference with Omicron vs delta and Wuhan?