

We first start with our developing trend of recombination. The Oncogene post is below. Today there will be 2 SARS-CoV-2 posts, and the second one is even cooler than this one.
Delta-Omicron recombinant SARS-CoV-2 in a transplant patient treated with Sotrovimab
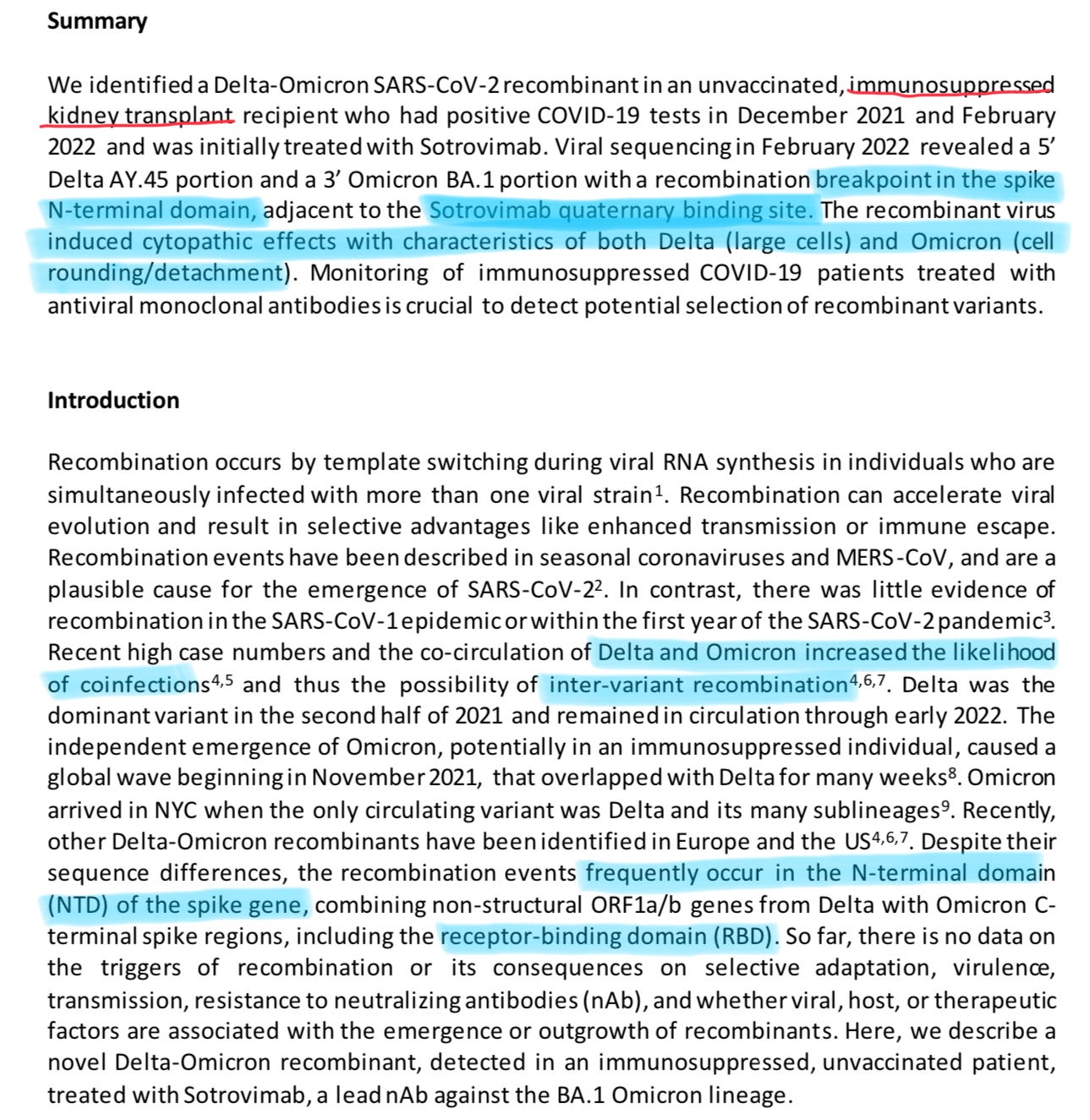
I found this paper interesting for a number of reasons. First, recombination, which is something I am really interested about when it comes to coronavirus, and always wondered where it would lead, in regards to the evolution of SARS-CoV-2.
Molecular genetics doesn’t make it easy for the average joe, or even the average university student to understand, so I will make it easier. The recombination took place in the same spot as the last post. And as pointed out by other researchers, the recombination (this just means different variants trade mutations that are beneficial for the virus) often occurs in the N-Terminal domain, and sometimes near the RBD.
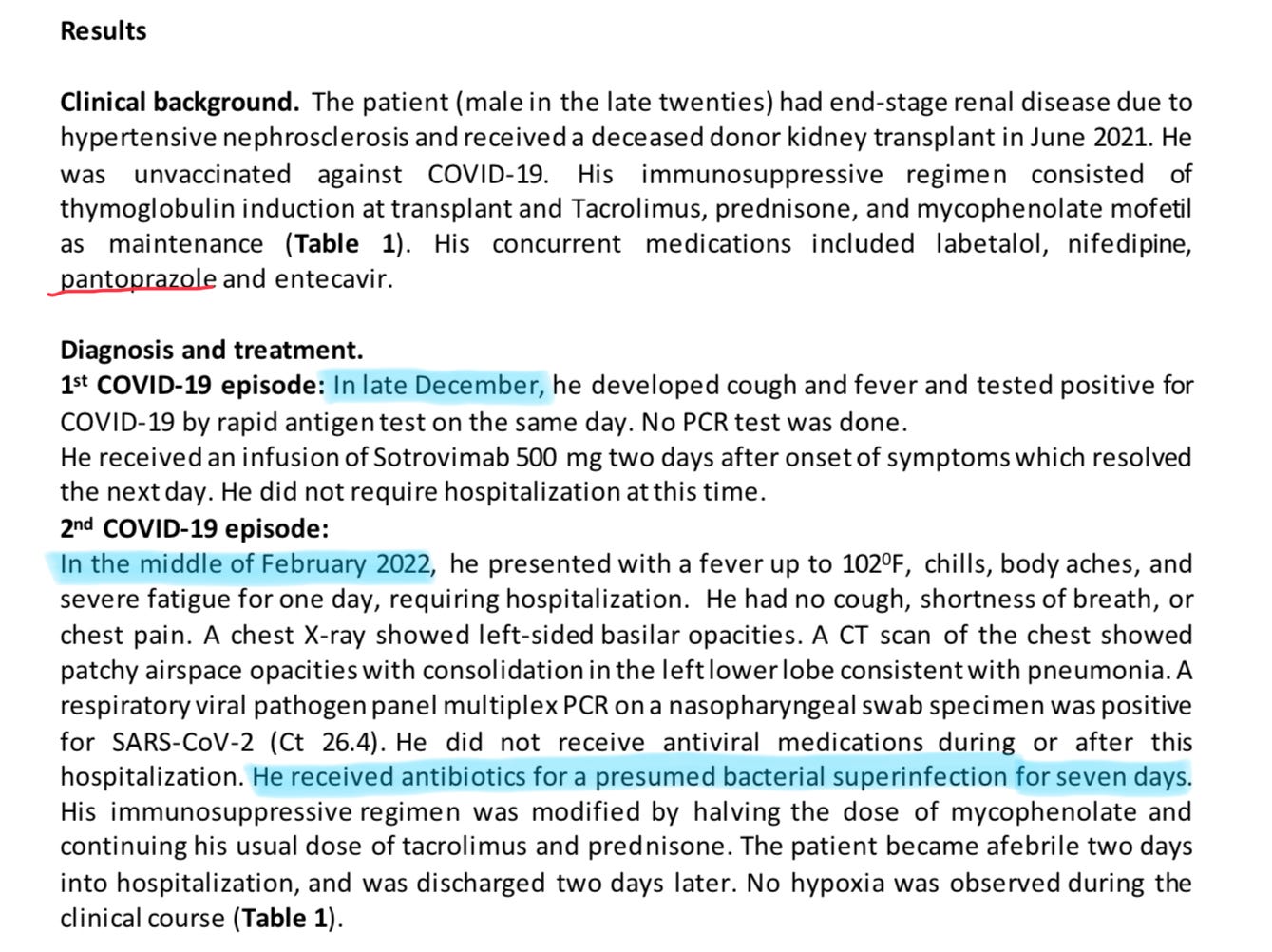
Here we have the details of said patient. Used PPIs (proton pump inhibitors, strongest anti-acids we have, over-prescribed), and was in a immunosuppressed state, which dictate the outcome of the disease.
The real question is the following. Was he infected two times in a short timeframe, or he had a latent infection ? Chances are equal to both. And for last, the common bacterial superinfection that often occurs in severe patients, immunosuppressed and, in a percentage of the vaccinated (Reverse AIDS Part II-Toll of TLR).
And now, to the real protagonist of this post.
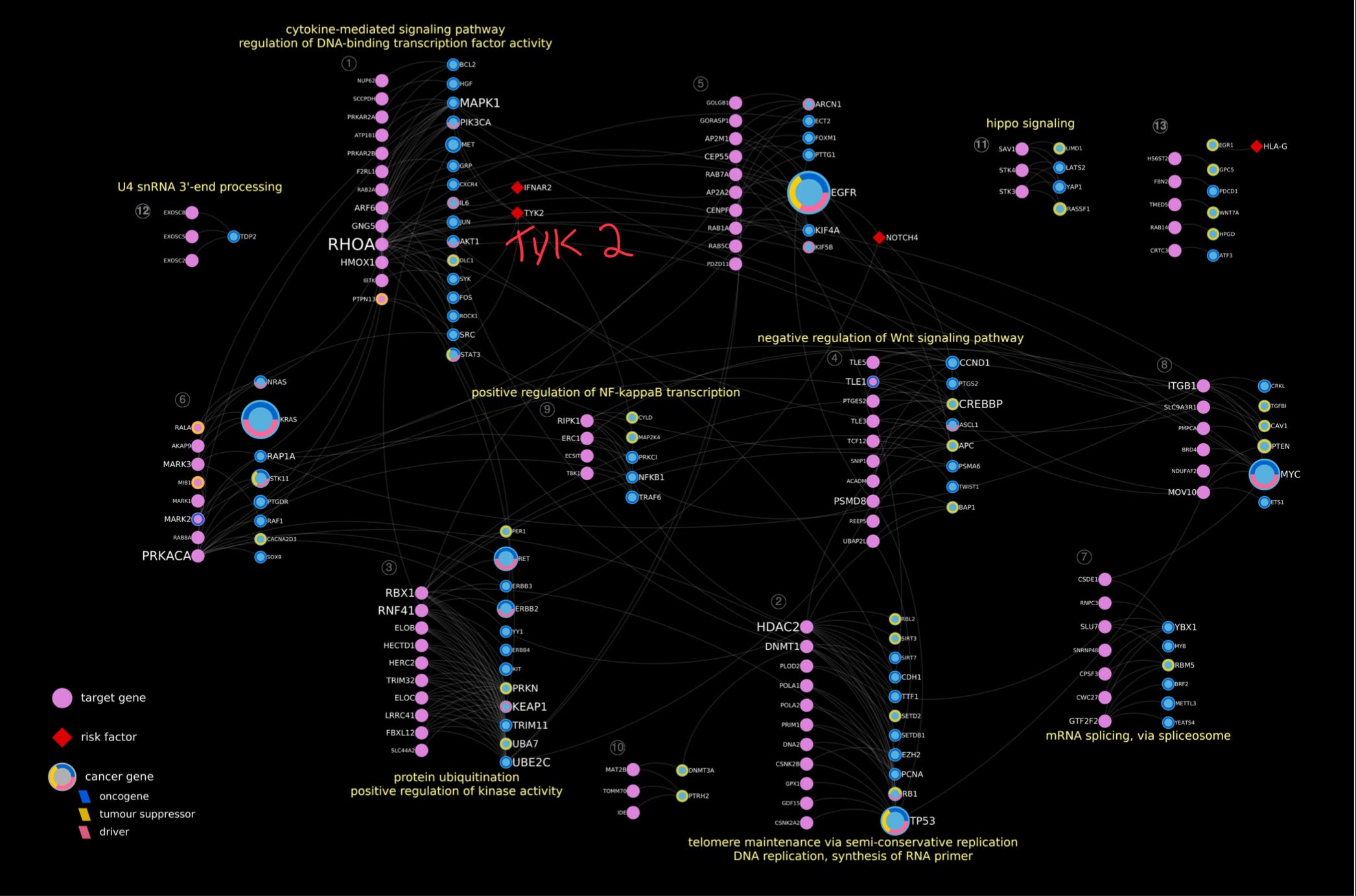
The network of SARS-CoV-2—cancer molecular interactions and pathways
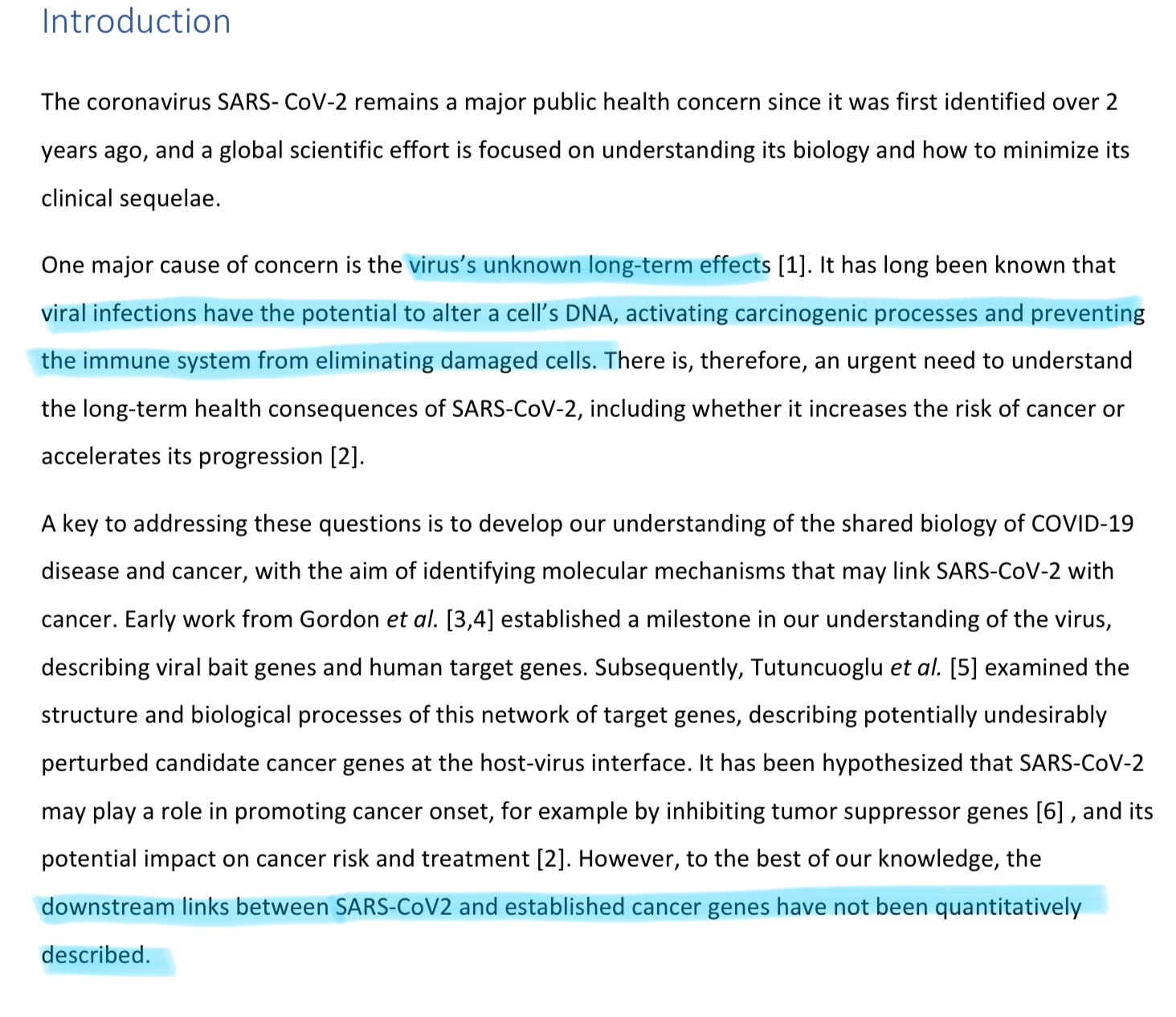
This paper is a bioinformatics one, and authors go to quantitatively find how SARS-CoV-2 might interact with cancer genes.
Why did I highlighted the first part ? Simple. As I said many times, regardless of what Omicron is, how it changed, at its base, it is still SARS. Go back a few posts, and you will find a paper talking about how Omicron, specially BA. 2 is doing subclinical damage to people, and nobody knows the long-term implications. Keep taking your damn supplements. For the hundredth time in 9 months.
BREAKTHROUGH INFECTIONS ARE NOT HARMLESS.
And they are napalm fuel in the vaccinated. You should really, really start supplementing, heavily, if you are vaccinated, otherwise concurrent infections will chip away your physiology, until you get overwhelmed.
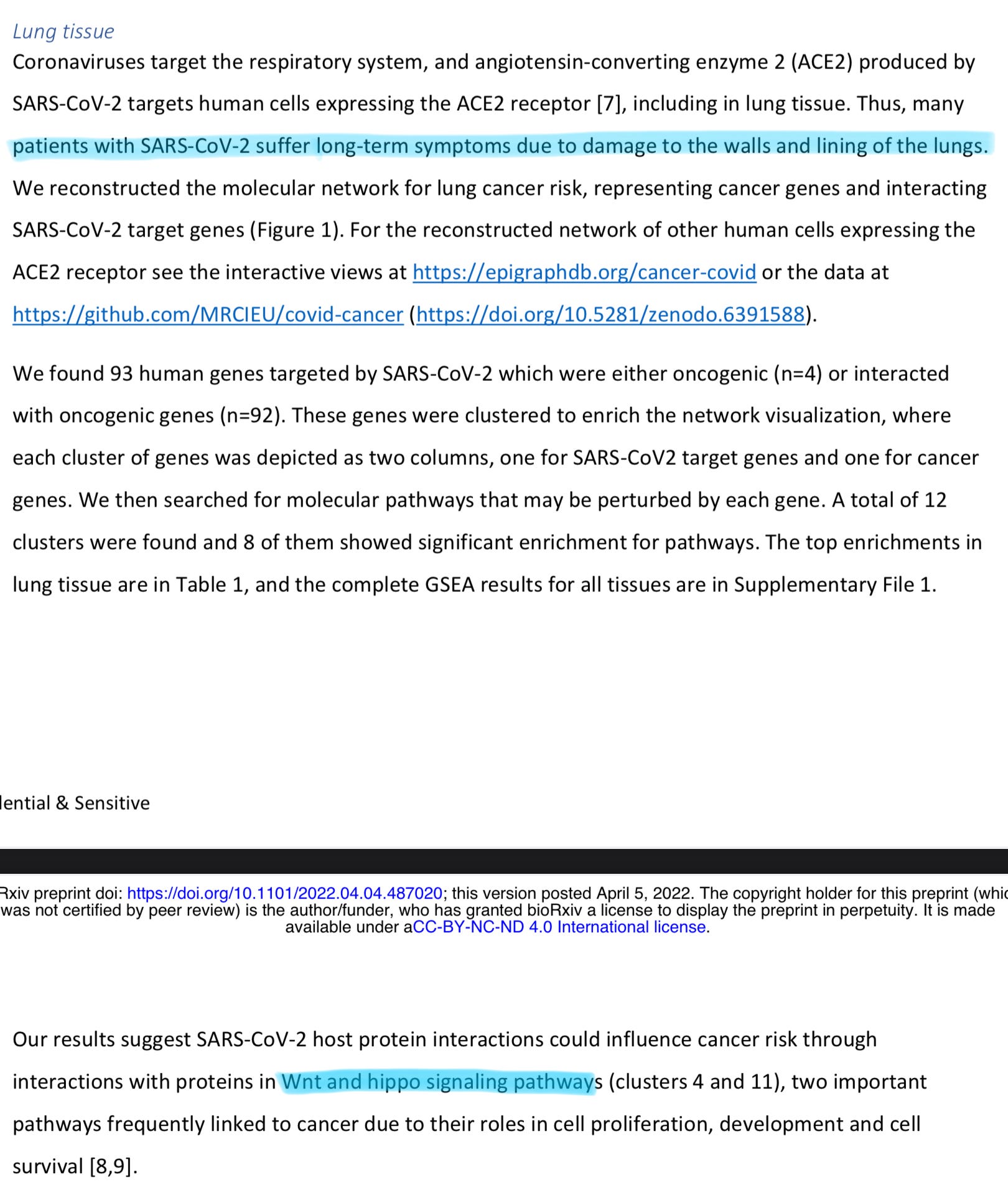
The second part I never covered, I am trying to contact the person who dug all the information, and made most of the research, but to no avail, I won’t steal his research, but that WNT pathway is very, VERY present in both viral, and vaccine, and important. I will wait a few more weeks, if I don’t get a reply from the person, I might just publish it, and ask for forgiveness later, would obviously give the credits anyway.
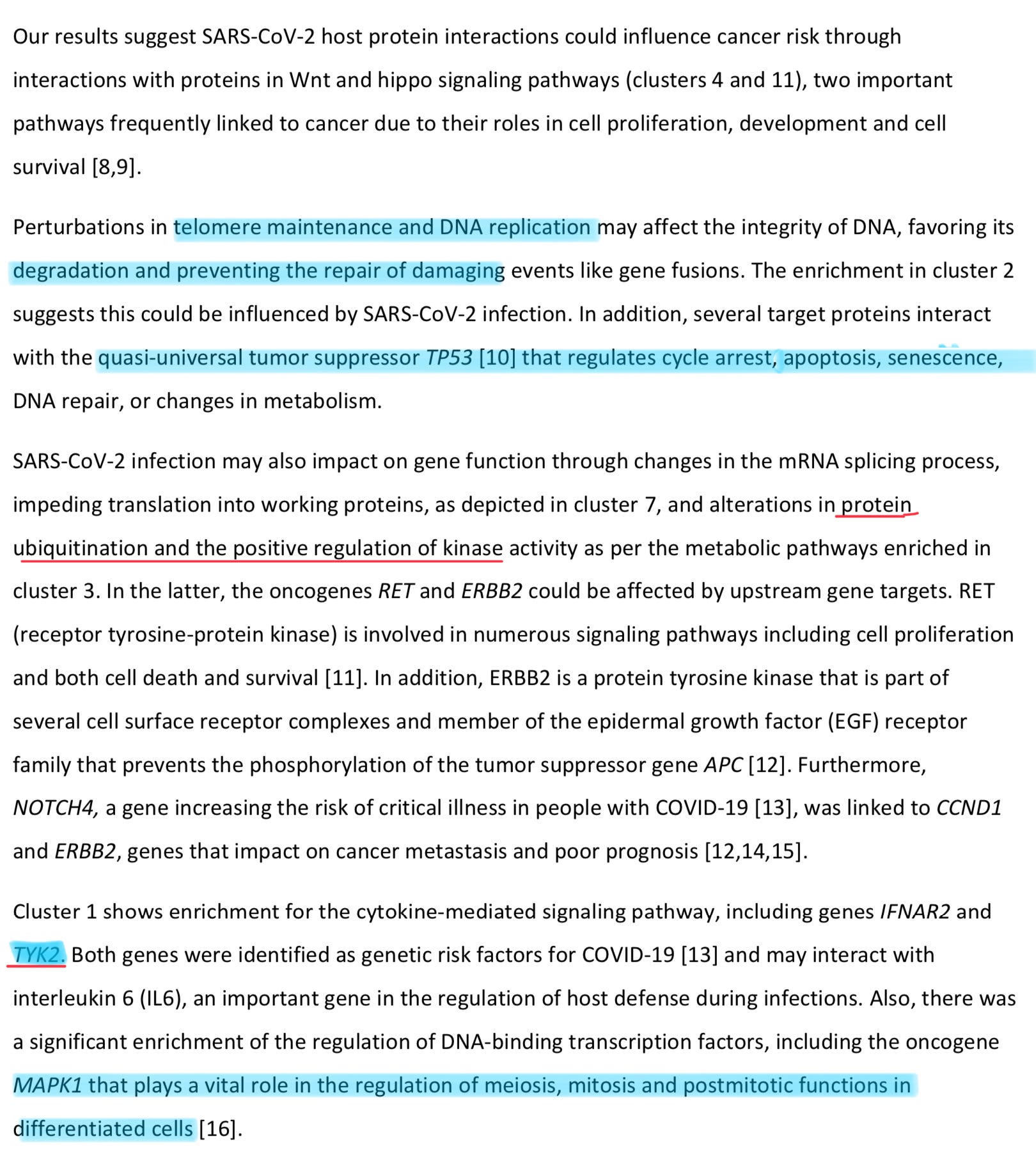
Everything here has been correlated with the infection, and anyone could guess, to the vaccination via other mechanisms, but the highlighted ones are of main concern, and don’t fear, everything I write, there is a way out, a “fix”, and I already covered before.
Protein ubiquination is really important, this is one of the ways your body deals with misfolded proteins. Don’t panic because as long as you don’t get overwhelmed, your body can, most of the time, deal with said proteins, and here lies my insistence in the use of NAC, Fisetin or Serapeptase/Nattokinase. And for last, TYK2, one we have extensive amounts of evidence about. Just read the post below.

If you didn’t catch it by now, because I like people to think for themselves, in my opinion both the viral infection, and vaccination deetirous effects are mediated but the same protein. The Spike Protein. If virus does one thing, in my opinion, and observations, the vaccines using the spike protein will do the same.
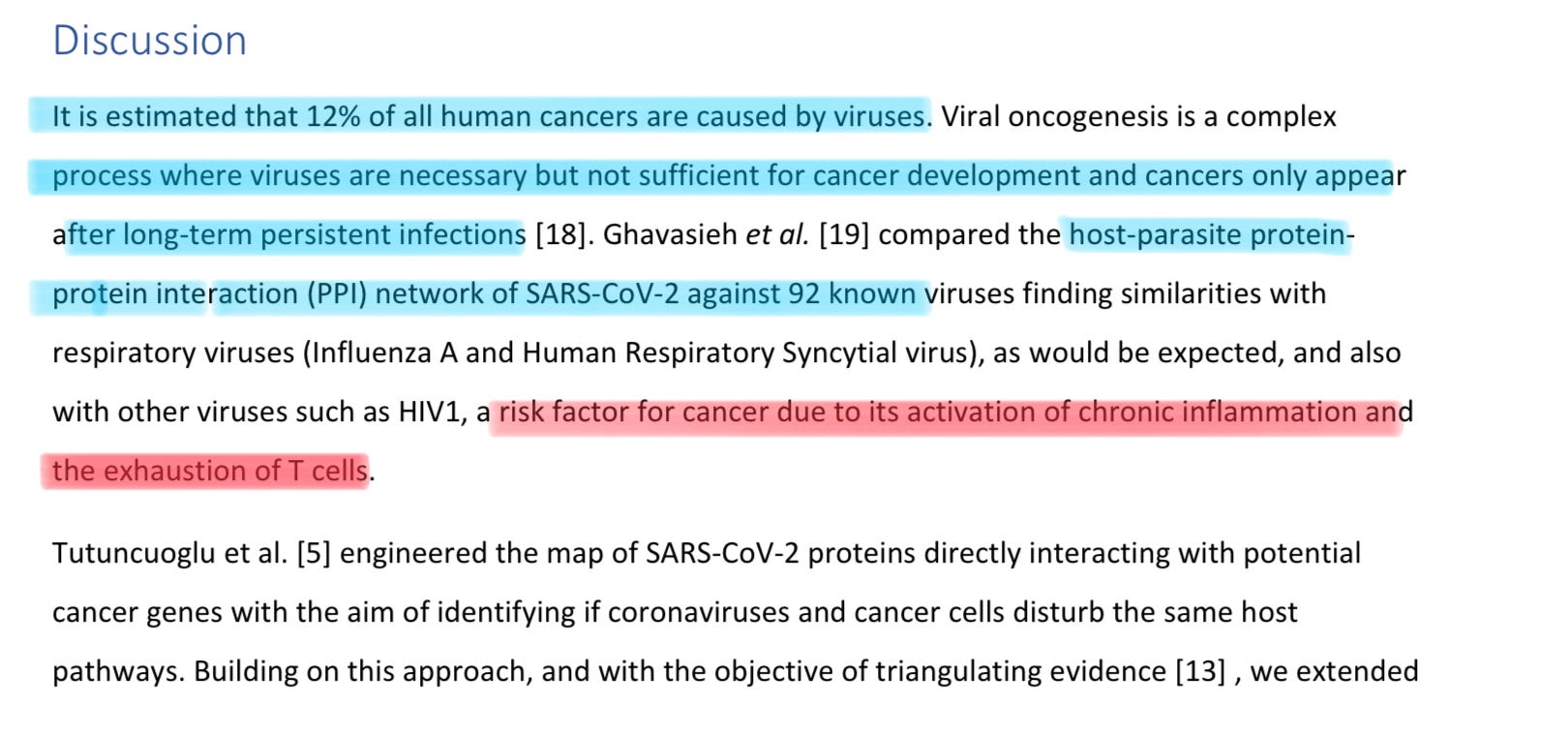
I have covered, extensively, both long-term persistent infection of SARS-CoV-2 (I was in fact, one of the first in the entire planet to propose that, with a few other brilliant doctors. I am not brilliant btw), and recently covered that SARS-CoV-2, in some people, inflicts a persistent low-grade chronic inflammatory state. And the T Cell one, well, shouldn’t take you long to find it here (Reverse AIDS, Reverse Marek. Yes, it is all a big singular hypothesis).
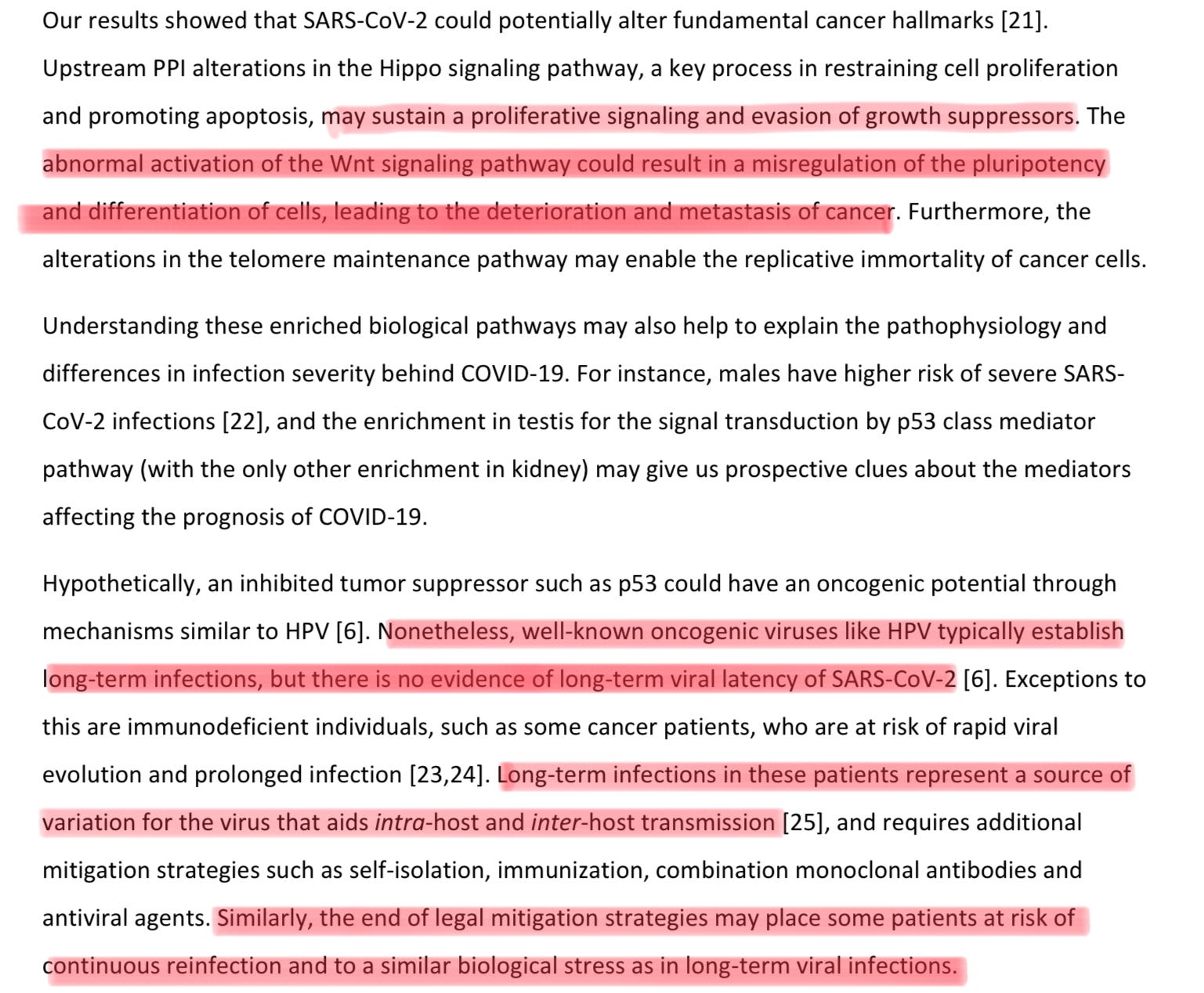
WNT signaling uses specific molecules, and proteins to do what they are describing here. Said proteins that are heavily unregulated by our pathway (Reverse AIDS), and the other person pathway, by using Beta Integrin. Do you want to guess where that leads ?
Chronic infection, and *check notes. Th 17 differentiation
If you read the posts linked in the Reverse AIDS hypothesis, and most of the recent ones, you will start to get a complete picture.
At the end of the post below you can find my perspective on how to fight most of these effects, both from a natural infection, and vaccination effects. In my opinion the posts about mitochondria are also among the most important ones.
You can use Ko-Fi to buy me a coffee whenever you feel like it.
If you enjoy independent, complex, interdisciplinary analysis, and forecasting consider becoming a free or paying subscriber, support is very much appreciated. Sharing also helps me tremendously. Deep appreciation for all the supporters.
Have you looked at NAD+ relative to infection and vaccines? I've been looking at NAD+ in terms of health/metabolism, and it has to be connected with SARs. Here's an interesting paper: https://www.nature.com/articles/s42255-021-00507-3
NAD+ is required for DNA repair and energy production, so deficiency can be causal for cancer.
I'll have to look at WNT :-)
I find your hypotheses are well based in the science, fascinating to read. 😊 (even though much of the science you speak of goes over my head, I have a BS in biology and a minor in chemistry, so I can follow it a little). We will see how much turns out to be true.