


SARS-CoV-2 burden on the kidney and children
NAD helps

For a while now, I have persistently brought up the underobserved, yet highly significant effects of SARS-CoV-2 infection in multiple organs, in which the damage now is mostly subclinical, somewhat “mininal”, a blip in standard bloodwork, but given enough time, or rather reinfections, the burden cometh.
While every organ is “essential”, an organ of high importance is your kidneys, because they control the fluid dynamics in your whole body and remove waste, both are important, but I give more importance to the first. I have a few articles mentioning the kidneys, and one specifically covering them. In the third article below, I mention this paper, where the authors find that NAD+ ameliorates kidney injury and damage.




Association between COVID-19 and the development of chronic kidney disease in patients without initial acute kidney injury


This is quite an interesting and pertinent paper, analyzing the long-term trend of developing chronic kidney disease without already pre-existing disease, or developing AKI (Acute Kidney Injury) one month after infection with either SARS-CoV-2 or Influenza. They matched both groups based on age, sex, race, pre-existing condition, and a few laboratory values to reduce biases and confounding factors.
The major finding of this paper was the significant higher risk of developing advanced Chronic Kidney Disease (CKD, stage 3 to 5) in the SARS-CoV-2 group compared to the Influenza group over a period of 12 months, Hazard Ratio [HR]: 2.02, 95% Confidence Interval [CI]: 1.69–2.42, p < 0.000, in simple terms, Covid patients were twice as likely to develop advanced kidney disease compared to influenza ones.
Even after excluding initial AKI, SARS-CoV-2 patients still had a significantly higher risk of developing kidney injury after the first month (3 times more likely), and having an eGFR < 60 mL/min/1.73 m compared to influenza patients, eGFR below 60 indicates reduced renal function, and it is one of the main markers for diagnosed CKD, the lower eGFR, the worse the kidney function is.
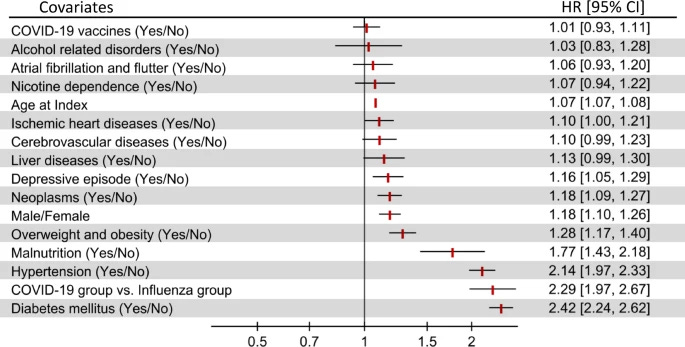
These findings were more pronounced in patients over 45 years old, regardless of sex, younger patients didn’t show a statistically significant increased risk of advanced CDK at 12 months, but they did show increased risk of AKI and reduced eGFR. Risk factors for increasing the odds of developing and worsening CKD are the well-known players, hypertension and diabetes, both of which severely impact renal function over time.
Vaccination status is not significantly associated with kidney dysfunction, something the Long-term article covers, in which the unvaccinated renal function is significantly impacted at first, and the Liver for the vaccinated.
The mechanisms for this long-term renal dysfunction and damage are many, including direct infection of kidney cells (they express both ACE2 and secondary receptors), which can initiate localized inflammation, damage, and fibrosis. Both directly via this mechanism and indirectly, this will cause endothelial dysfunction and chronic microvascular damage, disrupting blood flow and oxygen supply to the kidneys.
There is, of course, the large interplay between the Kynurenine Pathway and kidney disease, given that the kidneys are one of the main organs involved in the formation, degradation, and especially excretion of Tryptophan end-products, any disturbance in the KP results in kidney pathology, and vice-versa. The KP in and of itself can be pro-thrombotic, thus contributing to kidney disease.
Why this matter is multifold, but I shall focus on two-fold for our purposes in this article. Primarily, as the kidney controls fluid dynamics for the entire body, it should be a given dysfunction of your kidneys will impact your cognitive function at some level, especially over a long enough timeline.
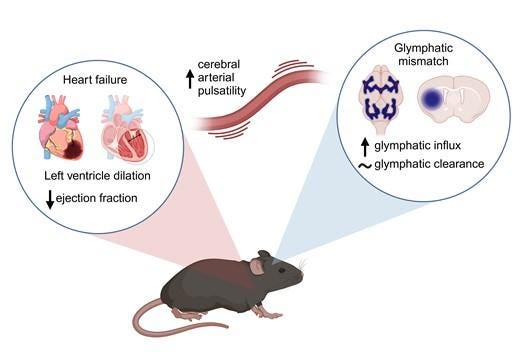
Cognitive impairment in Chronic Kidney Disease is associated with Glymphatic Dysfunction. CKD is associated with increased cognitive impairment, and interestingly, each 10 ml drop in eGFR below 60 ml is associated with an increase of 11% in cognitive impairment. Heart failure is prevalent in CKD, and the opposite is also true. Omicron variants cause a severe, significant cardiovascular burden, in which the cardiac impact may last months, and clearly it will impact the kidneys.
The most recent published research shows that glymphatic dysfunction is present in heart failure, and heart failure alone contributes to cognitive decline, because of the progressive reduction in blood flow to the brain. Here, the authors go through extensive and detailed research where they find an increase in the influx of fluids to the brain, but without an increase in clearance.
Another overlooked, by basically anyone, put a parent, is the burden of SARS-CoV-2 infections over time in younger people, especially children and adolescents.
Reinfection with SARS-CoV-2 in the Omicron Era is Associated with Increased Risk of Post-Acute Sequelae of SARS-CoV-2 Infection: A RECOVER-EHR Cohort Study
Excuse my French, but given the clusterfuck of viral evolution that is SARS-CoV-2 in this Omicron era, honestly, it could easily be called SARS-CoV-3, each wave birthed from a new variant, has enough mutations to evade previous immunity. While safeguarded from severity for the vast majority of the population, you are not shielded from everything else we cover.
Statistically, over the last few years, reinfections have led to more Long Covid symptoms and the development of the disease per the clinical definition. This is a large study, using data from 40 children's hospitals consisting of a total of 465,717 individuals under 21 years old. 77% of all patients in the study are unvaccinated, and they separate outcomes by vaccinated, unvaccinated, severe, and non-severe infection.


Younger people, especially children, respond very distinctly to the infection compared to all other age groups, and the effects of reinfection here are glaring. Children who experience a second infection are 2 times more likely to receive a Long Covid diagnosis than children with one infection. To understand the increased risk and the statistical analysis, all these are from reinfection.
Myocarditis, 3.5 times more likely.
Changes in taste and smell, 3 times
Blood clots, 2.3 times
Heart disease, 2 times
Acute Kidney Injury, 2 times
Electrolyte Imbalance, 2 times (this is a mainstay in any reinfection)
Generalized pain, 1.7 times
Arrhythmia (Heart beating at irregular pace) 1.6 times
Abnormal liver enzymes 1.6 times
Fatigue, and Malaise (general ill feeling) 1.5 times
Children and adolescents have a very distinct immune response compared to adults, and the older the age group, the more distinct the immune response between the younger vs older groups becomes. But reinfections are not harmless, and unlike adults whom we have a substantial amount of data, we don’t have a lot of data on the long-term effects of mild infections, which cells decline, increase, or the organs are more impacted.
I will now focus on a specific article on a recent paper talking about lasting epigenetic modification after the mRNA vaccine. It took researchers a while to corroborate a finding from another group that was criticized back in the day. I won’t rush it, so I will publish at some point this week.
Consider becoming a paid subscriber, and if you are one, thank you, it helps my interdisciplinary research.
AKI is very common in hospital patients. One of my main jobs was trying to prevent and mitigate AKI from drugs, surgery, sepsis, fluid shifts etc. Most people recover well, if identified and treated early. But viruses causing direct kidney injury has really never been seen before (unless the patient is septic but it is sepsis that causes it)
But I can't even read the stuff on children. My brain won't let me
Moriarty, I'm going to have to increase my SSRI intake to deal with the depression you are causing me, LOL. :-D
Your comments on what happens in the kidney when it is damaged made me think that oral intake of DMSO during and after a C19 infection (or vaxxxine) might be a significant help, as it decreases inflammation and fibrosis. Your thoughts?