
Long-term effects of Omicron BA.2 breakthrough
And our master antioxidant

Some days, fate just sends you in a direction, or life just gives you a gift, and any previous schedule or planning goes out of the window. Today is one of these days, because no matter how consistent or accurate any forecasting I may have done is, nothing beats evidence. I will need to emphasize the following section.
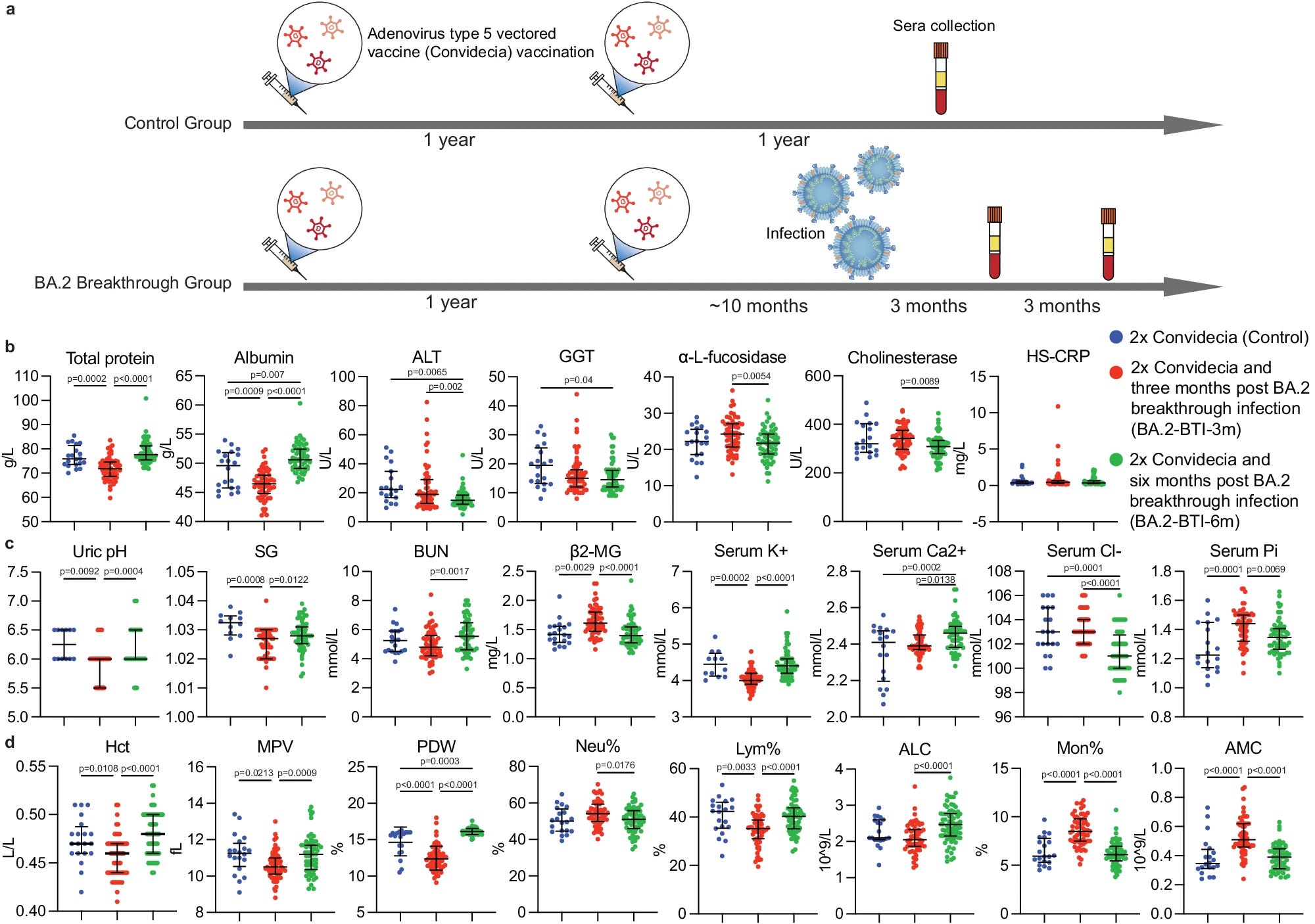
This research paper was done by Chinese scientists, in China, so there is no mRNA vaccine involved. The group in this study was vaccinated with the Adenovirus Type 5 vector vaccine. This vaccine is similar to the AstraZeneca, it still expresses the Spike Protein.
Now if you want to ascribe everything to the vaccine, it is your choice, papers like this one still give us insight into what is going under the hood, under different settings. My goal is to help people recover.
Long-term effects of Omicron BA.2 breakthrough
One of my main interests since 2022 has been the long-term consequences and effects of Omicron Breakthrough infections, not only from an immune system perspective (as in what it has done to our immune cells and the immune system itself) but also on a systemic level. This paper goes into great detail on what it does at the tissue level (the impact on organs), metabolic level, hormonal level, and coagulatory level.
Except for a small portion of researchers, minimizing or trivial interest in what these infections are doing is rampant, especially because as scientists do, there is no consensus in most mechanisms (to this very day, many who dispute the effects the viral infection has on the liver…)
Long-term effects of BA.2 BTI on major organs and blood cells
Tests to measure liver and kidney parameters were done at two time points, 3 months, and 6 months after a Breakthrough Infection (BTI from now on). In line with previous studies from China (done in unvaccinated, vaccinated, boosted, but I didn’t write about it) they observed a general shift in certain important markers. Protein synthesis was affected, liver enzymes (Cholinesterase CHE, α-L-fucosidase AFU) were elevated, Alanine Aminotransferase (ALT) and γ-Glutamyltransferase (GGT) (these are all liver markers) were also elevated at the 3 months mark, and at 6 months the trend was into normalization, meaning whatever damage or inflammation present in the liver was healed.
Kidney markers had different levels, BUN (Blood Urea Nitrogen) was low, Beta20Microglobulin was high, electrolyte levels varied, creatinine levels remained unchanged and Magnesium had extreme fluctuation levels, and many things can cause that, no cardiac injury was observed. Similar to the liver, these levels normalized at 6 months post BTI.
The next section of the study is the one I was intrigued by, a personal observation that most likely others have done was how the body compensates when there is a decrease in Lymphocytes there is an increase in Neutrophils. Similar to the previous 2 markers, there was a lower percentage of lymphocytes, at 3 months, but at absolute lymphocyte count was not significantly decreased. Monocytes and neutrophils increased, with absolute monocyte count remaining high at 3 months, and normalizing at 6 months.
The authors propose that the increase in monocytes is a byproduct of the body clearing fragments and antigens from the virus, which is great and important.
Their next step was doing a proteomic analysis, meaning studying and measuring changes in different genes and proteins at a large level. There is no easy way to explain this type of analysis, but for simplicity, the main upregulated proteins were coded by genes IGKV1D-33, UNC13D, CARHSP1, SYTL4, LIMS1, and ARHGAP45, while the downregulated ones included MT-CO2, ATP5MG, ALDH7A1, PLCXD1, and SULT2B1.
The GSEA (Gene Set Enrichment Analysis) showed that coagulation in the BTI 6m the expression of coagulation intersection genes CSRP1, ILK, ITGA2B, F11R, SELP, FCER1G, and TFPI upregulated. The GSEAs of the liver, lungs, pancreas, or heart were insignificant, indicating no considerable organ damage was found at six months.
Some of these genes play different roles if abundant or deficient in different diseases, and cancer, this is entirely a comment of my own, not alluded to by the authors at any point in the paper. All the other gene-related measurements in a similar style to this one found similar trends, any negative change was normalized at 6 months, and the immune reaction was mostly conserved at 6 months. The focus of the paper for the most part is this. One interesting trend among all types of immune cells was their “lethargy” (my term, not theirs), in which their bioenergetic potential was reduced, even after recovery, a level of reduction persisted.
And here is where things get very interesting. Change in metabolic profile and especially hormone.
In the author’s own words.
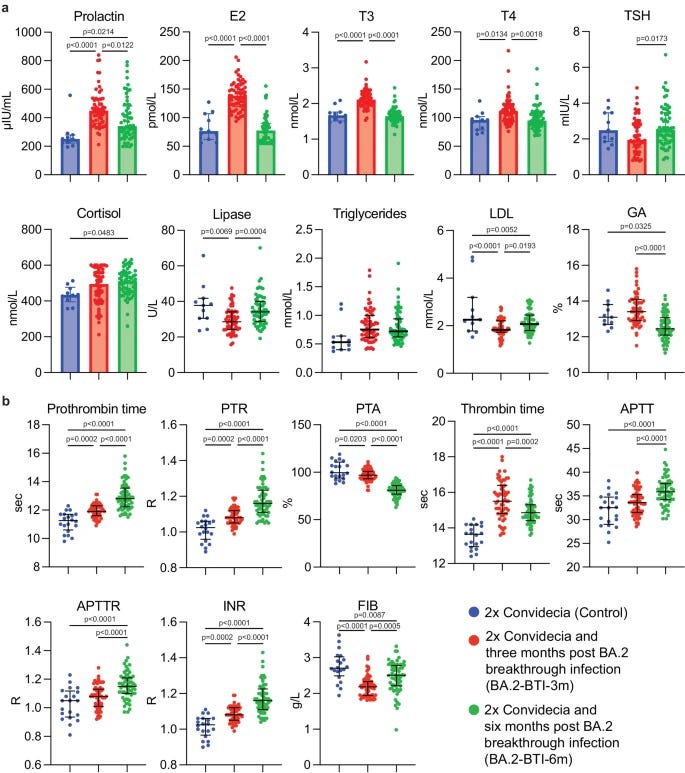
Cortisol has an immunosuppressive effect. It treats conditions caused by an overactive B cell-mediated antibody response29,30. The increase in cortisol seen at six months of infection may be a protective mechanism against the over activation of the immune response.
Importantly, liver and kidney injury and abnormal hormone levels can induce metabolic disorders, as indicated by the extreme changes in the mid-term serum glucose level (glycated albumin, GA), which did not recover to the control levels even six months after BA.2 BTI (Fig. 8a). This indicated that glucose metabolism was affected in the long run. Cortisol promotes the activation of glycogen phosphorylase, which is required for the effect of adrenaline on glycogenolysis29,30. Therefore, changes in cortisol may correlate with both the immunity and the abnormal GA. Lipid metabolism was also disturbed, with the levels of lipase and low-density lipoprotein (LDL) first decreased and then increased at three and six months post BTI, respectively (Fig. 8a) but with recovery trends.
This is a somewhat complex but overlooked trend, not only from the cortisol side, that has gained attention, but the whole hormonal side of Covid, in a recent paper titled “Occult endocrine disorders newly diagnosed in patients with post-COVID-19 symptoms” they found that endocrine and metabolic disorders are overlooked, underdiagnosed and missed especially because they were frequent but not associated with Long Covid symptoms, so it is very easy to miss.
And lastly, they measure what to me is the most important aspect of Omicron infections (perhaps only the endocrine/metabolic aspect is more important) the coagulation profile. Unlike previous variants, Omicron lacks a hypercoagulability profile, meaning it does not create the clotting observed between Wuhan and Delta, its coagulatory profile is similar to DIC. Disseminated Intravascular Coagulation.
The defining feature of DIC is… microthrombi. Commonly referred to as microclots. “PWH who fulfil the diagnostic criteria for DIC show significantly more dysregulation of the haemostatic system. This may reflect baseline abnormalities including endothelial dysfunction in the context of inflammation and liver dysfunction.”
I think I know someone who saw this coming a little bit ago, like yesterday.
To be abundantly clear, DIC is an incredibly complex condition to the point even among experts, clinicians, and critical care doctors there is little consensus on the possible mechanism, but there is evidence of certain common denominators such as the PWH paper referred to above.
To my knowledge, given my observations, one of the contributors of DIC in “healthy people” would be the sustained expression of HERVs, so it would be incredibly significant if researchers started measuring the expression of HERVs in all patients. Especially with the distinction between vaccinated, unvaccinated, infected, etc, since some researchers have “clean” samples (samples from patients before getting vaccines, after, and after infections).
One poignant quote from the author’s closing remarks.
Therefore, mild Omicron BA.2 BTIs induced potent NAbs against SARS-CoV-2 variants last longer than half a year but cause tissue impairments and require six months for the body to rebuild its defenses against other possible pathogens, as in vaccinated healthy persons.
I don’t link sharing with other people, especially researchers screenshots because it often looks, and sounds like I am arrogantly dunking on them, but you can go on social media and find both vaccinated and unvaccinated Covid researchers developing sequelae from “mild” Omicron.
Also if you (vaccinated or unvaccinated) got Omicron and experienced persistent symptoms, especially “feeling unwell” and supplementation didn’t solve anything, consider asking your doctor for a hormonal panel, in my experience this is more common in women, but it can also happen to men.
Should you be worried ? Absolutely not. But you should start taking care of your overall health seriously, all variants are evolving to evade our antibody response, they evade partially the T-cell response (the authors bring up this point in their paper, relying on T-cells), choose whatever form of supplementation you want and treat each infection accordingly, as fast as possible.
In this regard, I will be publishing a simplified version of my “stacks” (supplementation suggestions), since so many people have for so long asked. Nothing changes, very few additions, and some additions will have 0 explanation for now, this simplified version will be published in the coming days. But before ending this, since my Glymphatic System Part II hinges entirely on arguing one specific mechanism… and in case you need a refresher on the Glymphatic System.

SARS-CoV-2 Inhibits NRF2-Mediated Antioxidant Responses in Airway Epithelial Cells and in the Lung of a Murine Model of Infection
NRF2 is the master controller of our antioxidation system. Downregulation, means we experience a lot more oxidative stress from the get-go, not only does this mean cancer acceleration in some cases, but it is also very significant when it comes to neurodegeneration induced by multiple causes. Further reading if you are interested in why this is important and why I am so adamant about supplementing with NAC.

I truly appreciate your support !

https://www.fightaging.org/archives/2024/03/mitochondrial-dysfunction-in-the-aging-of-the-brain/
Saw the 5 mins after reading this, and thought you might be interested in another master antioxidant.
Do you support use of Nattokinase, during and after infection?
Also, thank you so much for sharing your work. I always enjoy when you show up in my email.