


Fibrin, Spike Protein and the mystery between
The gift that keeps on giving

Sometimes the subject matter demands a distinct approach, and today’s subject demands it, so I will somewhat oversimplify (from my perspective) this recent paper, which is incredibly important, and then do what we usually do. Connect the dots others don’t.
FYI this took a little longer than expected because, as you will see things got significantly more complicated as I went through the paper.
Fibrin drives thromboinflammation and neuropathology in COVID-19
One of Covid’s longest-standing mysteries has been its “coagulability variation capacity”, a fancy way to say how a respiratory virus is able to induce systemic clotting, in both severe, non-severe, and damaged (Long Covid/Vaccine injury) cases with significant variation. To me also how the Spike Protein + mRNA + LNP was able to induce systemic self-assembly of clots. From big clots to small… micro clots.
Clotting, whatever size it is, can induce significant debilitation, it induces system damage at different levels, from a clinical (you can easily measure) to a subclinical (you can easily miss, hard to measure), and it will also compromise the Blood Brain Barrier. A large subset of Long Covid and “Long Vaccine” patients have persistent clotting issues, sometimes for over 12 months. I, Geoff and many others had our own perspective on how that happens.
Fibrinogen binds to SARS-CoV-2 spike
Fibrinogen is a “big protein” that circulates in the body, and whenever the body suffers a form of injury, it will initiate a complex process which at a point forms thrombin, and when thrombin meets fibrinogen + platelets, you get a complex “cellular mesh” to plug wounds— also known as a clot.
To start to understand how this happens, the first step is testing in assays (sometimes literally in test tubes), and by mixing Spike Protein with fibrinogen and fibrin, they found it actually binds (glues) to both, but with much weaker strength than to ACE2. Once again the now infamous “receptor hierarchy” I have mentioned recently. Next step was analyzing what happens when you inject mice with fibrinogen and spike protein, and they found that both could interact in the lungs of mice.
To understand how to better treat and “target” these conditions, we need to understand how it occurs at a molecular level. This next section will be of the highest importance later on. These are the positions where the Spike and fibrinogen bind.
Reverse mapping of fibrinogen binding on SARS-CoV-2 spike variants revealed binding sites spike37–103, spike229–251 within the N terminal domain (NTD) S1 subunit, spike305–319, spike341–355 within the receptor-binding domain (RBD) and spike1049–1063 within the S2 subunit (Extended Data Fig. 1f and Supplementary Table 2). Computational docking identified a model with the best docking energies with close association between fibrinogen γ364–395 and spike37–103
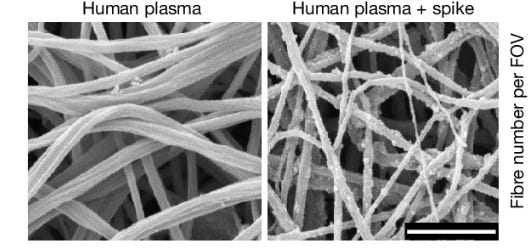
When different proteins interact together, you must see if there is any form of additional function or dysfunction. By adding Spike Protein to donor plasma with thrombin (the trigger for clot formation) in it, the authors observed both clots forming and these clots had abnormal structures. They were denser and had thinner fibers, making them more resistant to being broken down, thus observing that this interaction delays fibrinolysis (the breaking down of clots). By adding Spike + Fibrin to Bone-Marrow-Derived-Macrophages they uncovered that this combination enhances the fibrin inflammatory properties. It is not that Spike Protein-derived abnormal clots are resistant to being broken down by the body, but they are also more inflammatory.
Fibrin drives inflammation
After fibrinogen is converted to fibrin, it exposes the cryptic (effects unknown) inflammatory piece γ377–395. By using mice without this specific section (epitope) the authors found that it greatly reduced inflammation, oxidative stress, and lung damage compared to normal mice. To further test this hypothesis they used mice that lacked fibrinogen and this showed a remarkable decrease in inflammatory pathways, including Type I Interferon responses, which when aberrant are responsible for severe Covid, and these are usually persistently high in Long Covid too.
They also observed that fibrinogen-deficient mice exhibited an increased activation of Natural Killer cells (NK), which are crucial to fight viral infections and cancer.
Fibrin suppresses NK cells
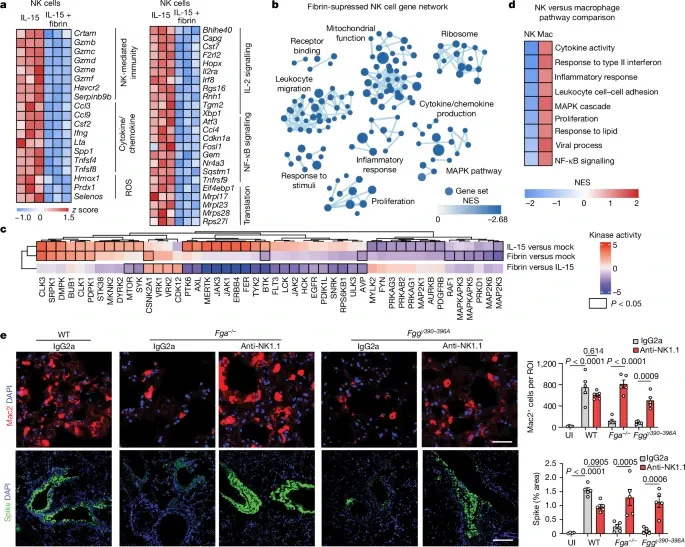
To understand how Fibrin by itself suppresses NK cells the researchers stimulated NK cells from mice to fibrin and analyzed its gene expression, finding that 277 genes were downregulated (meaning a lot less critical proteins were produced) and 76 upregulated. The suppressed genes included those involved in NK cell immunity, cytokine production, and responses to oxidative stress. These changes led to a broad suppression of pathways essential for NK cell function, including mitochondrial activity, cell migration, and the inflammatory response. All these changes especially in critical pathways lead to a reduction of NK proliferation, lower production of IFN-Gamma and Granzyme, and lower activation of these cells, dampening the ability of Natural Killer cells to combat infection and clear pathogens.
They replicated these findings in mice afterward, proposing that fibrinogen plays a crucial role in promoting lung damage during acute Covid infection by depressing NK cells. The next section is where this paper gets a little…controversial. The authors built “custom particles” of Spike Protein (called Spike PVs) that cannot engage ACE2 receptors, to test the infection-independent roles of fibrin.
When Spike PVs were injected in mice, they triggered significant fibrin deposition in their lungs, leading to increased inflammation and oxidative stress. Mice injected with PVs without Spike Protein didn’t have this effect. Mice lacking fibrinogen experienced a severely attenuated response. In simple terms, the Spike Protein potentiates the Fibrin-independent effects described above. The controversial part is that the author injects mice with Spike Protein, which interacts with fibrinogen and fibrin, they demonstrate its effects and… say the vaccines don’t do the same, which I won’t fault them for. Either you add this type of rhetoric on papers, or you don’t get peer-reviewed.
In summary:
Fibrin plays a crucial role in promoting inflammation, oxidative stress, and fibrosis during SARS-CoV-2 infection.
Fibrin's interaction with the CD11b–CD18 receptor exacerbates lung damage and immune dysregulation
Fibrin suppresses NK cell activity, impairing viral clearance
The presence of SARS-CoV-2 spike protein enhances fibrin's pro-inflammatory effects, even in the absence of active infection
The Fibrin suppression of NK cells, and the Spike-Binding aspect of it are another mechanism that explains accelerated cancer growth observed in certain subsets of vaccinated individuals. Yet to be tested in a lab (I doubt it ever will, too much of a taboo topic).
The Things Hidden In Complexity
I simplified the paper because while I read it a few times, I foresaw it would get very complicated, very fast. Remember the places where fibrinogen binds to the Spike Protein ?

They “neighbor” or even overlap the same positions Endotoxin binds to the Spike Protein, and they are also very close to the positions for many of the Spike Protein “novel” features, some I wrote about recently. Fibrin itself is known to act as a “trap” for Endotoxin. One of its most prominent parts would be the aforementioned here and elsewhere “NTD” which is an almost perfect mimic of human Galectin-3.
Microclotting (the correct term is Disseminated Intravascular Coagulation) is seen in Sepsis and septic states, but also it has been observed in Long Covid in which Fibrin interacts with Amyloid to form microclots that can last months and impair recovery. When the abnormal clots were sequenced by another team of researchers they found something unusual hidden inside them.

The abundant presence of HERVs in severe/ICU cases of Covid is often correlated with the higher consumption of fibrinolysis factors, meaning it drains the body of the capacity to dissolve clots.
Here is the insane, multilayered twist. You need Natural Killer cells to control acute retroviral infection, the disruption brought by Spike + Endotoxin + Fibrin mixture is one that cascade throughout months, leading to fewer and much weaker NK cells thus leading to failure to control retroviruses. Adding insult to injury, Extracellular RNA is found to act as a factor for coagulation and found associated with fibrin-rich structures. SARS-CoV-2 is once again found to create lasting RNA complexes with significant inflammatory potential, also found to be hard to dissolve.
Other mechanisms and cascading effects exist, such as the most recent one related to Galectin-9. But all of these “oddities”, novel effects, and long-lasting damage potential come from one single protein. A protein that binds them all.

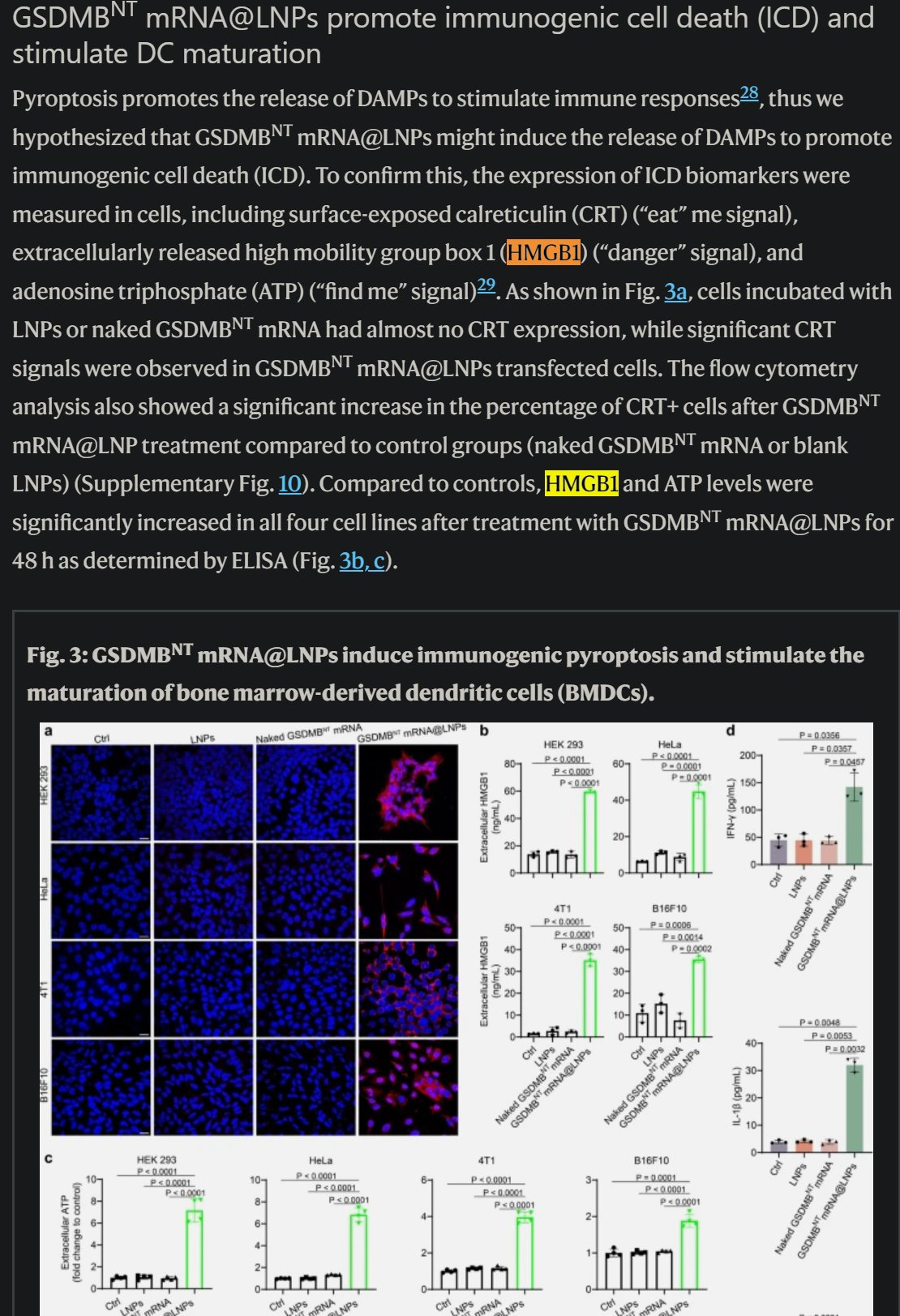
And in case you forgot or didn’t read the article above. “High-mobility group box 1 protein promotes development of microvascular thrombosis”. Let us check with the Spike Protein, Endotoxin-binding, Fibrin-friendly protein HMGB1 is present when mRNA LNP is administered. Well… that is kinda inconvenient huh.
A road yet to be traveled by me, the one about Mast Cells, but I need to mention this. Perhaps the abundance of “allergic” and “suspicious” rashes in the last 18 months is the fact that Mast Cells are being recruited to degrade fibrin. After all, Mast Cells are an abundant source of chymase, and proteolytic proteins (they break down other proteins, imagine your body's own source of Serrapatase/Nattokinase in an extremely simplified form).
The paper and all the articles mentioned here are important from a long-term perspective.
I appreciate any and all support, thank you ! You can buy me a coffee if you want (it will actually go to peptides =P).

It's a shame that the scientists always stay within the realm of viral spike protein alone because it's effect of the body may be completely different to the vaxx expressed poison.
I can't remember which interview but iirc Dr Burckhardt broke down that the viral spike protein had a broad array of (i thought 30 proteins) which would have been a far safer manufactured protein to administer (ignoring that the assumption that the platform is inherently unsafe and the DNA plasmids/Endotoxin contamination is there)
Personally I see this as an attack but it would be nice to have some information that shows the damage of the vaxx spike is worse and why/how. Ideally that a layperson like myself can understand. Perhaps the missing proteins? dampen the damage(or worsen).
Always hard because you cannot support every substack worthy of it. If I'm every in excess cash I'll be sending some your way but until then I'll share your work everywhere like the others.
Thanks
When excess deaths started being reported in UK we had a high number of deaths from 'falling over'. I have several relatives and friends who have collapsed to the ground suddenly ( did not faint or trip, just fall to the ground) resulting in various injuries.
Two deaths that I know of in last few weeks and the comments made were not that they had been ill with x/y/z but they had fallen over a couple of times.
I have not seen anyone report on it, yet it could be an indication that medical attention is essential.
Could microclotting cause sudden collapse or is it more likely to be an electrical signal issue?
Doctors are, as expected, baffled.