

Before I properly introduce and write a substack that I hold in high regard as one of the most important (non-linear) dynamics in this pandemic, and heavily overlooked, first we need to understand the first “hit” in this complex Hit and Run effect of SARS-CoV-2, the mRNA Spike and endotoxins.


Endotoxins and sepsis, sepsis-like states play a disproportional role in many of the subjects covered this year and last year in my Substack. Given the intricacy and complexity of Covid infections, especially in severe cases, the authors of this paper sought to offer a new framework to analyze and differentiate viral and bacterial sepsis.
Given how unique each patient is, especially in a septic state, whether bacterial or viral, targetted treatments remain somewhat lacking given the current interpretation of this state by modern medicine, most of the care remains in supportive care and biochemical parameters (inflammatory and other types of markers). Prolonged inflammatory dysregulation and disturbances in organ hemostasis have been observed, leading to long-term sequelae. While bacterial sepsis-related complications are referred to as post-sepsis syndrome, SARS-CoV-2-infected patients experience post-discharge complications known as "long COVID."
By using single-cell RNA sequencing the authors sought to elucidate often overlooked dynamics by other researchers, especially differences being critically ill to non-severe patients, and the differences between bacterial and viral sepsis. These findings can help the development of immunomodulatory therapies tailored to the scale of severity and disease progression, and deepen our understanding of sepsis.
Differential Expression Profiles in Bacterial and Viral-Induced Sepsis
In the process of identifying if there were and the potential differences between viral and bacterial-induced sepsis, they chose 10 genes and analyzed it in both Covid and non-Covid patients with both severe and mild forms of the disease. In the severe form of the disease, they found significant upregulation of the genes FOSB, DEFA3, CEACAM8, CD24, and S100A12 in patients with septic shock not caused by Covid. A similar trend followed in mild forms of the disease, so regardless if the sepsis and its complications were viral or bacterial, the gene expression is similar was higher.
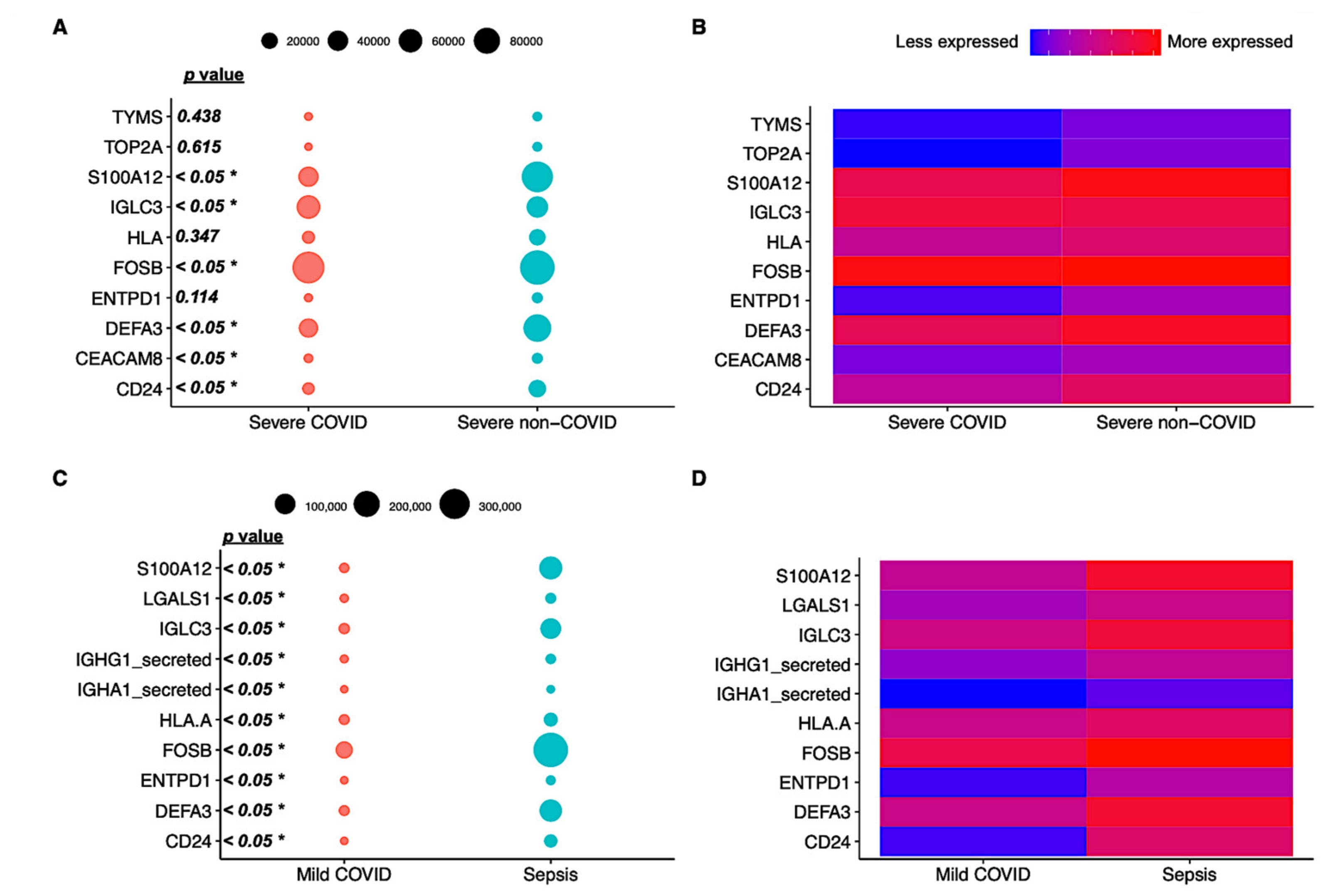
In their next step, the researchers measured the differences between mild and severe cases, and in non-covid cases. Bacterial and Covid-induced sepsis have very little overlap in their gene expression, but as expected given the amount of research and evidence produced on how severe Covid infection affects your immune system, they found higher immune cell counts in non-covid patients, especially B cells, classical monocytes, CD4, CD8 naive T cells and NK cells, now a known and well-studied trend in regards to severe Covid (the lack of proper immune response).
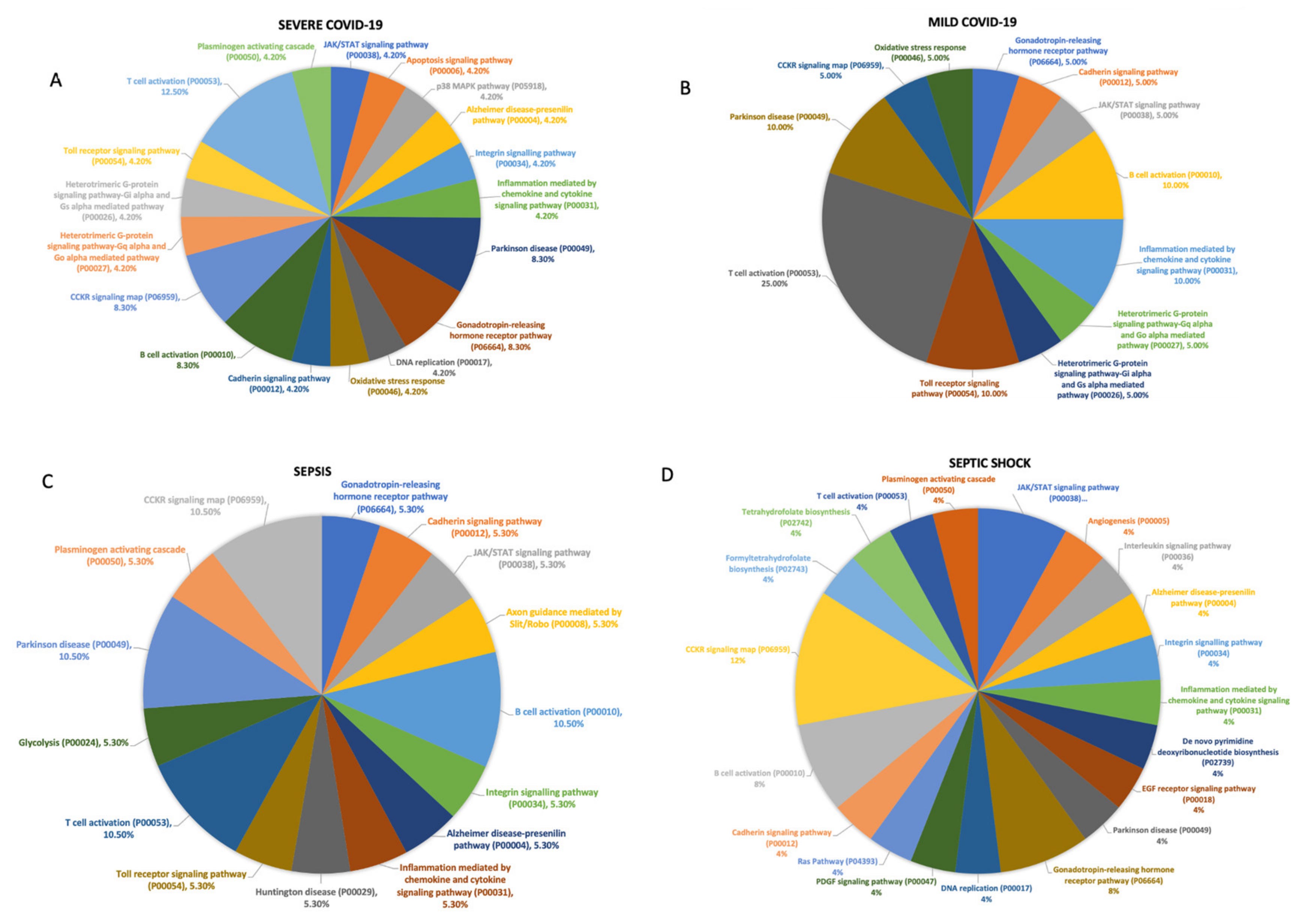
There were similarities between severe cases of Covid and sepsis/septic shock with 400 genes overlapping between the two conditions, therefore implicating there is similar pathway activation between both. To be able to differentiate between mild and severe cases of viral and bacterial sepsis, the researchers performed a functional analysis of the genes involved in each stage of the diseases.
As described above, non-severe Covid patients had more abundant T Cell activation and CCKR signaling (gut-brain axis in a simplified way), while patients with the severe form of the disease had genes that contributed to less activation of the T cell pathway. The Parkinson's disease pathway was found to be abundant in the non-severe form of sepsis. Interestingly, the inflammatory pathway mediated by cytokines and chemokines signaling was distinctly upregulated in the mild Covid group.
What do all of these complicated graphs mean in simple terms ? Critically ill cases of Covid and sepsis (septic shock) share similarities on all levels, including the “middle of the road” between going from a mild to a severe disease state. A big portion of severe/ICU Covid patients meet the criteria for sepsis, in fact, many do in fact develop sepsis, I have covered and written quite a large amount of dynamics of secondary infections, and the role their play in long-term dysfunction and damage in many of the severe cases. The authors raise the point that the widespread abundant use of dexamethasone poses a threat to the rise of secondary infection, alongside the rise of antimicrobial resistance, and much attention should be paid to this regard. Secondary infections have both the trend and the capacity to set off septic states.
As for the closing remarks of the paper, I leave to the authors.

Both Covid and Sepsis upon reaching severe status share many commonalities, but here the authors raise the fact that both present a failure of CD8 T Cell activation, a hallmark of chronic infection, and Long Covid. The depletion of CD8 T cell function can also happen via another pathway, but before discussing that, we must understand what the second highlight entails.

The authors found the increased expression of S100A12 in sepsis and in severe Covid, and in the substack above, I mentioned a recent Long Covid paper where they found a dysfunctional axis in their patients, and among the 3 proteins that could be used for new markers for Long Covid, one of them was… you guessed it, S100A12. S100A12 is present in inflammatory responses, but it is also a protein regulated by the very same axis found dysfunctional in Long Covid and in the paper we just went through. Endotoxins are known to induce the production of Interferon Gamma, and as written in the substacks referred to at the very top of this piece, Endotoxins play a significant role in SARS-CoV-2.
Interferon Gamma is also one of the major axis that can regulate IDO the protein responsible for diverting Tryptophan towards the overproduction of Kynurenines, and guess what that does to CD8 cells ? It inhibits both its expansion (creating new cells) and its memory, and if you don’t recall, failure of CD8 T cell memory is a hallmark of Covid severity, Long Covid (and sepsis). The paper I just referred to also raises the point this can be the case for vaccination… Excessive tryptophan catabolism along the kynurenine pathway precedes ongoing sepsis in critically ill patients.
A map for the visual learners that I made, of everything discussed so far.

It is now public knowledge that most Covid deaths were caused by secondary infections, often of bacterial origin, we now know that endotoxins play a major role in the inflammatory responses of the Spike Protein, and now and shortly below that sepsis either bacterial or viral also plays a disproportional role in the damage.
At this point, I do rather call Covid a novel form of endotoxic induce inflammatory and immunological dysfunction than anything else. A masterpiece designed with intricate interactions with all other pathogens laying inside us, using them as both decoys and payload on and in themselves. “Didn’t you write recently that a significant portion of Long Covid is caused by latent viruses being reactivated ?” Yes, I did, guess. Reactivation of Multiple Viruses in Patients with Sepsis

For brevity and simplicity's sake, I will share the highlights of these important papers that all share a role in everything discussed so far.
SARS CoV-2-Induced Viral Sepsis: The Role of Gut Barrier Dysfunction
The loss of gut barrier integrity and consequential dysbiosis are well known to play a role in immune function and disease progression of almost every disease, from neurological pathologies to SARS-CoV-2.
The intestinal barrier is characterized as the “motor” of sepsis, exerting a central pathophysiological role in the development of multiple organ dysfunction [11]. Numerous experimental and clinical studies have demonstrated that all the three levels of gut barrier defense are compromised in sepsis [11,12,13]. Specifically, the intestinal microflora equilibrium is disrupted, there is increased apoptosis of intestinal epithelial cells and reduced expression of TJs, Paneth cells and submucosal Treg cells are decreased while intraepithelial CD3(+) T-lymphocytes and proinflammatory cytokines are increased. These gut barrier alterations promote bacterial and endotoxin translocation in the systemic circulation activating the release of proinflammatory mediators, which may cause deleterious effects on the structure and function of remote organs, resulting in multiple organ dysfunction [13].


While the authors argue from one single point, the loss of gut barrier and the “leakage” of fungal and bacterial pathogens and proteins outside the gut, which by all the evidence and autopsies is real, one perspective doesn’t invalidate the other. The authors bring some of the most pertinent immunological changes in regards to this proposed mechanism, and a well established effect of what you can see in the first image is the shift in T cells towards Th17, losing the capacity of T regulatory Cells to keep them in check.
Pre-existing gut barrier dysfunction and endotoxemia in patients with comorbidities such as cardiovascular disease, obesity, diabetes, immunosuppression predisposes to aggravated endotoxemia and endotoxin-induced immune activation after SARS-CoV-2 infection contributing to higher rates of severe COVID-19 in these patients [73]. A potential mechanism may be that SARS-CoV-2 infection induces ACE2 deficiency leading to induced endotoxemia and deteriorated endotoxin tolerance [73]. A schematic overview of the interconnection between gut barrier dysfunction, bacterial and endotoxin translocation, immune activation and systemic complications of severe COVID-19
Patients with severe COVID-19 suffer from a “viral sepsis” syndrome and are prone to multiorgan dysfunction. According to recent pathophysiological theories, supported by preclinical and clinical evidence, the intestinal barrier exerts a central role in the sequence of events that lead from SARS-CoV-2 infection to the development of viral sepsis with severe systemic complications. SARS-CoV-2 disrupts the integrity of the biological, mechanical and immunological gut barrier with mechanisms described in the present review. This dysfunctional gut barrier permits the escape of luminal bacteria, fungi and endotoxin to normally sterile extraintestinal sites and the systemic circulation. Pre-existing gut barrier dysfunction and endotoxemia in patients with comorbidities including cardiovascular disease, obesity, diabetes and immunosuppression predisposes to aggravated endotoxemia. Bacterial and endotoxin translocation promote the systemic inflammation and immune activation, which characterize the SARS-CoV-2 induced “viral sepsis” syndrome associated with multisystemic complications of severe COVID-19. When treating patients with COVID-19-associated sepsis, we should not neglect protecting their intestinal barrier by applying general measures including adequate fluid replacement to prevent visceral-microcirculatory disturbances or enteral nutrition to provide important nutrients for enterocytes. Further clinical studies are needed to explore the potential positive impact of more specific gut barrier modulating treatments
The paper above also cites a few potential natural interventions to address these changes, Arginine, Omega 3, γ-linoleic acid, and Glutamine. Of greater interest to me is Glutamine, because it literally acts both on immune cells and on gut barrier integrity, it is a powerful supplement for anyone who suffers from gut issues, especially inflammation and erosion (such as gastritis). Resveratrol, curcumin, and quercetin are all potent anti-inflammatories and antioxidants that also help with gut barrier function.
The following paper is also really important Patients with SARS-CoV-2-Induced Viral Sepsis Simultaneously Show Immune Activation, Impaired Immune Function and a Procoagulatory Disease State.
While extremely complex, with overlapping, sometimes contradicting pathways, the interplay of other pathogens both bacterial and fungal, and after reading how much endotoxins and these other pathogens contribute to severity and mortality, and since a significant portion of all of these processes is mediated by the Spike Protein, some of you may have wondered “If it is this bad, why everyone who got the vaccine or early rough infections are not dead, but sometimes may develop dysfunctional immune systems, why so many secondary infections ?”
Endotoxin tolerance and low activation of TLR-4/NF-κB axis in monocytes of COVID-19 patients
Our data provide evidence indicating that SARS-CoV-2 infection induces lower cytokine production and TLR-4/NF-κB activation in monocytes from severe COVID-19 after LPS stimulation. In addition, COVID-19 patients had systemic alterations in the peripheral blood, such as increased LPS and cytokine levels, higher frequency of immunosuppressive CD14 + HLA-DRlow, and higher expression of TLR-4 and NF-κB activation. Taken together, these results may indicate that the pro-inflammatory condition and microbial translocation markers observed in acute SARS-CoV-2 infection may induce endotoxin tolerance associated with the potential development of secondary infections.
Key messages
Severe COVID-19 patients had higher levels of LPS and systemic IL-6 and TNF-α.
Severe COVID-19 patients presented higher CD14+HLA-DRlow monocytes.
Increased TLR-4/NF-κB axis was identified in monocytes of severe COVID-19.
Blunted production of cytokines after whole blood LPS stimulation in severe COVID-19.
Lower TLR-4/NF-κB activation in monocytes after LPS stimulation in severe COVID-19.
All these states, interconnected in response to one another are effectively creating some of the most aggressive and dysfunctional metabolic loops known to modern biology, effectively subverting Tryptophan towards high toxicity, draining NAD+ (cell energy) by different pathways but mostly by the aforementioned Tryptophan one, and these open up the opportunity for secondary infection and “secondary” aggression, reactivation of latent viruses, in simple terms, it opens the flood gates for everything your T cells keep at bay.
And lost in the middle of this metabolic chaos, lies the immunological dysfunction where an inflammatory axis such as Interferon Gamma will lead to immune suppression and a race into suppressive loops that paradoxically leads to more inflammation.
And this is my cue to finally finish writing my endotoxic tolerance Substack. I will write other posts between that moment and now, but be “warned” the one about Endotoxic Tolerance will take some time, I have over 150 scientific papers to contextualize, read, connect the dots, and do what I often do. I spent months dissecting the pathways, and there is always another one, but in my opinion, it is THE most important dynamic long-term to be covered.

If you chose to support this substack or used Kofi as a one-time thing, or shared this Substack, thank you, appreciate the support.
Long time reader. Phenomenal research and summary, appreciate your dedicated work. What a mess to untangle. This is the sort of research that can lead to incredibly important and novel treatment, which thus far the "mainstream" seems less and less concerned about. But this show ain't over.
Can’t think of reading anything more important. Seminal research and conclusions in line with Covid-19 symptoms.
HIV disables the immune system by infecting lymphocytes and SARS-2 disables the immune system by infecting leukocytes. This is a strange symmetry, or maybe not?