
SARS-CoV-2 Spike Protein as a tumor fighting tool
And how Aspirin fights metastasis and salt too

In mid-December of 2024, I covered a rather interesting topic, SARS-CoV-2's role in tumor immunity. To be precise, the opposite of what you read all around, not cancer acceleration but anti-cancer effects. Not a popular topic, but I chase where my curiosity leads, and I find the topic rather peculiarly fascinating.

In the article above, I covered many topics, including one specific paper, the induction of nonclassical monocytes in relation to SARS-CoV-2 infection and how they can mediate the regression of cancer, even metastasis. The Spike Protein itself has neoantigens, antigens that, when your immune cells recognize them, enable your body to fight cancer more effectively. And, of course, not forgetting the original goal of mRNA, which was a personalized cancer vaccine.

So, to my surprise, this was just published in Nature. I will add my thoughts separately.
LNP-RNA-mediated antigen presentation leverages SARS-CoV-2-specific immunity for cancer treatment
In line with previous but sparse evidence, the authors argue here that given the widespread immunity against SARS-CoV-2, especially its Spike Protein due to the mRNA vaccines, they can leverage this immune response as a form of cancer therapy. The reasoning here is that if they present the Spike Protein and its little lego pieces within the tumor microenvironment, pre-existing Spike-specific T cells could redirect themselves and attack the cancer cells within the tumor.
This is in line with the evidence that sometimes, in outlier cases, where the Spike Protein or the virus itself somehow makes its way into a tumor and transforms the tumor from cold (it evades your immune) to hot (it becomes a target and can be killed by your cells).
Most of the LNP used to deliver mRNA to cells is “flawed” from any perspective you look ( does an amazing job on covering this), so the authors created a library (a collection) of new LNPs with different “structures”. These LNPs were then used to treat two types of cells relevant to vaccine delivery: C2C12 myoblasts (representing muscle cells, a primary target for intramuscular vaccination) and JAWSII dendritic cells (DCs, crucial antigen-presenting cells for initiating immune responses).
They measured luciferase expression (it glows inside the cells !!) in these cells to quantify mRNA delivery efficiency. The key finding was that AA2 LNP, particularly lipids with branched ester tails, exhibited superior mRNA delivery compared to other AA lipids and even clinically approved LNPs like SM-102 and ALC-0315 (used in Moderna and Pfizer/BioNTech COVID-19 vaccines, respectively). They tested this new LNP in rates and found the same they did in cells, and also in vivo it had lower off-target distribution, avoiding the liver and spleen.
After finding the best new LNP formulation, the authors went to test the new vaccine response in mice, finding the expected in a sense, compared to Pfizer and Moderna mRNA vaccines, it produce 3.4 and 4.7 higher IgG levels. On the T cell compartment, it produced significant levels of CD4+ T cells compared to Moderna. CD8+ T cells were produced at higher levels but not as drastically. At this point, I firmly believe it is a feature of the mRNA platform.
The next part of their approach is using this already-present immune response towards the Spike and redirecting it to cancer cells. They create a new method of engineering a new molecular that combine the heavy chain of MHC I, microglobulin, and a covalently linked epitope into a single chain. This SCT (single chain trimer) design is aimed at mimicking the presentation of “things” in the cell surface, so here they are “decorating” a cell with Spike Protein.
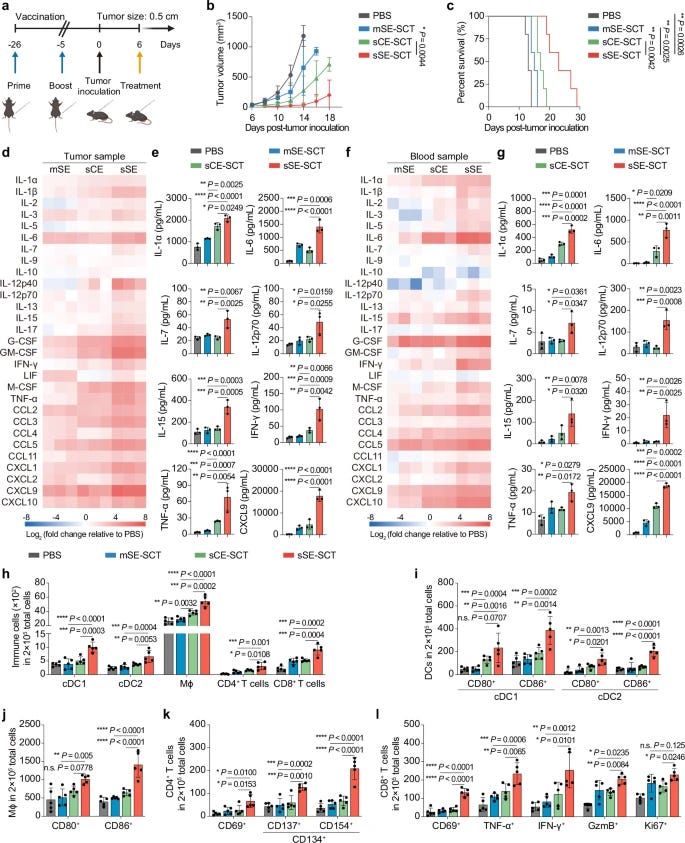
The author used both an mRNA design and a saRNA design (self-amplifying RNA, has been doing an amazing job of covering the bad side of saRNA) to test the efficacy. The saRNA had a superior delivery and more effective expression of this customized Spike to the cell surface. After vaccinating the mice with “normal” Spike Protein vaccine, they inject the mice with melanoma tumor cells, once the tumor took in, the mice were customized AA15V LNP-sSE-SCTs.
A single dose of their customized therapy significantly suppressed tumor growth compared to the control groups, and the one using saRNA was more effective than the one using mRNA, it also significantly extended the overall survival rate of the tumor-bearing mice. By depleting specific T cells to understand which type is responsible for the anti-tumor immunity, they found that CD8+ T cells are the ones responsible for mediating this effect, CD4+ T cells had a less pronounced effect.
Levels of key immune-boosting molecules, cytokines like IL-1α, IL-6, IFN-γ, and chemokines like CXCL9 were significantly elevated in both tumor tissues and the blood. Flow cytometry (used to count and analyze immune cells) showed a surge in immune cell infiltration into the tumor. They saw increased numbers of dendritic cells (cDC1, cDC2), macrophages, CD4+ T cells, and CD8+ T cells.
Antigen-presenting cells (APCs) like DCs and macrophages showed signs of activation (CD80+/86+), and both CD4+ and CD8+ T cells were increased, showing activation markers (CD137+CD134+ on CD4s) and signs of cytotoxic killer function (Granzyme B+, IFN-γ+, TNF-α+, and proliferation marker Ki-67+ on CD8s).

To assess these observations in a “real use case scenario”, the author used human tumor tissue. They treated slices of human glioma and lung adenocarcinoma with their customized therapy. Quantitative analysis showed detectable expression of H-2Kb+β2m+ (a marker for the presented SCT molecules) in a fraction of CD45+ immune cells within these human tumor samples. Evidence that AA15V LNP can effectively deliver sSE-SCTs to human tumor cells. General overview.
AA15V LNP-sSE-SCTs efficiently deliver saRNA to tumor cells, leading to stable presentation of spike epitopes on MHC I.
Pre-existing spike-specific CD8+ T cells, generated by vaccination, recognize these spike epitopes on tumor cells.
This redirected T-cell recognition triggers T-cell mediated cytotoxicity, directly killing cancer cells.
Simultaneously, the saRNA component of LNP-sSE-SCTs activates innate immune responses within the TME, leading to the release of pro-inflammatory cytokines and chemokines.
This TME reprogramming enhances immune cell infiltration and activation, further amplifying the anti-tumor response.
CD8+ T cells are the primary mediators of the anti-tumor effect, but other immune cells and innate immunity also contribute.
Combining AA15V LNP-sSE-SCTs with ICIs synergistically enhances T-cell activity and therapeutic efficacy.
Unlike the aforementioned proposed approach, where some authors argue on using the Spike Protein as a surrogate for a cancer vaccine (therefore immunizing you against potentially developing cancer) this novel therapy aims at treating an already present cancer as an adjuvant therapy, hijacking the widespread use and immunity against SARS-CoV-2 to target cancer.
While the mice were immunized with the full-length Spike Protein for their novel anti-tumor therapy, they used only specific, carefully chosen epitopes (pieces) of the Spike Protein (VNFNFNGL, SIIAYTMSL, VVFLHVTYV, and VVLSFELL), allowing them for precise targeting and predicting of the tumor cells displaying these Spike fragments.
I do find it peculiarly interesting that, so far, all mRNA vaccines using Spike Protein have a significant problem on eliciting broad, strong CD8+ T cell responses, in fact, the primary and most alarming “effect” of the Moderna and Pfizer vaccines was the fact they lowered CD8 levels for months. Even with this rather sophisticated approach, the platform still lacks off-target guardrails, here avoiding the spleen and liver and spleen by using a unique LNP formulation.
Now I wonder myself, if with a very sophisticated, elegant approach, you could engineer a highly customized Spike Protein to target other conditions, especially immune-mediated diseases, for example, B-Cell mediated pathologies, “forcing” the body to wipe out a whole part of B-Cells and resetting that specific immune niche, thus “healing” the autoimmune condition.
Now to less controversial topics (lol). Aspirin is a part of my list of suggestions to treat and avoid sequelae from a SARS-CoV-2 infection. While optional, it is somewhat very effective, extremely cheap, and widely available. It has been proposed for some time that Aspirin has anti-cancer properties, especially anti-metastasis properties, but an accurate mechanism was never proposed before, backed by solid evidence.
Aspirin prevents metastasis by limiting platelet TXA2 suppression of T cell immunity
Metastasis is the spread of cancer cells from primary tumours to distant organs and is the cause of 90% of cancer deaths globally1,2. Metastasizing cancer cells are uniquely vulnerable to immune attack, as they are initially deprived of the immunosuppressive microenvironment found within established tumours3. There is interest in therapeutically exploiting this immune vulnerability to prevent recurrence in patients with early cancer at risk of metastasis. Here we show that inhibitors of cyclooxygenase 1 (COX-1), including aspirin, enhance immunity to cancer metastasis by releasing T cells from suppression by platelet-derived thromboxane A2 (TXA2). TXA2 acts on T cells to trigger an immunosuppressive pathway that is dependent on the guanine exchange factor ARHGEF1, suppressing T cell receptor-driven kinase signalling, proliferation and effector functions. T cell-specific conditional deletion of Arhgef1 in mice increases T cell activation at the metastatic site, provoking immune-mediated rejection of lung and liver metastases. Consequently, restricting the availability of TXA2 using aspirin, selective COX-1 inhibitors or platelet-specific deletion of COX-1 reduces the rate of metastasis in a manner that is dependent on T cell-intrinsic expression of ARHGEF1 and signalling by TXA2 in vivo. These findings reveal a novel immunosuppressive pathway that limits T cell immunity to cancer metastasis, providing mechanistic insights into the anti-metastatic activity of aspirin and paving the way for more effective anti-metastatic immunotherapies.
Aspirin prevents metastasis by directly interacting and limiting TXA2, which participates in clot formation and is produced by activated platelets, macrophages, neutrophils, and endothelial cells. By doing so, it limits the immunosuppressive axis formed by TXA2, which limits the T-Cells activity against cancer cells and metastasis.
It is curious that TXA2 is increased in SARS-CoV-2 infections… so perhaps aspirin should be an option some of you or close family members and friends should consider in different situations (especially if your stomach can handle it…mine can’t, RIP). And as a big proponent of consuming adequate (or more) amounts of salt. Salt is also anti-cancer =).
Sodium chloride in the tumor microenvironment enhances T cell metabolic fitness and cytotoxicity
The efficacy of antitumor immunity is associated with the metabolic state of cytotoxic T cells, which is sensitive to the tumor microenvironment. Whether ionic signals affect adaptive antitumor immune responses is unclear. In the present study, we show that there is an enrichment of sodium in solid tumors from patients with breast cancer. Sodium chloride (NaCl) enhances the activation state and effector functions of human CD8+ T cells, which is associated with enhanced metabolic fitness. These NaCl-induced effects translate into increased tumor cell killing in vitro and in vivo. Mechanistically, NaCl-induced changes in CD8+ T cells are linked to sodium-induced upregulation of Na+/K+-ATPase activity, followed by membrane hyperpolarization, which magnifies the electromotive force for T cell receptor (TCR)-induced calcium influx and downstream TCR signaling. We therefore propose that NaCl is a positive regulator of acute antitumor immunity that might be modulated for ex vivo conditioning of therapeutic T cells, such as CAR T cells.
Do you want to know what, besides everything else, lowers your sodium levels ? A covid infection. Unless you are among the 5% of the global population who are hypersensitive to salt, you should consider adding just a little more to your diet. Your immune system and brain will thank you later, and it is cheap.
Your support is greatly appreciated and enables me to continue my journey of endless curiosity and boundless learning.
The Aspirin paper is new, so I decided to add it as a counter-point to the mRNA/saRNA one, the salt one is also somewhat recent but also good information. Overall, the goal is a "positive" article because the next one ain't. At all. LOL
I will try to avoid publishing it on the weekend...
Thanks.
Idk how mRNA can ever be safely used for anything as at a minimum it causes inflammation? It really hit me.
What about shedding?
As for ASA…. I read a study awhile ago about the combo of vitamin C and ASA taken daily can decrease cancer risks? I can’t remember details. I’m old. lol. Just offering some info I read.
Thanks.
Take Care.