
SARS-CoV-2 and its bacteriophage abilities (and how to address it, and heal yourself)
Science finally catch up to me !

Be warned if you didn’t read my Reverse AIDS series, you might get a little lost in the middle. There is important information about our immune system there, besides the hypothesis.
First, for you to understand why I sound “happy”, refer to this ALMOST 2 YEARS OLD TWEET.
(It does both, it lowers your immune system and helps secondary, and opportunistic infections go rampant and has bacteriophage capabilities or at the very least behaviour)
The impact of SARS-CoV-2 on your gut microbiome/flora is pretty well established, this isn’t a hot topic, but the clinical and scientific evidence to this, which I will now share a recent one.
Alterations in microbiota of patients with COVID-19: potential mechanisms and therapeutic interventions
There is accumulating evidence that the microbiota are significantly altered in patients with COVID-19 and post-acute COVID-19 syndrome (PACS). Microbiota are powerful immunomodulatory factors in various human diseases, such as diabetes, obesity, cancers, ulcerative colitis, Crohn’s disease, and certain viral infections
It is not a mystery what all these diseases have in common, and I have commented, and shared sufficient papers about it, to put it bluntly, and directly they all share a common denominator in a decent portion of the afflicted. The deregulation of your immune response, especially in your gut. From here.
Th17 cells are an important subset of effector T cells that are protective during extracellular bacterial and fungal invasion (83, 88–91). However, excessive Th17 responses are also associated with a variety of pathogenic conditions, depending on the pro-inflammatory cytokines they co-produce (30, 91–95). Littman and colleagues showed for the first time that commensal microbiota play important roles in the development of intestinal Th17 cells (22, 53, 96–100). Th17 development and differentiation is controlled by cytokine and epigenetic regulation (91, 92, 101, 102), but the mechanistic details of microbiome dependent control of Th17 development during mucosal infection is largely unclear.
A number of factors including diverse environmental conditions, intake of diet and medication, as well as host genetic factors determine the dynamic composition of gut microbiota in individuals (103–107). Gut microbiota are capable of restraining the mucosal colonization by enteric pathogens, a process defined as colonization resistance (108). Thus, administration of antibiotics, and altering the resident microbiota during a mucosal infection is known to lead to post-antibiotic expansion of the pathogens. Loss of overall diversity, or even deficit in single group of bacteria can alter the susceptibility to gastrointestinal infections
There are numerous ways your gut microbiome is impacted, and it shifts your immune response, and viral infection can do the same. AIDS causes the reverse of this, it causes a massive dysfunction of your Th17 response, by attacking the mucosal layer of the gut, and causing bacterial translocation, meaning the bacteria has nothing holding it back from moving around and causing a ruckus. Besides the dysfunctional response of your CD8 cells caused by the mRNA, this is the other reason I called it Reverse AIDS.
While rather complex, you need to understand at least this much, about the intricacies of gut health, your immune response, and how infections impact it.
Healthy upper airways are typically populated by Staphylococcus, Propionibacterium, Leptotrichia, Rothia, Dolosigranulum, Haemophilus, Moraxella, Veillonella, and Corynebacterium. Veillonella, Fusobacterium, and Haemophilus are the main genera inhabiting healthy lungs. Prevotella and Streptococcus occur in both upper airways and lungs.5,48,49,50 Evidence from prior research demonstrated that commensal bacteria in the respiratory tract help prevent pathogens from establishing infections and spreading on the mucosal surfaces
Dysfunction or overgrowth of any of these will set off a myriad of symptoms and physiological effects. Prevotella and Covid-19. Before I go any further, the first thing you need to do, in case SARS-CoV-2 hit your gut and causes any disfunction, is to address such changes. Plus everything else I wrote in the Hidden Things series.
The role of glutamine in supporting gut health and neuropsychiatric factors
Recent research has shown that the amino acid glutamine can positively affect gut health by supporting the gut microbiome, gut mucosal wall integrity, and by modulating inflammatory responses. As modulated by the vagus nerve, via the enteric nervous system, the gut-brain connection can impact the brain's neurochemical environment. Poor gut health can disrupt the balance of neurotransmitters, which can result in neuropsychiatric based conditions such as depression. Glutamine supplementation may provide significant adjunctive nutritional support in cases of depression by promoting proper gut health and function.
Another thing, and this one I tested extensively to my own misery (since I had to inflict dysfunction upon myself after Omicron to therefore correct it), is Wheat Bran. Wheat bran will feed the correct bacteria, help to bind what the “bad bacteria” release, which is one of the causes of the hives, and help “scrape off” everything else. It ain’t the most tasteful thing though, eat with some low glycemic fruit like strawberries, blueberries, etc.
The Effects of Intact Cereal Grain Fibers, Including Wheat Bran on the Gut Microbiota Composition of Healthy Adults: A Systematic Review
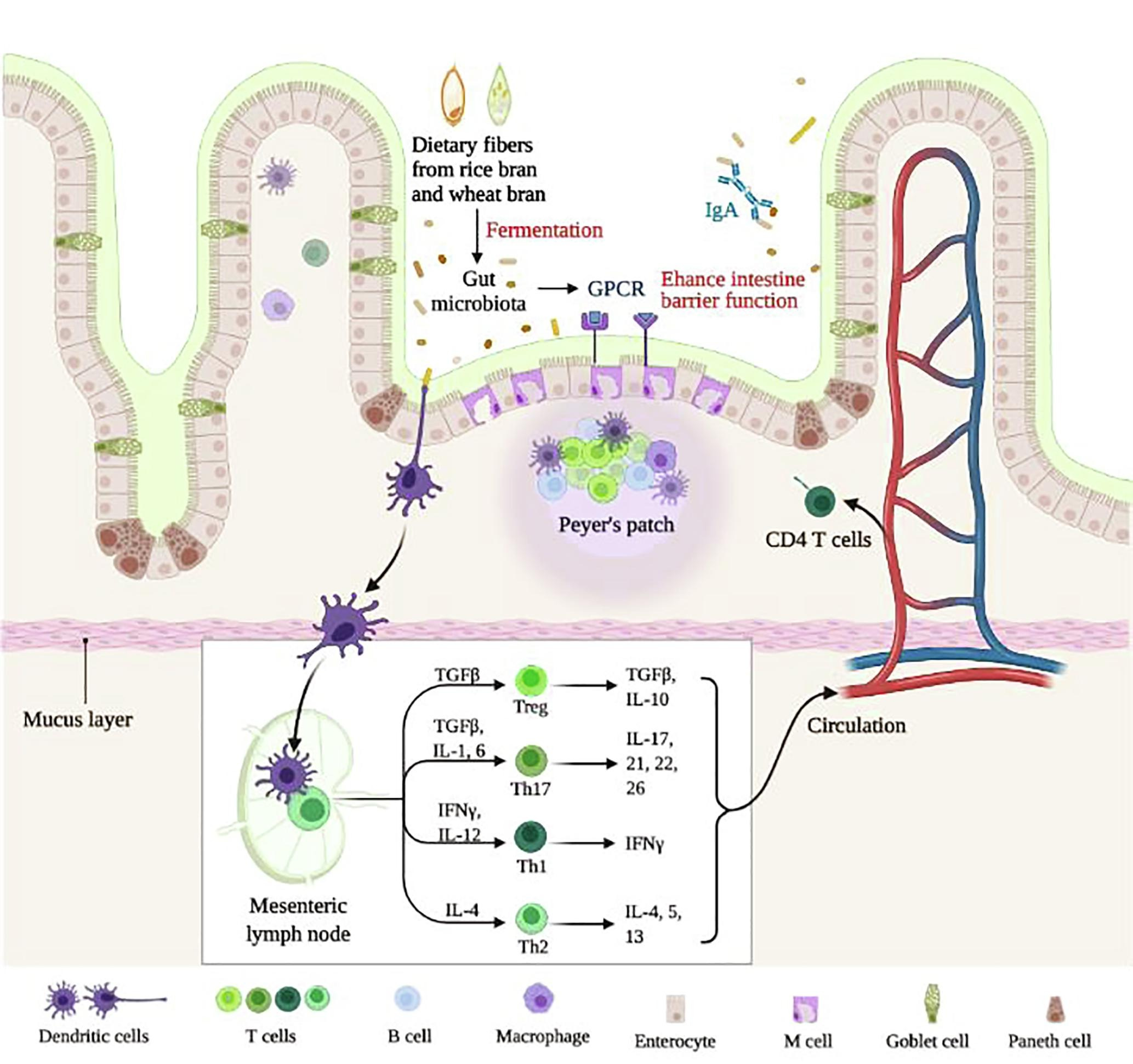
The effects of dietary fibers from rice bran and wheat bran on gut microbiota: An overview
Could SARS-CoV-2 Have Bacteriophage Behavior or Induce the Activity of Other Bacteriophages?
By investigating related metabolic pathways, distinguishable functional signatures in COVID-19 respiratory tract microbiomes were revealed, including decreased potential for lipid metabolism and glycan biosynthesis and metabolism pathways, and enhanced potential for carbohydrate metabolism pathways. The findings also suggested new connections to consider, possibly specific to the lower respiratory tract microbiome, requiring further research on microbial function and host-microbiome interactions during SARS-CoV-2 infection
Authors go to lengths to write to make their point, as is commonplace with uncommon touchy research subjects, listing other papers, which I won’t here, but this part is relevant. I covered this myself quite a few times, how SARS-CoV-2 is a glucose hungry beast, and it will “rewire” your metabolic pathways to use all your glucose around to its replicative purposes, among other things (poor glycemic control will heavily affect the entire outcome of the infection, including inflammation during, and after), and as I covered this before, specific immune cells have metabolic preferences, and Th17 is highly glycolytic (meaning it has a preference and proliferates faster with more sugar around your blood). To the surprise of no one with an internet connection.
Results
Replication and Viral Load Increase of SARS-CoV-2 in Bacterial Cultures
The curves of replication and viral load increase of SARS-CoV-2 in bacterial cultures are shown in Figure 1, Panels A and B, with the permission of Dr. Petrillo [7]. In particular, three couples of fecal samples from different “infected donors” (i.e., sources of A) and “healthy recipients” (i.e., sources of B) have been recruited, and subject to the same experimental procedure described in the Materials and Methods section. All combinations of “infected donors” sources (A1, A2 and A3) and “healthy recipients” donors (B1, B2 and B3) were subject to the same experimental procedure. Although with certain differences, the observed trends were similar (Figure 1A), confirming the increase over time of SARSCoV-2 RNA load in samples of type A and in samples of type B (A+). Lastly, for each “recipient”, SARS-CoV-2 RNA load was measured (Figure 1B). The results report virus replication in bacterial cultures suggesting that this virus behaves as a bacteriophage.
This paper has some flaws in my opinion, but the researchers are taking a step in the right direction, just wanted to be clear about this.
Translating from science-speak, it means that samples from infected donors were tested using an experimental procedure, and at the end of the experiment, there was more RNA detectable in those samples than in healthy donors.
In particular, the green signal corresponds to the Gram-positive bacteria that are shown in the images in panels C, F, H. The red signal indicates the nucleocapsid protein of SARS-CoV-2. In panels D, G, and I, the same bacteria shown in the previous panels are shown. Since these are labeled with this signal, it means that they are infected with the virus. The confirmation is obtained from the overlay/merge fluorescence shown in panel E in which the Gram-positive bacteria (signal with green light- in panels C, F, and H) were attached to viruses likeparticles of SARS-CoV-2 (signalled with red light, in panel D, G, and I). In panels F and H, it is possible to observe the computerized magnifications of the bacteria indicated with numbers 1 and 2 that appear green because they are marked with the anti Gram-positive antibody. Similarly, panel G is a computerized magnification of the bacteria attached by SARS-CoV-2 indicated with the numbers 1 and 2. The negative control of the culture obtained without primary antibodies but only with secondary antibodies is shown in panel L. Panel M is the merge of the negative control of a healthy fecal bacterial culture
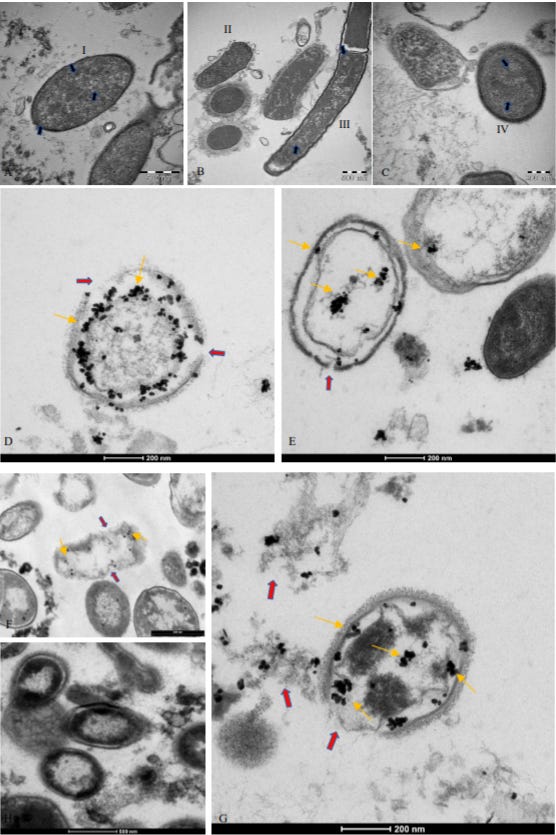
Describing the findings, and a visualization of the same.
For example, some past studies have observed a co-participation of bacteria in the infection of another RNA virus such as HIV [22]. In addition, recent studies have observed the presence of HIV in intestinal mucosal lymphoid tissues.
In a recent case report, it was reported that 500 days after recovering from Ebola virus (fecal-oral RNA virus), an African boy sexually transmitted the virus to a woman [24]. One would wonder: how is this possible? Where was the Ebola virus hiding?
The answer won’t be accepted for years to come, I covered Ebola before, and just now the community is accepting its latent potential, HIV, and EBV are well known to be latent, and chronic viruses. There are a few mechanisms for viruses to stay hidden inside you, immune evasion, infecting immune cells (HIV), immune suppression (EBV), and hiding in specific tissues, but the main point here would be one I covered once. Biofilms.

This paper and previous evidence give weight to my (once upon a time) insane hypothesis of this particular virus, SARS-Co-V, being a bacteriophage or possessing the capabilities (behavior) of one. What is happening in my opinion, and the authors will propose this too, is that this interaction is creating enterotoxins. Toxins are created inside you, from your own cells, bacteria living inside you because of the interaction of invading pathogens, cell signaling, and stress (both on a physical/hormonal to a cellular level).
Some people who talk to me directly can attest to this, I have been on about it for close to 2 years.
Interestingly, at that time, a group of researchers observed how bacteria might play a role in the selection of a few different strains of poliovirus. They observed that bacterial endotoxins induced a lower rate or even inhibited viral replication [35]. Similar to our studies , we highlighted several toxin-like proteins in the plasma, feces, and urine of COVID-19 patients, which were produced by bacteria as a consequence of interaction with SARS-CoV-2. We have shown that these oligopeptides are derived from bacterial cultures and we are testing them in mice (data in preparation). We have already observed the replication of SARS-CoV-2 virus in bacteria many times and have conducted some experiments with Nitrogen Isotope 15N in the bacteria culture in the presence of this virus to better understand this phenomenon . This finding is reported in another of our works, concerning the spike protein and the nitrogen isotope present in it [36]. Furthermore, we found that after 30 days of bacterial cultures, using a previously published methodology, some bacterial genera tend to increase and others tend to decrease. These data suggest that the increase in viral load, as previously shown by Petrillo et al., in bacterial cultures, is associated with a decrease in some bacterial genera after 30 days, perhaps is due to the lytic cycle of these bacteria . We found that some bacterial genera, such as Dorea, Fusicatenibacter, Klebsiella, and Streptococcus decreased, while other genera, such as Campylobacter, Prevotella, Staphylococcus, Bacteroides, and Cytobacter increased.
nasopharyngeal commensal bacteria including Gemella morbillorum, Gemella haemolysans, and Leptotrichia hofstadii were significantly depleted in the pharynges of COVID-19 patients, whereas bacteria such as Prevotella histicola, were relatively increased.
However, it must be considered that the interaction between bacteria and SARS-CoV2 does not necessarily occur with native viral surface proteins, but most likely with a surface reworked by proteases and toxins produced by bacteria. A likely explanation for this novel interaction between bacteria and coronaviruses could be based on the highly dynamic process generated between bacterial products (toxins, metabolytes, oligopeptides, proteases) and viral proteins
I, and some people with +10.000 hours of clinical care of Covid-19 patients, and much much much smarter than me agree with this assessment, with evidence behind it, alas they refuse to publish, or even tangentially share it. These closing paragraphs are pretty much aligned with my, and the aforementioned doctors observations.

As per the tweet I shared, very early on I insisted on the reinfection happening, at the bacteriophage stage of this virus, and also early on about the chronic aspect of this virus. And this entire paper and piece give credence to these ideas. Some people will get hit harder than others, your metabolic health, gut health, nutrient availability, and your own microbiome will impact the outcome of these interactions.
I don’t believe SARS-CoV-2 can replicate inside bacteria, but I believe it can use them to modulate your own immune system, and more interestingly stay hidden, per my Into the Chasm tweet. And the more worrisome trend would be to recombine inside biofilms, and bacteria themselves.
Since this is a fairly big piece, and complex, to simplify, there is extensive evidence SARS-CoV-2 influences, severely impacts the microbiome of some of the infected, the more severe, the more impact, and mostly contributes to the Long Covid cases, which usually share similar gut issues, even if at a subclinical level. This paper lay the groundwork for further research on said mechanisms, and what that can mean to the pandemic (and overall to current biology dogma too).
Secondary bacterial infections are fairly common, really important to pay attention to, and they modulate your immune system, further shift it towards “the wrong” response, and also cause a change in your microbiome, this is an important research topic, and one I usually pay close attention to (even though I missed this paper lol).
This also pertains to strains before Omicron, Omicron has a predilection towards hitting the gut, and the newer strains for even longer (4 weeks), but the “sample data” is now relatively contaminated (heh), because we don’t know what the vaccines do in all this, I have my own hypothesis, but that doesn’t mean I am 100% right, we need more time, and research to actually measure what Omicron does to the gut, and if it has the same behavior.

As a final note, as a proponent of low carbohydrate diets to help, well, with everything, I do not recommend you go strictly to super low carbs for long (that will also bring changes to your microbiome, sometimes good, sometimes not pleasant), but carb cycling. Eat A LOT of carbs 1 day per week, perhaps a day and a half, with more protein when you eat lower carbohydrates.
You can buy me a coffee whenever you feel like it.
Deep appreciation for all the supporters!
its funny how often the words toxins and polio pop up together...
Wow this is a great article - the microbiome is so fascinating. This would explain a lot of what happened in my own family when infected with what we assume was Omicron. Those of us with gut issues (Celiac disease, IBS) were more severely impacted.
What would you suggest for someone with Celiac disease who wants to improve microbiome? I have tried finding rice bran but it's hard to find in my part of the world.