
Prophylactic Ivermectin works against SARS-CoV-2
And modular vaccine laboratories

I usually abstain from “memetic” posts, but this one deserves it. Nature-published paper can be found here. As a peculiar side note, I highly recommend you to google Satoshi Oumura, one of the authors of the paper.
Another one on the long list of “We told you so”, from Vitamin D, to C, to HCQ, among many others.



But this is more egregious than most of the others, together with HCQ (a drug that can factually, and scientifically be described as an anti-mRNA adverse-effects intervention) was absurdly politicized globally.
The paper has interesting findings because it is a prophylactic “treatment” using Ivermectin. A summary of the main points, the paper itself is short, but with substance.
Prophylactic administration of ivermectin prevents weight loss in a hamster model of SARS-CoV-2 infection
Analysis of body weight changes after inoculation demonstrated that hamsters infected with SARS-CoV-2 had temporary weight loss which peaked on the 7th day of infection. However, weight loss was suppressed in hamsters orally administrated ivermectin prior to inoculation (Fig. 1b). These results indicate that oral administration of 1 mg kg−1 ivermectin in hamsters acts prophylactically against SARS-CoV-2 infection and prevents weight loss after viral infection.
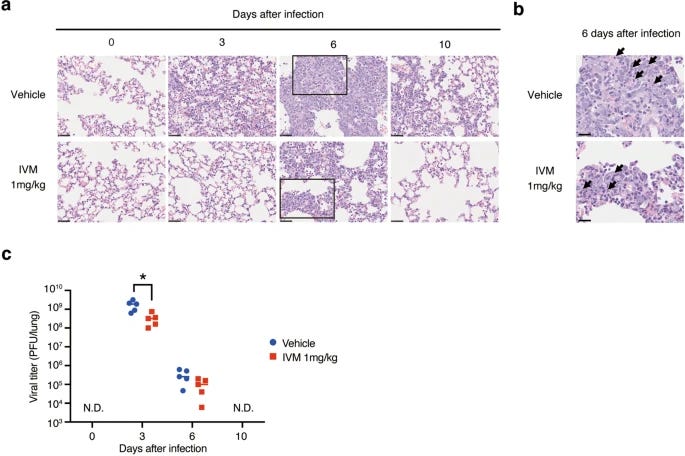
Prophylactic administration of ivermectin reduces pulmonary disease in a hamster model of SARS-CoV-2 infection
Viral titers in the lungs of ivermectin-treated hamsters were reduced by a factor of 10 compared to vehicle-treated hamsters on days 3 after infection (Fig. 2b) .These results indicate that prophylactic administration of ivermectin reduces pulmonary injury and viral titers in a hamster model of SARS-CoV-2 infection.
Prophylactic administration of ivermectin inhibits pulmonary expression of inflammatory cytokines in response to SARS-CoV-2 infection
Expression of pro-inflammatory cytokines, such as Il6 in the early stage of viral infection and Tnf in the late stage of viral infection, were decreased in ivermectin-treated hamsters (Fig. 3a, b). On the other hand, expression of the immunosuppressive cytokine, Il10, or the interferon-inducible transcription factor, Irf7, remained unchanged (Fig. 3c, d).These results suggest that ivermectin suppresses the expression of inflammatory cytokines associated with SARS-CoV-2 infection at the genetic level.
Prophylactic administration of ivermectin reduces the severity of pathological changes associated with SARS-CoV-2 infection
We further measured virus neutralizing antibody titer in plasma on 10 day after infection, which we considered the recovery period. Plasma titers of neutralizing antibodies were significantly higher in ivermectin-treated hamsters compared to vehicle-treated hamsters. In addition, ivermectin-treated animals had higher zinc concentrations in lung suspensions on day 3 after infection, with a similar trend observed 10 days after infection. These results suggest that prophylactic administration of ivermectin has multiple effects that lead to a reduction in the severity of pathological changes associated with SARS-CoV-2 infection.
In short, the prophylactic administration of IVM reduces the viral load and damage to the lungs, it also inhibits the pulmonary inflammatory response by lowering the levels of Interleukin-6 at the early stages of the infection, IL-6 is one of the biggest contributors to both damage and disease progression, it is the “main player in town” at the start of the infection, and also lower TNF (Tumor Necrosis Factor) at the later stages of the infection, similar to IL-6, this one is responsible for much of the damage in the severe stages of the disease, also a big contributor to long-term consequences of the viral infection.
It also increases the levels of neutralizing antibodies, so IVM is not immunosuppressing, but immuno-modulating in a very beneficial way, without negatively impacting a proper, robust immune response, it also increases the level of pulmonary zinc, something very beneficial in respiratory infections.
Once more, this isn’t exactly “news” dozens of scientists and hundreds of clinicians could attest to both the potential mechanism by which IVM was beneficial and the real-world positive impact of using the drug to treat patients. But more evidence is always good.
Now, since I don’t like sending multiple e-mails in one day. At first, I was deeply concerned, but now I am… intrigued and concerned.
In February, the Telegraph visited the first factory to be built from shipping containers in Marburg, Germany – and now an identical factory is being bolted together in the Rwandan capital of Kigali.
It’s the “first node in a decentralised and robust end-to-end [vaccine] manufacturing network in Africa”, says BioNTech.
Senegal and South Africa are expected to be next and a deal has been struck with Australia, which will take delivery of an identical facility next year. Eventually the new factories could be dotted all around the world.
“In the long run, I see this could be a very large local network,” said Sierk Poetting, chief operating officer at BioNTech SE. “You could imagine maybe BioNTainers closer to clinics and hospitals and so on [around the world].
“In the next two, three years, it’s probably like a smaller network … Rwanda, African countries, Australia and so on.”
If the factories work – and with the right people running them they should – Africa will soon have the capacity to produce hundreds of millions of vaccine doses within its borders
BioNTech’s vaccines are made from mRNA where no brewing is required. Once the genetic code for the jab has been designed and tested, they are cheaper, quicker and more reliably produced than conventional vaccines as the process is essentially a matter of chemistry.
A single 50 litre bag of mRNA made here is enough to produce five million doses of vaccine, with the “finish and fill” conducted at separate specialist facilities.
The same factories could even produce mRNA cancer vaccines of the sort currently being trialled in the NHS by BioNTech.
“As long as the vaccine is approved and made from mRNA, it can be manufactured in one of these facilities,” says Mr Brunen.


After finding and reading the article above, my first thought was of concern. It is self-evident and clear by any metric that the “tides of public opinion” are turning at an ever-growing rate, it is now impossible to hide the many, many problems with the mRNA platform, all the drawbacks, and everything in between, regardless of how politicized it is (and ever was, really).
Superficially within minutes, my first overall assertion was “If someone hired me to build portable dual-use labs, this is exactly how I would do and design them”, in fact, I even have it sketched in one of my notebooks. It is like your own, private, bioweapon factory, portable, modular, efficient, fast assemble, and needs few personal.
Doorless Carp, a friend of this Substack and a great scientific resource shortly sent me this. The following is also his commentary.
So there is no precautionary principle here, in effect, even for treating less severe conditions than say late-stage cancer. That's a hard No! Consultation on Point of Care Manufacturing Updated 25 January 2023
Screenshot (official governmental) source here.
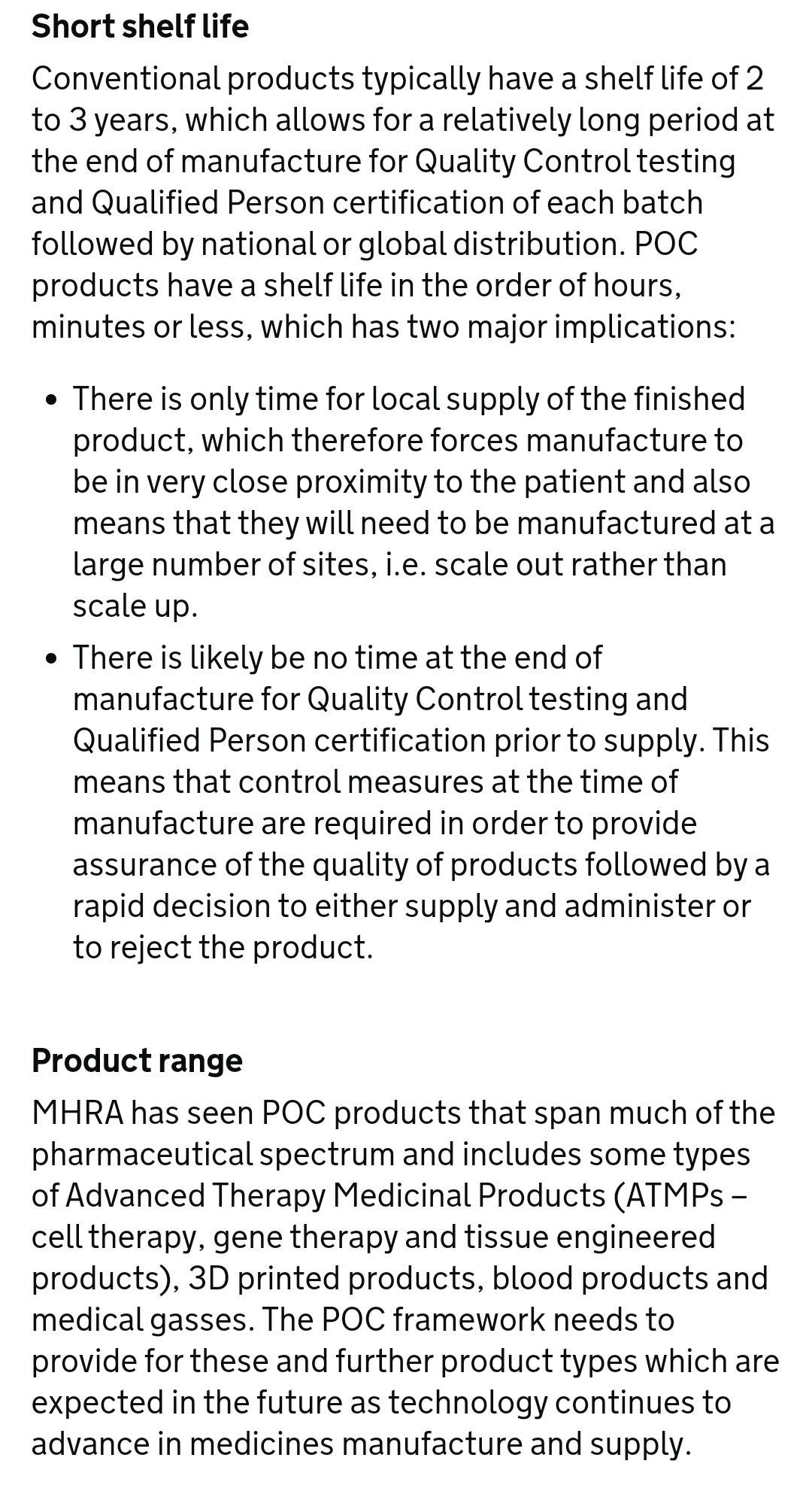
QC is not tossed out of the window unless it is an emergency, and yes I am fully aware of the false arguments by pharmaceutical companies and corrupt governmental bodies, not the focus right. This leads me to reassess my first observation. A decentralized modular approach would make perfect sense if, by different metrics and systems, governments expect a huge increase in bioincidents and bioterrorism, something not unheard of, I have been warning about it for years (and forecasting many of the events publicly, and others privately for myself.
The UN, DoD, and many other organizations also expect an increase in biological events in the coming years, so forecastings of the sort are not unheard of, or products of small forecasters. With the advances of AI in the past weeks (the subject of my next substack) it isn’t a surprise in the potential increase of these events.
A modular lab would be able to respond quickly to any “threat”, and epidemiologically speaking, high mortality viruses can’t “espace” their regional breakouts, responding to these hypothetical outbreaks quickly makes strategic sense. There are other problems with such modular labs, vetting the personnel involved would be one of the biggest, and security and logistical feasibility would be close next. Containers are not known to be paramount to security.
The right “payload”, just a little bit of knowledge and you have millions of doses of…something.
Something to think about.
Grateful for anyone who chose (or could) support this Substack, helps my work a lot ! And to anyone who shares it.
Hmmm, I used IVM as a prophylaxis for 2.5 years by taking it once a week. It's effective.
Yes! Even if naysayers claim it doesn’t stop covid it still has strong anti inflammatory effects that offer relief and can still save lives.
It is evil to suppress its usage and it’s still ongoing today.