

I do rather share a short yet positive article, before the next one, so here we are. First, the good news, incidentally giving evidence for early suggestion I had.
2 years ago I wrote multiple, to the detriment of my “peers” that many people would simply recover from the mRNA vaccine because most people were minimally damaged, if they avoided the initial cycle of disease, that being vaccine → second dose → immune depression → infection by SARS or another pathogen → secondary infection → tertiary infection → severe damage, autoimmunity, cancer sets in, they would be “mostly” fine.
Effects of BNT162b2 mRNA Covid-19 vaccine on vascular function
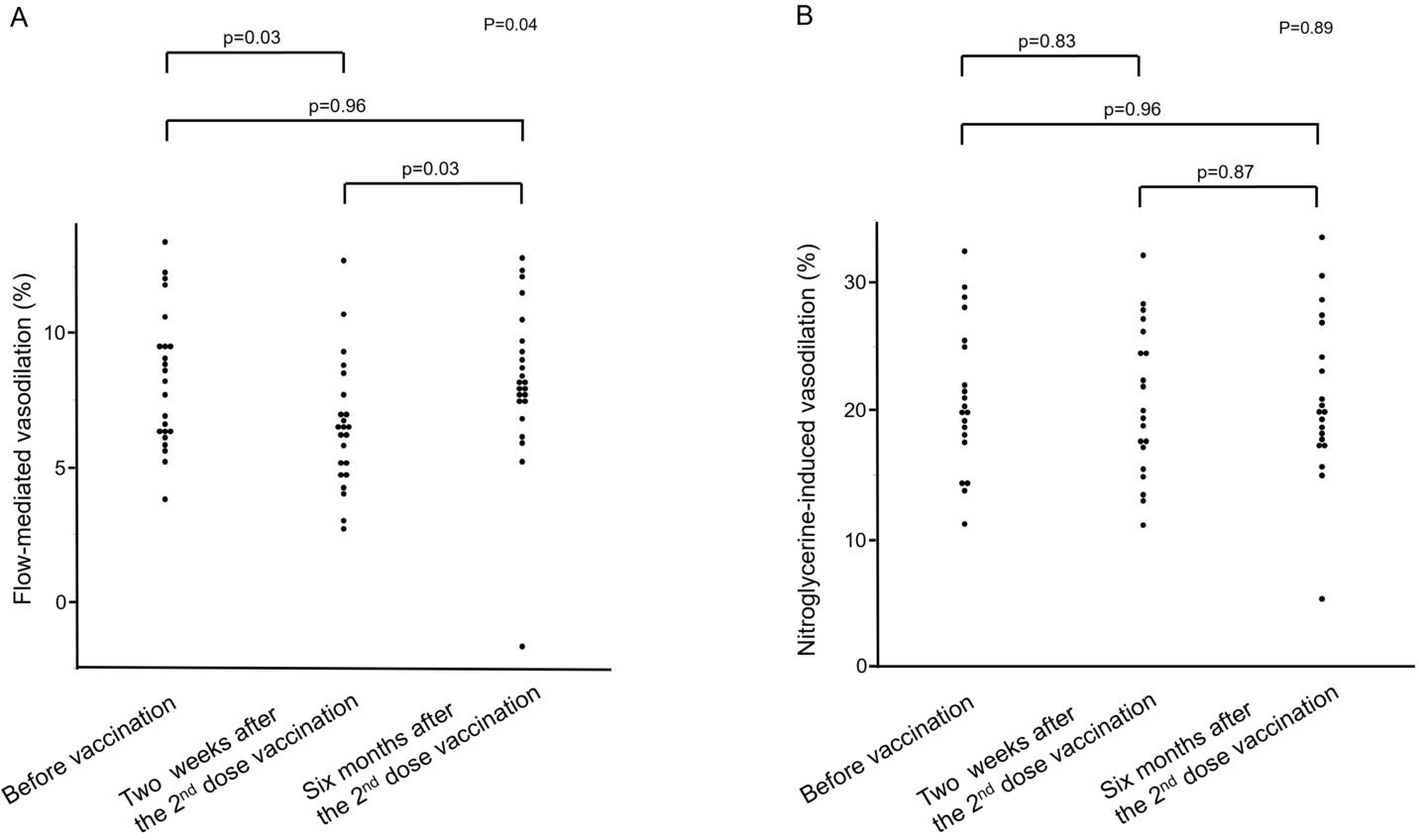
The effects of Covid-19 vaccines on vascular function are still controversial. We evaluated the effects of BNT162b2 vaccine (BioNTech and Pfizer) on endothelial function assessed by flow-mediated vasodilation (FMD) and vascular smooth muscle function assessed by nitroglycerine-induced vasodilation (NID). This study was a prospective observational study. A total of 23 medical staff at Hiroshima University Hospital were enrolled in this study. FMD and NID were measured before vaccination and two weeks and six months after the 2nd dose of vaccination. FMD was significantly smaller two weeks after the 2nd dose of vaccination than before vaccination (6.5±2.4% and 8.2±2.6%, p = 0.03). FMD was significantly larger at six months than at two weeks after the 2nd dose of vaccination (8.2±3.0% and 6.5±2.4%, p = 0.03). There was no significant difference between FMD before vaccination and that at six months after the 2nd dose of vaccination (8.2±2.6% to 8.2±3.0%, p = 0.96). NID values were similar before vaccination and at two weeks, and six months after vaccination (p = 0.89). The BNT162b2 Covid-19 vaccine temporally impaired endothelial function but not vascular smooth muscle function, and the impaired endothelial function returned to the baseline level within six months after vaccination.
As we say here, “Not everything is flowers” meaning uncertainties and difficulties exist. Individual factors play a significant role here, and even though the vast majority of mRNA vaccinated recover from their impaired endothelial function, a period of 6 months of impaired function entails other forms of correlated damage occurring.
Cardiovascular events, heart failure, other endothelial dysfunction-related diseases, and of course, clots. Authors themselves wonder the same we have been saying since day 1, the vaccine may minimally affect healthy people, but will likely accelerate problems for any person who already has an underlying condition. Also one has to wonder the narrative warfare between the vaccine worsens and whether the vaccines help Long Covid groups, evidence points towards both.
Do you know what helps with Long Covid, endothelial dysfunction, and mRNA damage regardless ?
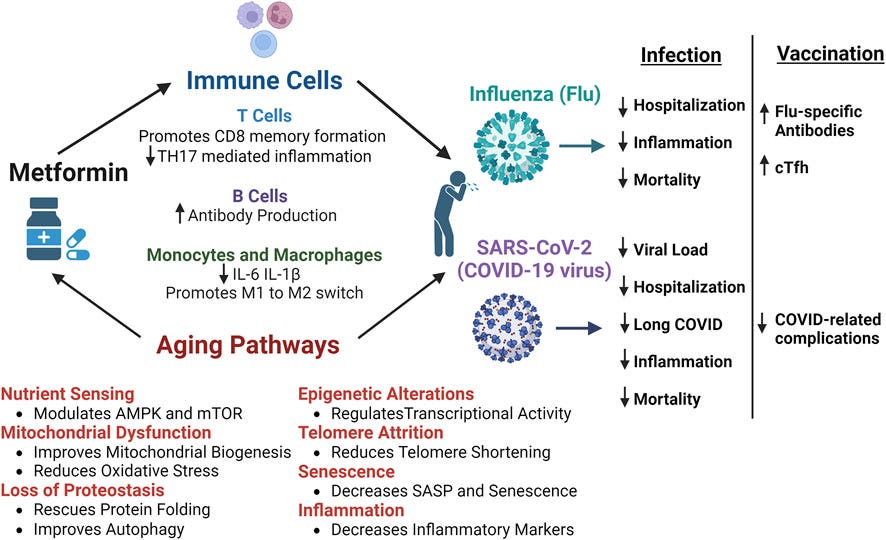
Favorable Antiviral Effect of Metformin on Severe Acute Respiratory Syndrome Coronavirus 2 Viral Load in a Randomized, Placebo-Controlled Clinical Trial of Coronavirus Disease 2019
Methods
COVID-OUT was a 2 × 3 randomized, placebo-controlled, double-blind trial that assessed metformin, fluvoxamine, and ivermectin; 999 participants self-collected anterior nasal swabs on day 1 (n = 945), day 5 (n = 871), and day 10 (n = 775). Viral load was quantified using reverse-transcription quantitative polymerase chain reaction.
Results
The mean SARS-CoV-2 viral load was reduced 3.6-fold with metformin relative to placebo (−0.56 log10 copies/mL; 95% confidence interval [CI], −1.05 to −.06; P = .027). Those who received metformin were less likely to have a detectable viral load than placebo at day 5 or day 10 (odds ratio [OR], 0.72; 95% CI, .55 to .94). Viral rebound, defined as a higher viral load at day 10 than day 5, was less frequent with metformin (3.28%) than placebo (5.95%; OR, 0.68; 95% CI, .36 to 1.29). The metformin effect was consistent across subgroups and increased over time. Neither ivermectin nor fluvoxamine showed effect over placebo.
Conclusions
In this randomized, placebo-controlled trial of outpatient treatment of SARS-CoV-2, metformin significantly reduced SARS-CoV-2 viral load, which may explain the clinical benefits in this trial. Metformin is pleiotropic with other actions that are relevant to COVID-19 pathophysiology.
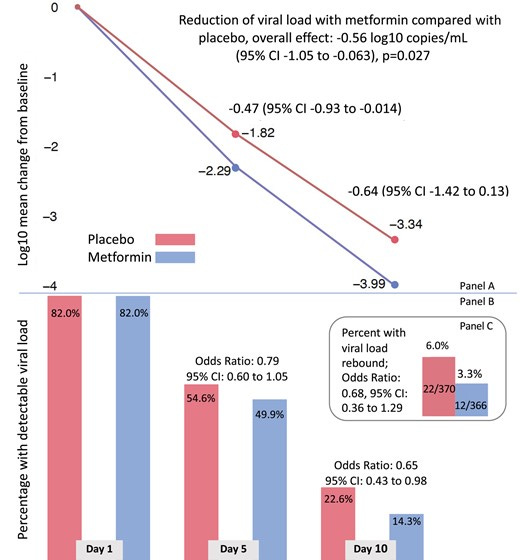
The “best” part of this paper is that it includes vaccinated, non-vaccinated, and a surprising minority of boosted, and even when adjusting to vaccination status, time since the last vaccine, other medications, etc the results were similar. Metformin exerts an antiviral effect on SARS-CoV-2 infection, with people on Metformin being less likely to have detectable viral load than those who didn’t. Interestingly, 12 people experience viral rebound while under metformin, and 22 on control.
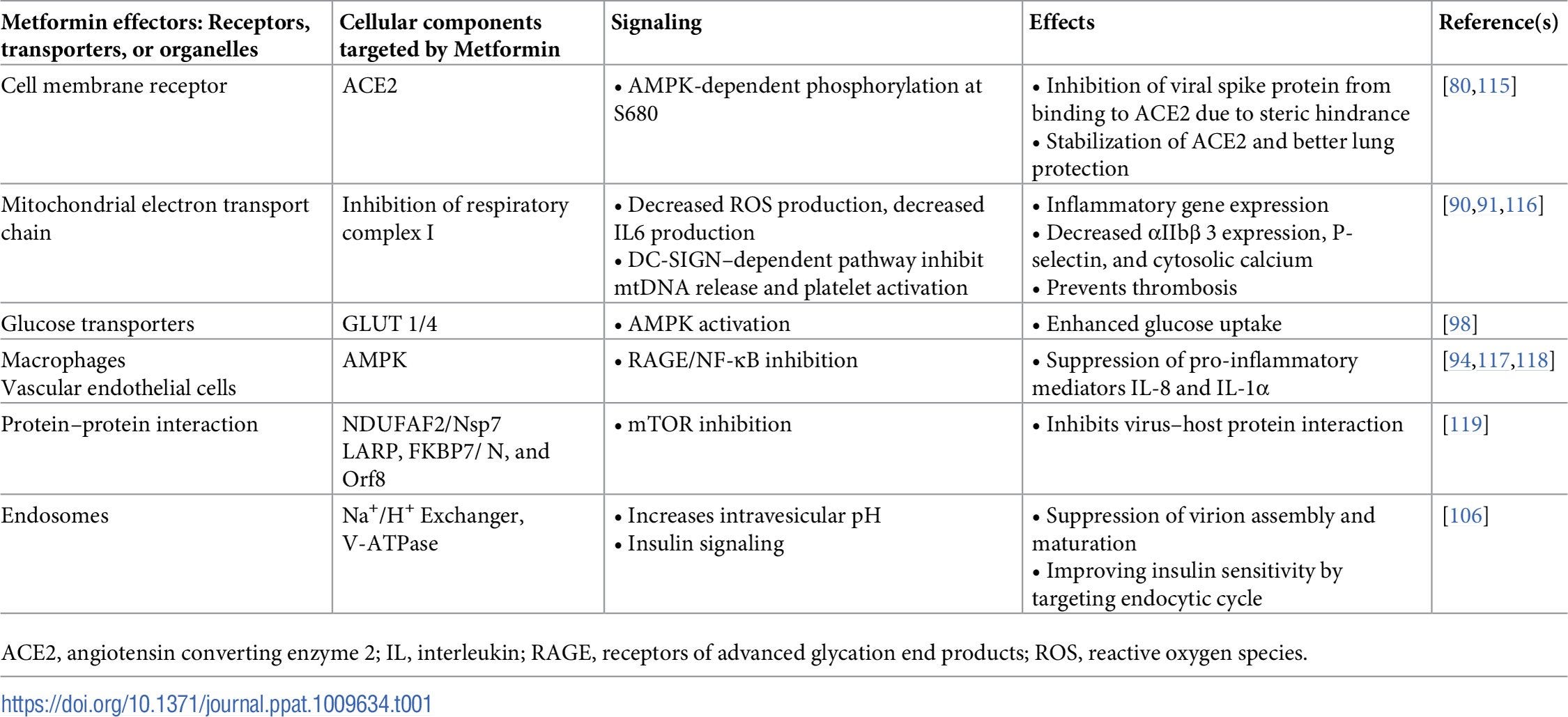
The authors further mention the other non-specific effects of Metformin, such as inhibition MTOR, Interleukin-6 (potent inflammatory protein), Tumor Necrosis Factor Alpha (Also potent inflammatory protein) in the presence of LPS, and the presence of LPS is correlated with severe Covid (and vaccine injury…), it also can increase IL-10 (anti-inflammatory) among other effects also in the presence of LPS.
I have covered Metformin multiple times before, but some were a biochemical/pharmacological approach, others small observational studies, this is one of the first published “actual trials”.
The following are screenshots I made in mid-2021
Given how prominent the avian flu talk is right now (separated article later this week), Metformin also helps with influenza.



Always remember, Berberine is an almost perfect analog to Metformin, with just a few differences, and specific pathways that each target, but on principle, they act very similarly. So can’t access/don’t want Metformin, Berberine is the next best choice, for some sometimes it is THE better choice.
Do you know what else I have been suggesting the usage and supplementation of, also since 2021 ? Exogenous Ketones, specifically Beta-Hydroxy Butyrate.


Oral beta-hydroxybutyrate alleviates COVID-19 related acute respiratory distress syndrome: A randomized, single-blind, placebo-controlled trial
Methods
We randomized 75 patients with mild (as per Berlin criteria) ARDS symptoms to receive oral 25 g twice daily or placebo for five days. The primary outcome was the change in pro-inflammatory cytokines (Interleukin-1β, Interleukin-6, interleukin-18, tumour necrosis factor-alpha) and anti-inflammatory cytokine (interleukin-10) from baseline to day 5. The secondary outcomes were the change in BHB levels from baseline to day 5, the number of hospitalization days, and the occurrence of adverse events.
Results
Treatment with formulated BHB resulted in a significant decrease in pro-inflammatory cytokines; Interleukin-1β (p = 0.0204), Interleukin-6 (p = 0.0309), interleukin-18 (p = 0.0116), tumour necrosis factor-alpha (p = 0.0489) and increase in interleukin-10 (p = 0.0246) compared treatment with placebo. Importantly, higher BHB levels (p = 0.0001) were observed after supplementation; additionally, patients who underwent this approach were hospitalized for fewer days. No serious adverse events were reported.
Conclusion
Beta-hydroxybutyrate, an oral adjunct therapy, has shown promising results in ameliorating symptoms of ARDS. This includes reduced inflammation, oxidative stress, and decreased patient fatigue levels. Further study with a large sample size is warranted to assess the potential of BHB therapy's effectiveness in reducing the development of severe illness.
A “simpler” trial but we finally have published evidence from a properly designed trial using BHB (Beta-Hydroxybutyrate, a ketone) as an intervention. Here they measured pro-inflammatory markers, the most important ones, and correlated with lower levels of each of the most important ones, with an increase of Interleukin-10, basically bringing “balance” to the inflammatory process.
In indirect ways, BHB will also possess antiviral effects by modulating both your T-cell metabolism, and your mitochondrial metabolism, and shifting your usage of sugar. One of the most potent and recently researched effects of a ketogenic diet or using ketones as a supplement is its neuroprotective effects, from ameliorating Alzheimer’s to basically reversing anxiety and depression (after 12 weeks, very recent trial).
Similar to Metformin, BHB will directly and positively affect influenza outcomes. KD-mediated immune-metabolic integration represents a viable avenue towards preventing or alleviating. BHB directly inhibits glycolysis in multiple tissues, such as heart, brain, skeletal muscle, and in tumors, the list goes on.
Since we talked about endothelial dysfunction.
Also remember, there is no “single magic bullet”, treating any form of infection with natural compounds and supplements is a “group effort”, you quite literally stack things together, preferably that synergize and achieve the desired outcome of minimizing damage/severity.
I will also explain my thoughts behind the next suggestion but I suggest you the reader buy some Olive Leaf Extract 20% Oleuropein and stock it, if you intend to take it, buy extra and save it.
I am grateful for your support, thank you ! And as a last suggestion, put this on the maximum resolution your display can handle, full-screen, and just watch it, based on one of my favorite books. It is great… if you can remember anything by the end of it =).
Next few ones... not so great news. Interesting from a scientific perspective, not exactly uplifting.
I wish everyone a great rest of the week.
as you know I am a fan of metformin. Form 'goats rue' or galega officinalis used since the 13th century.