
Inflammaging, SARS-CoV-2 and HSCs
Molecular nuclear bomb

For many weeks now I have been meaning to write a specific piece, that as usual would link to the bigger picture, another piece of this puzzle, and a minuscule piece of the biggest puzzle of all. Life.
What pushed me to decide to write this one today of all days, was this paper.
Highlights
Some relatively healthy individuals mounted weak responses to BNT162b2 vaccination
“Low responders” had impaired spike-specific antibody, B and T cell responses
Transcriptomic analysis revealed evidence of premature lymphocyte aging
Premature lymphocyte aging could reduce vaccination efficacy
SARS-CoV-2 vaccines have unquestionably blunted the overall impact of the COVID-19 pandemic, but host factors such as age, sex, obesity, and other co-morbidities can affect vaccine efficacy. We identified individuals in a relatively healthy population of healthcare workers (CORALE study cohort) who had unexpectedly low peak anti-spike receptor binding domain (S-RBD) antibody levels after receiving the BNT162b2 vaccine. Compared to matched controls, “low responders” had fewer spike-specific antibody-producing B cells after the second and third/booster doses. Moreover, their spike-specific T cell receptor (TCR) repertoire had less depth and their CD4+ and CD8+ T cell responses to spike peptide stimulation were less robust. Single cell transcriptomic evaluation of peripheral blood mononuclear cells revealed activation of aging pathways in low responder B and CD4+ T cells that could underlie their attenuated anti-S-RBD antibody production. Premature lymphocyte aging may therefore contribute to a less effective humoral response and could reduce vaccination efficacy.
At no moment whatsoever the authors even thought of linking this as a direct vaccine effect, and not the other way around as they attempt to describe. You also have very little chance to understand everything about to be discussed here if you don’t read the following one, or merely the paper referred to in the title. And as I said many times in the last 6 months, this was one of the most important papers on SARS-CoV-2 to date.

Aging also causes dysfunctional hematopoietic cell differentiation, and the Myc family members have an important role in B and T cell differentiation signifying additional deficiencies in the development of the immune response after vaccination. Low responders had fewer spike-specific antibody-producing B cells compared to controls, even after booster, indicating an attenuated amnestic response.
Interestingly, CD4+ T cells in low responders have augmented inflammatory pathways (e.g., TNF, IFNG, etc.) compared to controls in the scRNA-seq analysis, and this pattern is consistent with a senescent-associated secretory phenotype that is the hallmark of inflammaging.
The paper I am about to discuss that set off this whole endeavor was once again sent by the same person I often collaborate with.
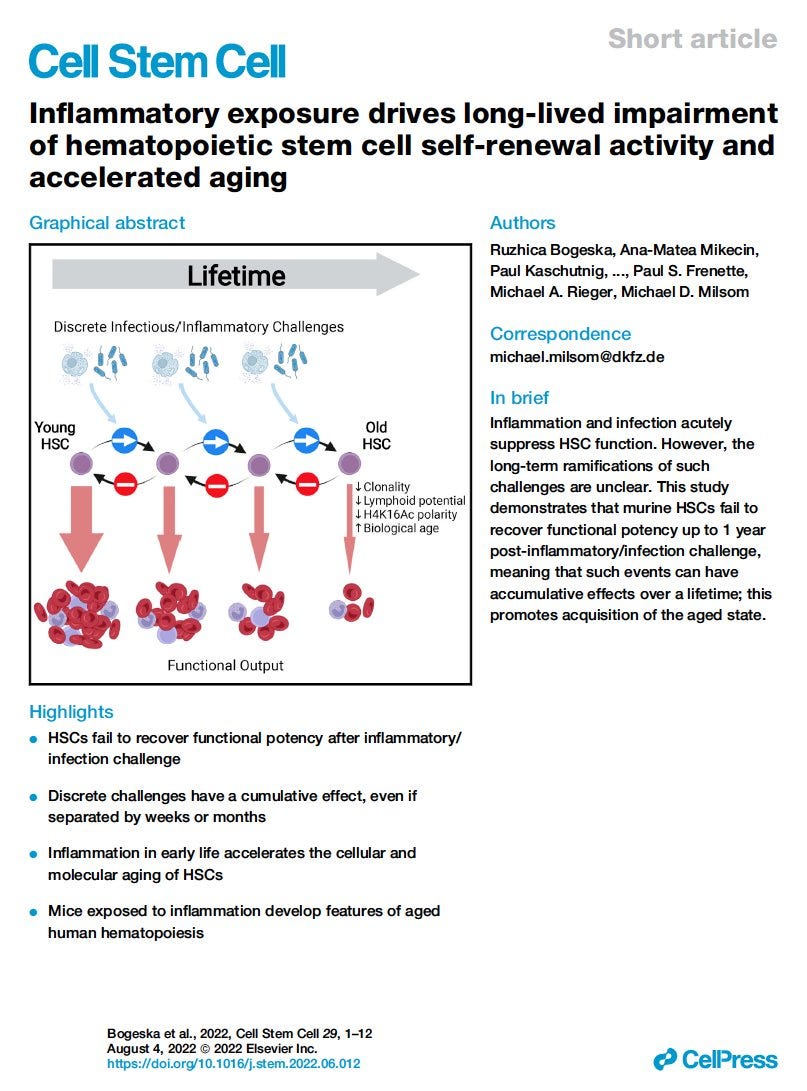
Hematopoietic stem cells (HSCs) mediate regeneration of the hematopoietic system following injury, such as following infection or inflammation. These challenges impair HSC function, but whether this functional impairment extends beyond the duration of inflammatory exposure is unknown. Unexpectedly, we observed an irreversible depletion of functional HSCs following challenge with inflammation or bacterial infection, with no evidence of any recovery up to 1 year afterward. HSCs from challenged mice demonstrated multiple cellular and molecular features of accelerated aging and developed clinically relevant blood and bone marrow phenotypes not normally observed in aged laboratory mice but commonly seen in elderly humans. In vivo HSC self-renewal divisions were absent or extremely rare during both challenge and recovery periods. The progressive, irreversible attrition of HSC function demonstrates that temporally discrete inflammatory events elicit a cumulative inhibitory effect on HSCs. This work positions early/mid-life inflammation as a mediator of lifelong defects in tissue maintenance and regeneration.
This is a quite remarkable paper. Here they show that unlike some hypotheses proposed over the last few years, where they argued your HSC was only impacted during infection or inflammation that the “damage” tallies up even when there is a distance between each infection, from months to even perhaps years, and the damage is cumulative.
With each inflammatory setting, regardless of source, there was no evidence of recovery of functional HSCs therefore a permanent depletion of these cells was present.
While I could now plug a dozen of my other pieces, I won’t for brevity's sake, but here we circle back to the first paper I mentioned, and this one before going deeper and tieing this to other things. If inflammatory challenges especially in mid-life (40+ years) dictate mediates lifelong immune and physiological function, and now besides every other aspect, you are hardcoded to respond with a hyper-inflammatory response to the mRNA, regardless of which mRNA is inside, and all vaccinated have higher ROS than unvaccinated and take longer to recover, isn’t it plausible that merely by the acting of vaccinating you are inducing the very thing the first paper is describing ?
Each time you vaccinate with mRNA, and the Spike Protein you are decreasing your HSCs and aging your entire immune system, then we add the Spike Protein directly damaging HSPCs, and what do you get ? Each time you get vaccinated, you age your entire capacity to renew your cells by a lot, and that is life long change. Inflammation drives the “aging” of HSCs by itself.
Great business model if you are in the pharmacological business, especially when you can tailor monoclonal antibodies to treat basically any ailment under the sun… for a short while.
Among a few other reasons, the paper above was one of the main reasons for my sudden shift into “antioxidants, fast” whenever someone asked me anything, and even when we look from a broader picture, I still stick to this one. Limiting ROS production and inflammation is key to avoiding or limiting the damage from virus/vaccine, in sum the Spike.
Now we circle back. One of the recent, and most present aspects of Inflammaging is one old friend of ours.
To understand what is about to be discussed below you must read this. It is also pertinent for most Long Covid and vaccinated people. (I suspect a sizable portion of the vaccinated have a very skewed kynurenine state).
Tryptophan Metabolism in Inflammaging
Inflammation aims to restore tissue homeostasis after injury or infection. Age-related decline of tissue homeostasis causes a physiological low-grade chronic inflammatory phenotype known as inflammaging that is involved in many age-related diseases. Activation of tryptophan (Trp) metabolism along the kynurenine (Kyn) pathway prevents hyperinflammation and induces long-term immune tolerance. Systemic Trp and Kyn levels change upon aging and in age-related diseases. Moreover, modulation of Trp metabolism can either aggravate or prevent inflammaging-related diseases. In this review, we discuss how age-related Kyn/Trp activation is necessary to control inflammaging and alters the functioning of other metabolic faiths of Trp including Kyn metabolites, microbiota-derived indoles and nicotinamide adenine dinucleotide (NAD+). We explore the potential of the Kyn/Trp ratio as a biomarker of inflammaging and discuss how intervening in Trp metabolism might extend health- and lifespan.
The rate of inflammaging, quantified by measuring these markers, is strongly associated with age-related disability, disease and mortality (6). It is theorized that inflammaging is driven by endogenous ligands released upon age-related tissue damage and can be aggravated by food excess and attenuated by caloric restriction, suggesting relevant cross-talk between metabolic and immune functioning
As I learned from a friend, too much of one thing is bad especially when it comes to our immune system. Kynurenine and its metabolites are the same, under specific circumstances, they will keep you from going into a hyperinflammatory state, on others they will immune suppress you, and cause disease progression because the loss of the ratio of some of its metabolites will definitely skew your immune system.
Per the following highlighted parts.

Furthermore, Tryptophan metabolism is directly linked with the creation (synthesis) of NAD+ from Tryptophan itself, and inflammation/inflammaging skewed towards its metabolism outside the preferential regions, therefore, contributing to local NAD+ deficits, which will impact certain organs more, in this case, the liver, and contribute to metabolic dysfunction.
Dysfunction of the Kynurenine Pathway can not only contribute to this state but can either send you into a hyper-inflammatory state or an immune-suppressed one. And this fluctuation is clearly correlated to everything we discussed so far.
Indoleamine 2,3-dioxygenase 1 (IDO1) is activated in chronic inflammatory states, e.g., in the aging process and age-related diseases. IDO1 enzyme catabolizes L-tryptophan (L-Trp) into kynurenine (KYN) thus stimulating the KYN pathway.
There is substantial evidence that the activation of the IDO1-KYN-AhR pathway robustly increases with the aging process. The activation of IDO1-KYN-AhR signaling does not only suppress the functions of effector immune cells, probably promoting immunosenescence, but it also impairs autophagy, induces cellular senescence, and remodels the extracellular matrix as well as enhancing the development of osteoporosis and vascular diseases.
If you don’t recall, AhR is the “promiscuous” receptor that is used by your body to respond to any foreign substance, in this case, the mRNA and/or LNP, therefore creating and incentivizing the KP feedback loop. There is an extensive paper on the subject of the role of the KP in modulating essential stem cell functions: proliferation and differentiation potential. There is also the role of HSCs in immune memory and immune training, but to avoid going on a massive tangent, I will leave it here, just as an observation for those interested.
As I said, all roads will often lead to Rome and Rome has a bioenergy problem.

In summary, both the vaccine, the Spike Protein, and even the viral infection to a much lower degree deeply affect the “age” and further response to any infection and the capacity of your body to renew its cell, the first two much more drastically than the latter. Accelerating the aging and dysfunction of your entire immune system by low-grade inflammation, creating at least 3 to 4 feedback loops, and they all end somewhat in the same way, with a dysfunctional state of bioenergy.
This is what I refer to as “slowly chipping away” people who keep getting vaccinated and suffer a continuous breakthrough infection of a myriad of pathogens. It is imperative that you take care of your health and inflammatory state, but especially important for anyone vaccinated. I need to write my NAC+Glycine piece, but it will become the cornerstone for the recovery and management of most vaccinated people on the planet, at least the ones looking for a fighting chance.
The topic of inflammation, aging, NAD, and KP is extensive, and I decided to end this here. If there is one single piece you should read after this one, iit s the following.
Because is not directly related to all of this, EFGR plays a very important role in HSCs.
Big appreciation for all supporters and the subscribers who share posts they find useful or interesting.
You know you're on the right track when so many pieces that you've been tracking keep coming together. This one is very important for young people as an incentive to do something sooner rather than later. The potential of kynurenine/tryptophan ratio as a biomarker of inflammaging will be very helpful, but I won't hold my breath for MDs to make it a regular part of their practices. I've long suspected that cholesterol levels might be a potential marker of systemic inflammation. I don't know if that's the case, but my own cholesterol was 240 back in 2012 at age 52. My MD said, "I know what your answer will be, but I have to offer you a statin." I declined. A couple of years later, I started lifting weights and hiking, and in 2016 it was 180, presumably (given my limited knowledge) because my body wasn't producing as much because I wasn't in the same inflammatory state.
Soap box: so was my mid-life health deterioration a degree of irreversible damage? Perhaps. What I do know is that I'm in a MUCH better place now than I was 20 years ago. There's little chance of escaping the fact that sometime in life we're going to have to work hard and deprive ourselves of some pleasures. Make the choice to do it while you're younger by keeping fit and declining the hyper-pleasing garbage that's sold as "food", or your hard work will come in the future when it pains you to do the simplest of things like walking or getting up from sitting positions. The pain you feel from exercise is nothing compared to the pain you'll feel when your body has irreversibly deteriorated. Believe me when I say this. I live in a community of people 55 and older and it's a fucking horror show. Literally all most of them can do is spend their lives sitting on their asses, eating, and watching TV. If you choose to do that when you're young, you'll be forced to do it when you're old. Movement: do it while you can, or someday, you can't because you didn't.
I wrote in the comments section of one of your older posts that a lot of people look a lot older now since the vaxes. I was sure if it was because we don't see people as often due to lockdowns etc or people are looking older. Not all but a considerable majority. Could it be that the repair mechanisms in their skin is also affected? is this somehow regulated with the immune system?