


Covid hyperglycemia as a byproduct of liver infection
Also mRNA myocarditis pathway and positive effects of Metformin

Serendipity strikes once again. And while I try very hard to avoid “bad vibes” on the weekends I will most likely break this self-imposed rule coming the following one because matters are worth it. Regardless it is vindication month from a personal level from a scientific perspective. While the papers covered in this substack are all meaningful I will just get the most significant and pertinent “out of the way”.
One of my main points since late 2020 was the following. SARS-CoV-2 directly impacted the liver and the pancreas, by direct infection of tissues and cells, something heavily criticized for most of the last 3 years. The exact mechanism of how SARS-CoV-2 impacts the liver.
COVID-19-related hyperglycemia is associated with infection of hepatocytes and stimulation of gluconeogenesis
It is no secret that my initial focus, and a significant portion of many of my substacks covering SARS-CoV-2 have been focused on the metabolic aspects of the infection, and even the vaccination, both from a immune response and adverse effects perspective, if you the search function in the website and the words glucose, hyperglycemia you will find many substacks directly related to the subject. The role of poor glucose control on the outcomes of the infection is widely accepted, post-vaccination damage is often less discussed but over time it will be a significant point to bear in mind.
Diabetes constitutes a major risk factor for the development of severe forms of COVID-19 (1, 2).Moreover, several studies indicate that the incidence of hyperglycemia in COVID-19 patients is associated with longer periods of hospitalization and with worse clinical outcome (3, 4).
On the contrary, COVID-19 is also associated with the onset of insulin resistance (8), which potentially contributes to the imbalance in blood glucose control. Since other viral infections caused by RNA viruses such as hepatitis C and B (HCV and HBV, respectively) can induce hepatic glucose production through the stimulation of gluconeogenesis in hepatocytes (9, 10), it is plausible that SARS-CoV-2 could act similarly.
COVID-19 Is an Independent Risk Factor for the Development of Hyperglycemia.
The authors measured the sugar level and took into account the highest blood sugar level each day, and considered any value above 300 mg/dL as severe hyperglycemia, associated here with an increased risk of death in ICU patients, also Covid-19 patients in the hospital exhibited higher incidence of hyperglycemic episodes (spikes of sugar level that come and go) over their hospital stay regardless of their diabetes status.
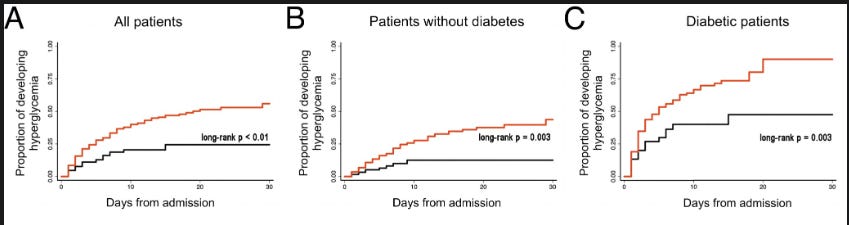
By using Cox regression (a statistical analysis method that takes into consideration many variables that can make something happen, in very simplistic terms) they found that Covid-19 patients had a 2.27 times higher risk of developing hyperglycemia compared to negative patients, and even when considered other factors such as sex, age, diabetes, and corticosteroid use, the associated remained significant. Patients not using corticosteroids had a similar association. One important and remarkable (to me) finding was that BMI did not independently contribute to hyperglycemia.
Next, they decided to measure specific markers to see if the hyperglycemia was due to endocrine pancreas damage, the markers being glucagon, C-peptide, and glycated. Patients with Covid-19 experiencing high blood glucose levels displayed increased levels of C-peptide, glucagon, and glycated proteins levels compared to negative patients, when they were compared with Covid-19 positive patients with normal glycemic levels, they had higher levels of C-peptide and Glycated proteins, but not glucagon indicating they normally secrete insulin.
Detection of SARS-CoV-2 Viral Particles in the Liver.
Next, by examining the liver of 4 nondiabetic patients from their study (postmortem) they found the presence of Spike Protein within approximately 40% of the hepatocytes screened, they also found that the Spike Protein colocalized with double-strand RNA (dsRNA) suggesting the virus can replicate in the liver. They used specific testing using the nonstructural protein 16 (NSP-16) to assure replication in the liver, biopsies from Covid-19 patients were positive for NSP-16. So far this is one of the most important findings in their research since they tested for Spike Protein.
SARS-CoV-2 Infect, Replicate, and Stimulate Gluconeogenesis in Primary Human Hepatocytes.
To understand how mechanistically SARS-CoV-2 does everything analyzed so far, the authors used an ancestral SARS-CoV-2 lineage referred to in the paper as SPBR-02, and conducted the experiments using primary human hepatocytes. The tests (immunofluorescence, amount of viral RNA copies, capacity to generate infective particles) demonstrated that liver cells are susceptible to SARS-CoV-2 infection, and more remarkably the infection did not cause significant damage to those liver cells, found by using common markers (enzymes - lactate dehydrogenase, alanine aminotransferase, and aspartate aminotransferase, with the first being one widely used marker).
After 48 hours post-infection, the liver cells experienced increased glucose production, to almost 2 times the levels of uninfected cells. The genes related to gluconeogenesis (a process of glucose production) or glycogenolysis (breakdown of glycogen to glucose) were not significantly changed or were even reduced upon infection. But what was found increased was the activity and presence of the enzyme PEPCK (phosphoenolpyruvate carboxykinase”, an enzyme responsible for converting certain non-carbohydrate energy sources into glucose (called gluconeogenesis), indicating that SARS-CoV-2 activates (and sequester) PEPCK, therefore manipulating glucose production.
Gamma, Delta, and Omicron were also able to infect liver cells, but Omicron did not produce infective viral particles unline the first two, and in a similar vein as the SPBR-02 variant used, they did not cause significant cell damage.

The last step is finding how SARS-CoV-2 can infect these liver cells since ACE2 has low expression in hepatocytes, there should be another receptor or a “co-factor” a protein that acts as an “in-between” and bridge the gap, and indeed there was the chaperone GRP78 (glucose-regulated protein 78, also known as BiP), chaperones are proteins that are fundamental on assisting the proper folding and assembling of other proteins in the cell. Under cellular stress such as viral infection GRP78 can “move” to the cell membrane and can act as a receptor/entry factor for certain viruses. And here they found GRP78 to be highly expressed in the hepatocytes and colocalized with the Spike Protein of SARS-CoV-2.
Another one of the most remarkable findings of this paper was the fact that blocking both ACE2 and GRP78 didn’t completely stop the entry of the virus into the liver cells, implying a compensatory mechanism, and the probable use of another receptor to do so. As I postulated later last year, SARS-CoV-2 can use a multitude of receptors and has a “preferential” list, and the receptor used defines the fate of the cell.
Why is this paper significant ?
Simply put, now we have an understanding by which mechanism SARS-CoV-2 can infect liver cells, how it impacts the liver, and finally one possible explanation for the higher and decontrolled levels of glucose after SARS-CoV-2 infection. Not only that but since the authors measured Spike Protein, this also implies that Spike can pretty much do the same in specific circumstances.
Another significant point is that hyperglycemia is directly correlated with inflammation, immune dysfunction, and long-term with many chronic diseases, but one of the most important aspects in regards to SARS-CoV-2 is that hyperglycemia is severely correlated to Galectin-3 levels, and also can promote the differentiation and activation of Th17 cells. Hyperglycemia creates an environment that favors the production of IL-17 and the expansion of Th17 cells. Glucose is the preferred fuel of Th17 cells, therefore potentially creating an inflammatory loop as a direct byproduct of skewed metabolism.
Higher levels of GRP78 alone are also significant (cancer, chronic diseases, chronic inflammation, etc).
The findings here are one of the biggest reasons I advised for quite a while the use of Metformin or Berberine, but especially exercise and fasting. In fact, many of the pathologic effects, both short and long-term that I covered recently can often be “fixed” by exactly these two. Fasting, exercise.
Ironically enough, this was just published.
Metformin reduces SARS-CoV-2 in a Phase 3 Randomized Placebo Controlled Clinical Trial
Current antiviral treatment options for SARS-CoV-2 infections are not available globally, cannot be used with many medications, and are limited to virus-specific targets.1-3 Biophysical modeling of SARS-CoV-2 replication predicted that protein translation is an especially attractive target for antiviral therapy.4 Literature review identified metformin, widely known as a treatment for diabetes, as a potential suppressor of protein translation via targeting of the host mTor pathway.5 In vitro, metformin has antiviral activity against RNA viruses including SARS-CoV-2.6,7 In the COVID-OUT phase 3, randomized, placebo-controlled trial of outpatient treatment of COVID-19, metformin had a 42% reduction in ER visits/hospitalizations/death through 14 days; a 58% reduction in hospitalizations/death through 28 days, and a 42% reduction in Long COVID through 10 months.8,9 Here we show viral load analysis of specimens collected in the COVID-OUT trial that the mean SARS-CoV-2 viral load was reduced 3.6-fold with metformin relative to placebo (-0.56 log10 copies/mL; 95%CI, -1.05 to -0.06, p=0.027) while there was no virologic effect for ivermectin or fluvoxamine vs placebo. The metformin effect was consistent across subgroups and with emerging data.10,11 Our results demonstrate, consistent with model predictions, that a safe, widely available,12 well-tolerated, and inexpensive oral medication, metformin, can be repurposed to significantly reduce SARS-CoV-2 viral load.
Additionally, metformin demonstrates a dose-dependent ability to inhibit IL-1, IL-6, and TNF-alpha in the presence of lipopolysaccharide (LPS), inflammatory products that correlate with COVID-19 severity
9 In macrophages of mice without diabetes infected with SARS-CoV-2, metformin inhibited inflammasome activation, IL-1 production, and IL-6 secretion, and also increased the IL-10 anti-inflammatory response to LPS, thereby attenuating LPS-induced lung injury
Metformin directly inhibits or lowers the production of the very proteins responsible for acute and long-term damage of the viral infection, of significance is attenuating the inflammatory response of LPS. Metformin also positively impacts Galectin-3, NETs, Amyloid deposition, and the Kynurenine Pathway. In the substack below you can find what else Metformin can do and a lot of resources and my own “personal stack” meaning what I take daily.

In fact, a running joke between a friend and me was discovering a potential new pathologic pathway from the mRNA or virus, and just searching that pathway and Metformin. Berberine is an almost perfect analog to Metformin. Exercise and a proper diet are superior to both.
Whenever you read a new SARS-CoV-2 post you may do a little game of searching whatever protein or mechanism they are discussing + metformin, and most of the time, be positively surprised.
For last (and also something Metformin would directly ameliorate…)
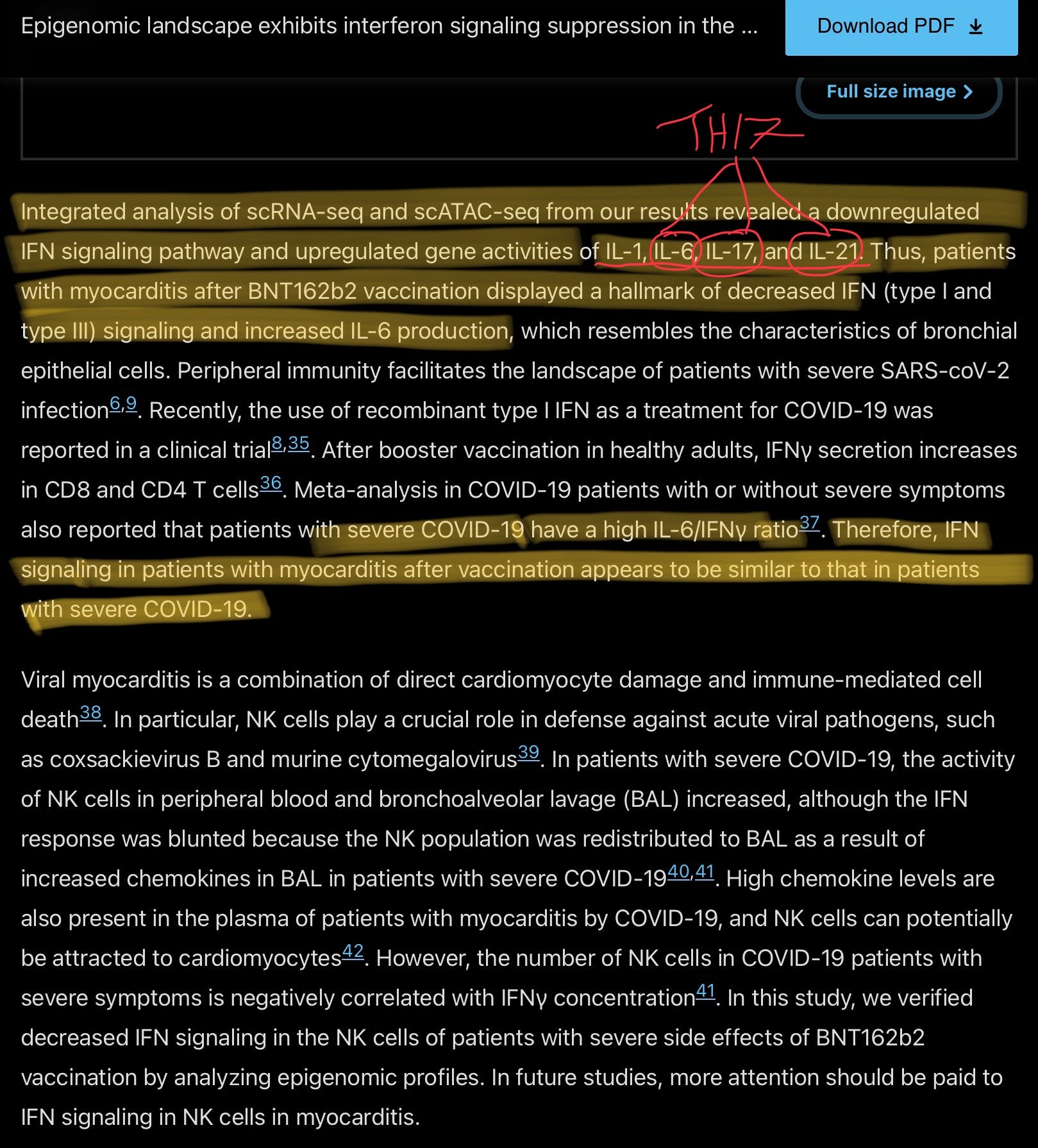
This paper is incredibly significant and impactful on many levels. Since the early roll-out of the vaccines, and me and a friend doing research akin to reverse engineering the mRNA immunological response I stated many times that the immune response elicited was harmful, especially one of the points the vaccine pushers were most happy about, the increased levels of Interferon Gamma (with the literal phrase “It means it is working” stated by one Pfizer scientist).
The screenshot above and highlighted sections are the ones of most importance to me, and a way to keep this substack shorter. Patients that suffer from myocarditis (increasing every day now) have a very similar inflammatory and immune response as patients that suffer from severe Covid-19, the highlighted Interleukins (IL) already say what I wanted to say.
They further raised the point that high chemokine levels are present in cases of myocarditis in patients with Covid 19, severe or not and they might play a role in attracting immune cells to the heart and induce damage. Chemokines are chemoattractants, meaning they attract specific cells by binding in their respective receptors), and the primary function of chemokines is to regulate the movement (migration) of immune cells towards any place with inflammation or tissue damage, they are crucial in the movement of immune cells.
This is an interesting find separated from its role on myocarditis, a paper I am yet to analyze in the context of the duality of autoantibodies found that many people infected with SARS-CoV-2 with mild infection developed temporary autoantibodies against certain chemokines, and this was one of the potential protective mechanism against reinfection months down the road. These autoantibodies waned after months.
A reminder.


If you choose to support this work in whatever form, thank you !
God bless you. Great research.
Wish you were wrong
Have heard so many good things about NAC. Thank you for your research.