
Western excess mortality and depression post-mRNA
And good business intensifies

This is not a Conspiracy “-day”, but in the end, you may as well want to interpret it that way. Breaking through explaining how Neural Networks (the basis of all tech now in a sense) and Machine Learning can be very difficult. In goes a lot of computer science, engineering, and math, out comes “smart machines”. But this video makes one of the best explanations and use cases, so watch it, it will be important later in this article.
First things first, after a while I decided to stop writing about excess deaths because the data was poisoned, completely manipulated, and skewed towards whatever each research group's biases wanted to show, it was early on, a couple more years would give us enough data to make a sense out of the mess. The latest and among the largest studies to date.
Excess mortality across countries in the Western World since the COVID-19 pandemic: ‘Our World in Data’ estimates of January 2020 to December 2022
Introduction Excess mortality during the COVID-19 pandemic has been substantial. Insight into excess death rates in years following WHO’s pandemic declaration is crucial for government leaders and policymakers to evaluate their health crisis policies. This study explores excess mortality in the Western World from 2020 until 2022.
Methods All-cause mortality reports were abstracted for countries using the ‘Our World in Data’ database. Excess mortality is assessed as a deviation between the reported number of deaths in a country during a certain week or month in 2020 until 2022 and the expected number of deaths in a country for that period under normal conditions. For the baseline of expected deaths, Karlinsky and Kobak’s estimate model was used. This model uses historical death data in a country from 2015 until 2019 and accounts for seasonal variation and year-to-year trends in mortality.
Results The total number of excess deaths in 47 countries of the Western World was 3 098 456 from 1 January 2020 until 31 December 2022. Excess mortality was documented in 41 countries (87%) in 2020, 42 countries (89%) in 2021 and 43 countries (91%) in 2022. In 2020, the year of the COVID-19 pandemic onset and implementation of containment measures, records present 1 033 122 excess deaths (P-score 11.4%). In 2021, the year in which both containment measures and COVID-19 vaccines were used to address virus spread and infection, the highest number of excess deaths was reported: 1 256 942 excess deaths (P-score 13.8%). In 2022, when most containment measures were lifted and COVID-19 vaccines were continued, preliminary data present 808 392 excess deaths (P-score 8.8%).
Conclusions Excess mortality has remained high in the Western World for three consecutive years, despite the implementation of containment measures and COVID-19 vaccines. This raises serious concerns. Government leaders and policymakers need to thoroughly investigate underlying causes of persistent excess mortality.
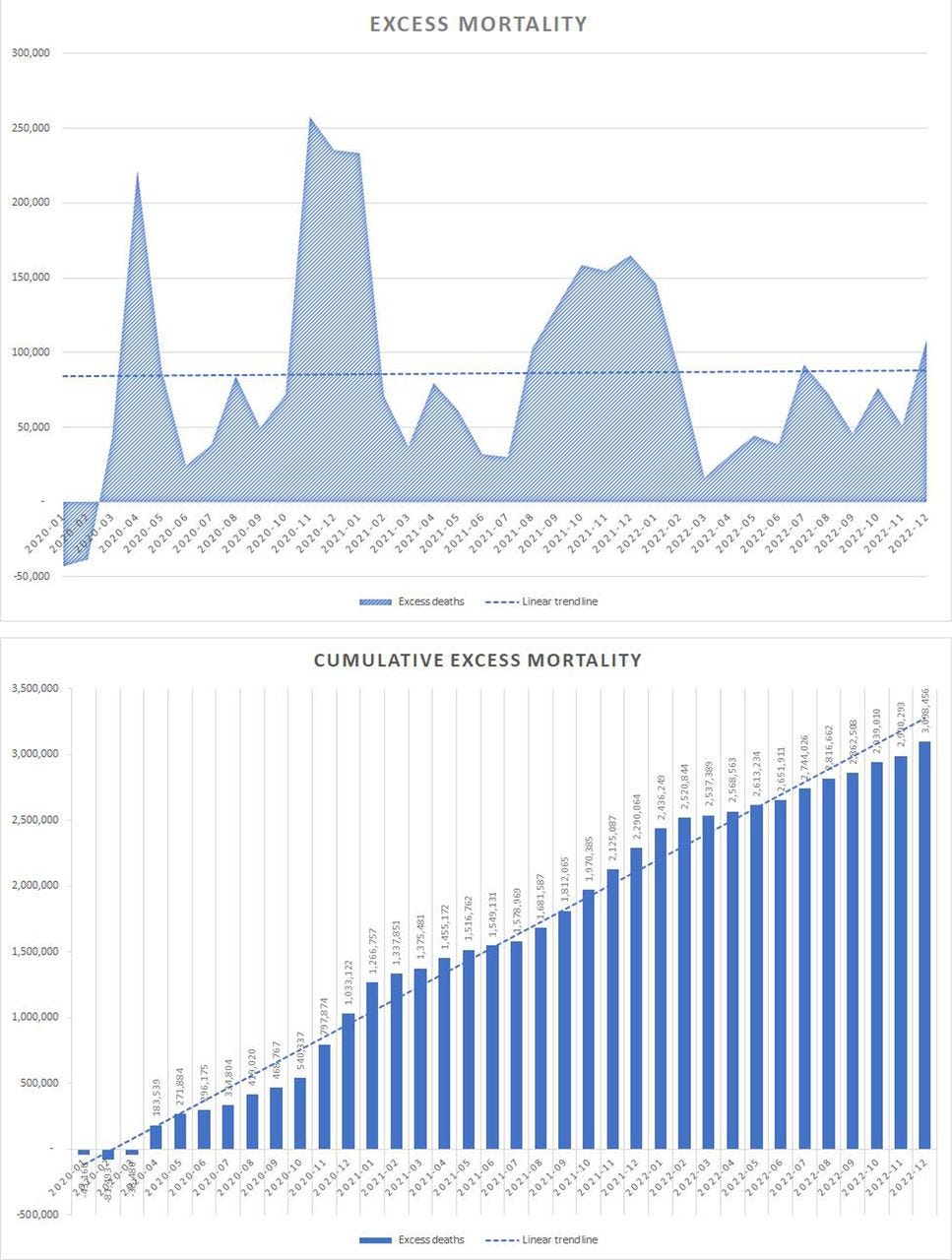
Simple to understand.
2020 experienced excess deaths in Western Countries, there were no vaccines
2021, introduction of vaccines, Western Countries experience excess deaths
2022 provisional data, vaccines still heavily used, Omicron dominates, still excess deaths
The authors are very honest and paint a truthful picture of the limitations of researching excess death, and even the math involved (you can fudge the math quite easily), but the main problem here is transparency from the pharmaceutical companies, from governments, the amount of resources that needs to be put so the data reflects reality. Governments are not willing to incur the political cost of assuming this once-in-a-century fuck-up.
I also want to bring to your attention the atrocious lag time from the moment the journal accepted the paper.
Received: 9 June 2023
Accepted: 20 March 2024
First Published: 3 June 2024
Was this a conscious choice of the journal and/or editors ? A massive lag, and deciding to publish it right when there is a significant and observable narrative shift ? But excess mortality is somewhat of a “low-hanging fruit” my primary interest was always the long-term consequences leading to massive geopolitical shifts.
Who would have thought vaccinating using a neo-polymorphic toxin from a chimeric virus would have similar, yet faster consequences ?
Thus the next two studies bear more weight here. Here is an early dark tweet on the subject.

Psychiatric adverse events following COVID-19 vaccination: a population-based cohort study in Seoul, South Korea
This is a population-based study, meaning it covers millions of individuals in a specific country. In this particular case, there were 2.027.353 participants. The findings are as it follows:
The cumulative incidence of depression, anxiety, dissociative, stress-related, and somatoform disorders, sleep disorders, and sexual disorders at three months following COVID-19 vaccination were higher in the vaccination group than no vaccination group. However, schizophrenia and bipolar disorders showed lower cumulative incidence in the vaccination group than in the non-vaccinated group.
Unlike other papers covering a similar subject, the authors propose multiple potential mechanisms on how Covid vaccination could increase the incidence of depression, anxiety, dissociative, stress, sleep, and sexual disorders 3 months after vaccination, although schizophrenia and bipolar disorders went down in the vaccinated group.
The first proposal is the alternation of the hypothalamic-pituitary-adrenal (HPA) axis, in simple terms the HPA axis is the link between the endocrine and the nervous system, a way to link hormones from the gut to your brain, thus affecting here mainly serotonin.
The second proposal is the absurd amount of inflammatory response mounted by the vaccines, specifically the author’s name the LNP part of the mRNA vaccines. Complementary to this the following argument is one we are familiar with, free Spike Protein floating around, reaching the brain and engaging specific receptors, particularly TLR2 and TLR4, both with extensive evidence of harm caused by the viral spike alone.
The last step was testing which genes were enriched, seeing which genes were more abundant for each “disease”. And the peculiar finding.
For depression, as an increased risk after COVID-19 vaccination, the results were shown for the deep interaction of spike protein-related factors such as NLRP3 inflammasome [40]. This supports that the presence of the spike protein plays a crucial role in the manifestation of diseases after COVID-19 vaccination
NLPR3 is an old friend of ours. Below some of the articles that mention or directly refer to it.
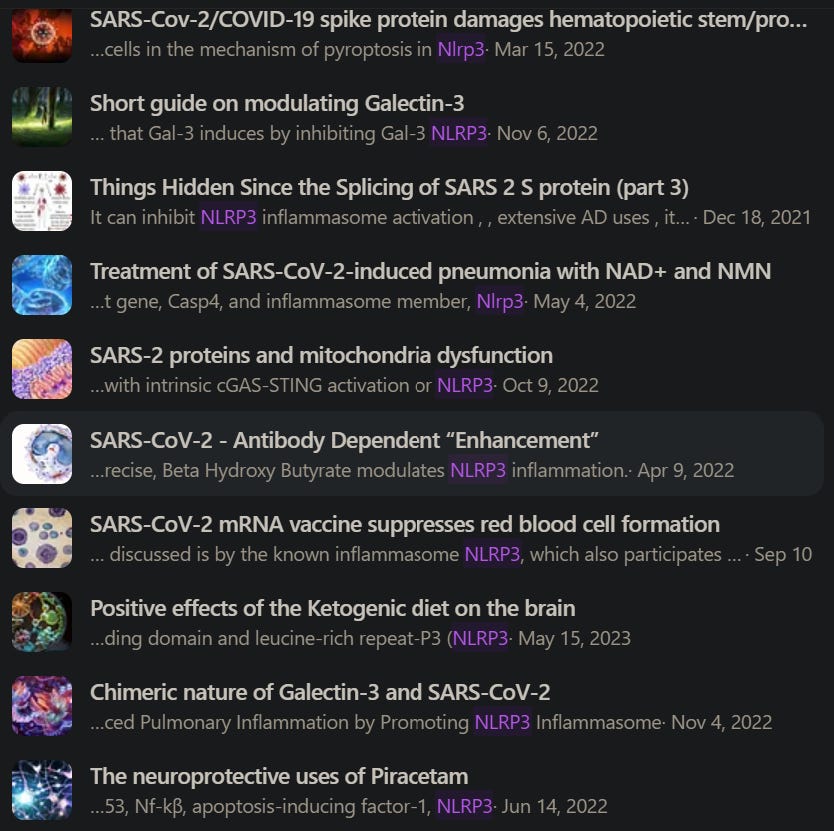
Of course, the body and our cells are not a closed system, so shall we do what we usually do ? TLR4 primes and also activates NLRP3. Endotoxin, which directly binds to TLR4, can cause more coagulation in conjunction with NLRP3. Endotoxin also directly makes the body shift into the Kynurenine Pathway. Paradoxically enough, one metabolite from the Kynurenine Pathway, Kynurenic acid ameliorates the inflammatory damage of NLRP3, so sometimes the body may shift, for a period of time towards the Kynurenine Pathway not solely because it needs more “cell energy” but for protective, dual-edge reasons.
Since HMGB1 should be fresh in your mind, care to guess ? HMGB1-activatied NLRP3 inflammasome induces thrombocytopenia. LPS can make macrophages “expel” extracellular vesicles (small cells from big cells) carrying HMGB1 which causes more damage. The cooperation of both NLRP3 and HMGB1 is what can enable latent viruses to wake up. All of this and more contributes to both changes in systemic metabolism, dysbiosis (changes in your entire microbiome), thus creating multiple feedback loops that make Long Covid symptoms and others persist.

And all of this contributes to… depression. The problem with pinning down “vaccine injury mechanisms” is precisely because it is basically the same as the viral Spike Protein, but worse. And the problem with both depression and all the mechanisms above is their duration. Depression and its causative mechanism are all long-lasting, they can last months or years, and depression is the primary perfect example of a “negative feedback/doom loop”.
Recently a new “potential” treatment for vaccine injury was proposed. I will leave the boring detail out, but basically it uses LNPs to deliver small-interfering RNA to targeted cells, which is somewhat a lie, because it is impossible to precisely target anything with LNPs. Here the authors propose the usage of LNPs for gene editing and gene silencing.
However, there are still some challenges for utilizing nucleic acid therapeutics in vivo because of certain unfavorable characteristics, such as instability, biological carrier-dependent cellular uptake, short pharmacokinetic profiles in vivo (RNA), and “on-target” and “off-target” side effects (DNA).
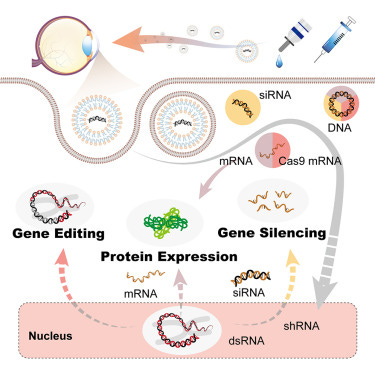
One of the most common problems in using siRNA is its off-target effect, you aim at stopping gene X, but you will often hit genes around the region or with similarities. siRNA can interact with dsRNA and also trigger non-specific off-target effects… and this got me thinking (and this is where Neural Networks video and Machine Learning come in).
From a biological-organic cognitive perspective, Machine Learning/AI and current Neural Networks are horrible learners from an efficiency perspective. They do learn, and they can infer a lot from that knowledge, and find patterns most humans and experts miss, but the problem is scale. We need far less data to learn. GPT4 for example was basically trained upon the entire knowledge mankind ever produced in thousands of years, yet it is not “super-intelligent” in a general sense.
This means current AI/Machine Learning needs a lot of data. Lots, and lots of data. This has been my argument for years, the mRNA experiment was the largest data-gathering experiment in human history, and even Pfizer and Moderna were proud to announce this. You introduce a therapeutic that induces gene mutation, but that is not enough data… so, years down the road, you introduce the cure, a therapeutic that introduces gene silencing. You gather the data.
Advance molecular genetics and biology 50 years within 10 years.
The modern adage I introduced in 2021 persists.
Just as a way to balance things and be positive, a first, scientists used gene therapy to significantly improve hereditary deafness in 5 of 6 children.
The authors concluded, “Our results show that AAV1-hOTOF binaural gene therapy for patients with DFNB9 is feasible, safe, and efficacious. The study expands the scope of DFNB9 treatment, potentially improving clinical intervention for hereditary deafness and promoting clinical transformation of gene therapy for hereditary deafness caused by other deafness genes.”

Added Chen, “Our study strongly supports treating children with DFNB9 in both ears, and our hope is this trial can expand and this approach can also be looked at for deafness caused by other genes or nongenetic causes. Our ultimate goal is to help people regain hearing no matter how their hearing loss was caused.”
I appreciate your support ! Thank you !
Yes, it is all about the data. Data is the new gold and data is everything (right now). Cynic worldview but correct for the next 10 years or so.
Phew! - Thank you. I expect these bioweapons have been under development for a decade or more.
The horrendous effects are by design it would appear, so many vectors - LNP, Q Dots, nano tech,
Graphene O&Hydrox', the emf's /5G... Gene editing @ 'cyborgous homo not geniuses'.... GMO Human.2 'owned' beings... sad, really sad.