
Type 1 diabetes "epidemic" in children during the pandemic
Happy 4th of July !

First and foremost a Happy 4th of July to all my American subscribers. Most likely one of the most important holidays in human history. The Founding Father’s writing is among the very few “political” writing I often suggest anyone read.
I hope everyone had or is celebrating a very nice day.

At this point it is no secret one of my biggest interests in regard to SARS-CoV-2 is its effects on human and cellular metabolism, both implicated in almost all of its damage, both acute, severe, short, and long-term. I will not bother you linking past substack, but recent ones will bear more weight here than older ones. This will be also simplified. Earlier today I was surprised on finding the following paper.

Results Forty-two studies including 102 984 incident diabetes cases were included in the systematic review. The meta-analysis of type 1 diabetes incidence rates included 17 studies of 38 149 youths and showed a higher incidence rate during the first year of the pandemic compared with the prepandemic period (incidence rate ratio [IRR], 1.14; 95% CI, 1.08-1.21). There was an increased incidence of diabetes during months 13 to 24 of the pandemic compared with the prepandemic period (IRR, 1.27; 95% CI, 1.18-1.37). Ten studies (23.8%) reported incident type 2 diabetes cases in both periods. These studies did not report incidence rates, so results were not pooled. Fifteen studies (35.7%) reported DKA incidence and found a higher rate during the pandemic compared with before the pandemic (IRR, 1.26; 95% CI, 1.17-1.36).
Conclusions and Relevance This study found that incidence rates of type 1 diabetes and DKA at diabetes onset in children and adolescents were higher after the start of the COVID-19 pandemic than before the pandemic. Increased resources and support may be needed for the growing number of children and adolescents with diabetes. Future studies are needed to assess whether this trend persists and may help elucidate possible underlying mechanisms to explain temporal changes.
The reason for me to write this substack today “out of the blue” while I was working on the Nova Swan one was the author’s conclusions, arguing low-key there are no know mechanisms for Type 1 or even 2 Diabetes. A refresher, Type 1 is of autoimmune nature, Type 2 is basically a metabolic state and continuous poor response to insulin. As a matter of track record, since early September 2021 there were dozens, subsequentially hundreds of “safety signals” in regards to glycemic control and the low-hanging fruit of 2023, the mRNA vaccine, including Type 1 Diabetes. There are a few case reports of Fulminant Type 1 Diabetes after vaccination. The infection can rarely induce the same, here a Chinese pregnant lady developing it. The inactivated vaccine may also induce but at such a lower rate that is indeed very rare.
The difference here is the amount of Spike Protein your body is “flooded” with. I am not fond of repeating myself, but certain criticism I will, as how the mental rigidity certain fields of medicine and science indulge upon makes them unable to forecast basically any meaningful event because they always act in a retroactive way. This cognitive trend ain’t helping anyone in the next 2 decades.
With my tangent and the low-hanging fruit (direct link to vaccines) out of the way, my primary criticism of the authors of the T1D paper. First the most obvious potential mechanism.
Given the properties of SARS-CoV-2 and its Spike to both displace and use Endotoxin, especially from intestinal/gut original, there is evidence for intestinal endotoxin as a trigger for Type 1 Diabetes, even before the onset of any common microvascular complication (a somewhat early sign of T1D), there is evidence for sustained endotoxin activity. The role of Endotoxins in development (triggering is the scientific term used) is quite extensive and undeniable, what is left to discover is the exact mechanism.
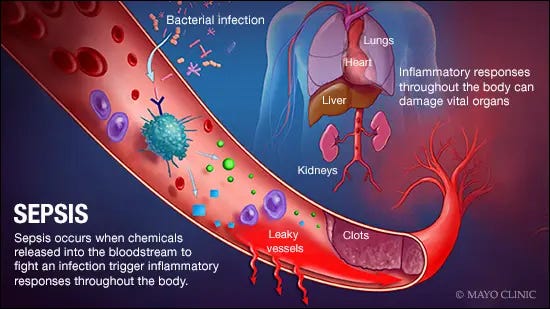
Untreated Type 1 diabetes increases sepsis mortality without inducing a lethal cytokine response, which I personally refer to sometimes as “covert sepsis”. We have the start of one doom loop.
Galectin-3 (which has an almost perfect mimic stitched in the Spike N-Terminal Domain) has been shown to be involved in both types of Diabetes, it directly induces inflammation in the region, and as you should be aware by now, it binds and interacts to Endotoxins. This is what they call a twofer ?
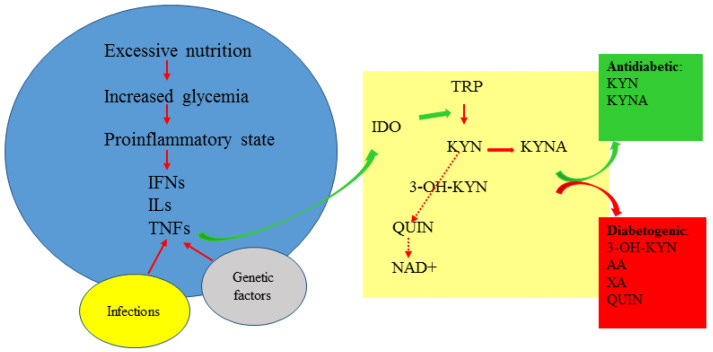
I will not bother mentioning Interleukin-12, since I literally did merely a few days ago, and the list of evidence on this one is rather large. The other part of the axis, Interferon-Gamma also has a role in the pathogenesis of T1. IL-12/IFN-Gamma axis will induce the expression of IDO, the enzyme responsible for the breakdown of Tryptophan into Kynurenine. And repeating myself (ugh) Kynurenine Pathway is the quintessential example of a biological double-edged sword.
So far, this covers many of the pathways I have written, quite extensively at that, about recently. Everything discussed so far can work “together”, creating negative feedback loops where one increases the other ending up in synergy to induce disease. One last variable to add to this protein-focused part of the substack is Nicotinic receptors. Specifically, a7 nAChR and the loss of this specific receptor influence the development (and overall the whole metabolic, inflammatory process) of Type 2 Diabetes.
But not just protein floating around does Type 1 Diabetes happen, in fact, one of the few consensus in regards to T1D among researchers is the role of viruses in the development of the pathology. I did say latent viruses play a massive role in regards to all the damage SARS-CoV-2 induces, and I do want to remind you to check the list of pathogens Endotin exposure and sepsis awakens inside someone.
HHV-6 (one of the pathogens responsible for Long Covid) has been linked as a contributor to T1D. Drug Hypersensitivity Syndrome can be a life-threatening condition, in rare cases leading to Fulminant T1D, and HHV-6 has been implicated as having a role.
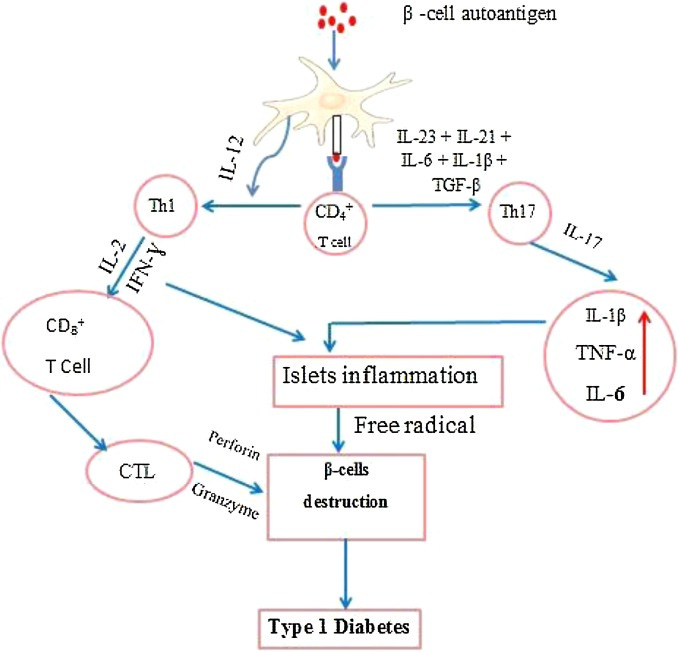
A similar role for Epstein-Barr Virus (EBV), DHS, and T1D has been proposed. EBV has also been proposed in recent years as being involved in the development of T1D, and lo and behold, in this very recent paper the authors found that children with EBV had lower levels of CD8, and they had a higher secretion of IL-17. IL-17 (and therefore Th17) both have a role in Type 1 and 2 Diabetes (a reminder this is the dominant immune response of severe infection and the vaccines). EBV is directly linked to Long Covid too.
As of no surprise, if you read my criticism of using mRNA to vaccinate against Influenza viruses (in there, I went through a paper that demonstrated higher sustained levels of influenza antibodies are directly linked to developing autoantibodies, therefore autoimmune disease), Japanese researchers found that there is a risk of developing new-onset Type 1 Diabetes after influenza infection.
Another can of worms that I rather deal with on a substack solely on the subject is Ferroptosis, the cell death caused by Iron dysfunction, now with good evidence on its role in the pathology of T1D. For months after the first wave of vaccination, anyone using social media was able to find poor iron control of all sorts.
For visual learners and further research. Yeah, “no mechanism” for T1D and SARS-CoV-2 (or even the mRNA) indeed.

Given the role of latent infections and many proteins related to them, to endotoxin and the Spike Protein, addressing the same pathways ends up mitigating the chances of developing T1D. Such as Vitamin D being protective in children diagnosed with early T1D. People with T1 and T2 both have a higher need for Vitamin C. The same goes for younger people needing a higher dosage of antioxidants such as NAC.
In rats, NAC reduces the morbidity rates of T1D. Basically, sometimes the same, sometimes different pathways, but the supplements I suggest tackle what was discussed here.
If you chose to support my work, thank you =) !
The viral trigger for type 1 diabetes goes back in literature quite always. Many years ago Denmark had a mumps epidemic and in the 2 years after the mumps epidemic diabetes rates skyrocketed. Type 1 diabetes is also a listed adverse event of the mmr vaccine, undoubtedly since it’s a live virus vaccine introducing the mumps virus into the body even if attenuated.
Celiac disease also has a high prevalence in t1D and undiagnosed celiac can seem to make those genetically susceptible more likely to develop t1D.
All in all, it’s sloppy research to not mention any previously discussed mechanisms of cause for t1D. The increase in DKA is no mystery - it can happen so quickly and early stages it looks like a gastro virus. With all the “stay home” messaging, kids who may have otherwise been diagnosed at the frequent urination stage were likely missed and so were in full DKA by the time they sought medical help.
This is first time I’ve heard of EBV as a trigger, but I’ve long believed that any virus can trigger it, some are just more likely to than others. Also auto-antibodies can take years to damage the pancreas to the point where it no longer creates insulin, so the timing is actually less specific than is being let on. There is testing that can be done to show if or how many auto antibodies someone has. (Have to have a first degree relative with t1D to participate.) If someone is negative for all they can become positive at any time but those who are positive don’t turn negative again. Onset of insulin dependence after the antibodies are present can vary from weeks to years though so there is still a lot that needs to be learned.
Had a bad flu almost 30 years ago on New Years Eve, 3 months later I was diagnosed Type 1. I have other autoimmune issues now as well.