
The shift in mRNA elicited immunity
IgGs don't go brrrrr.

I was supposed to publish the next BMO today, but life get in the way, and I barely wrote 30% of what I intended to, and in the spur of the moment, I decided to write this one instead. A paper recently caught my attention, I even got referred to it a few times, but before we delve into said paper, we need to understand many others, because this actually creates an immunological shifting timeline in regards to mRNA vaccination.
For context before reading the rest of this piece, for many months hidden in between the lines of many papers, and subject to a wider context, you would basically need to read papers outside their disciplines, there was a clear shift in the immunologic response of the vaccines. The “hybrid immunity” was born from this shift, where many papers were trying to elucidate and obviously “push” the safety and effectiveness of these genetic products.

That 5-month-old post is quite important because it demonstrates to us many important aspects of SARS-CoV-2 infection, and while there is no mention of vaccination, it will be important later. What it demonstrates is that Fc Receptors mediated both the infection and death of certain cells, non-neutralizing antibodies mediated this inflammatory process, among other interesting points. To summarize, SARS-CoV-2 can use all 3 Fc gamma Receptors to infect certain cells, and create a potent inflammatory reaction and most of these cells will die. The body tries very hard to kill any cell SARS-CoV-2 infects, probably a reaction to avoid any possible reservoir creation.
In fact, if the body somehow creates a high affinity towards FC gamma IIIa, the immune system may respond aggressively to infection and uses ADCC (antibody-dependent cellular cytotoxicity) leveraging the response toward disease severity. The following article titled The role of IgG Fc receptors in antibody-dependent enhancement is an amazing paper that anyone interested in all of this should read. Here are some highlights.
Administration of neutralizing antibodies at sub-neutralizing doses113 or non-neutralizing mAbs capable of engaging and activating FcγR pathways was not associated with enhanced disease pathogenesis or IgG-mediated tissue inflammation73,77,79,82,112,114–117

While the authors of this paper argue the opposite of what most would assume, I will argue they were partially right for the wrong reasons. So here we go into something that has been “popping” up in different papers lately.
Hybrid immunity shifts the Fc-effector quality of SARS-CoV-2 mRNA vaccine-induced immunity
The paper only uses previously infected and never-infected (naive), both vaccinated. This paper tries very hard to paint the picture one would expect, but alas there are a few data points worth covering, which I will so we finally get into what I mentioned at the start of this.

In line with previous evidence, there is a shift of both Immunoglobulins (antibodies) of the G type (a class of antibodies) and there is a distinct shift between previous infected and never infected. Among the naive there is a clear correlation between IgG3 and FcR binding, which in this case means neutrophils were opsonizing (covering something in antibodies) and phagocyting it (eating and digesting a pathogen).
The second paragraph, which is in regards to the second dose of vaccine in both groups is even more revealing, where previously infected individuals have a closer to what one would conclude “normal” IgG response, away from IgG3 and FcR binding, suggesting a shift in the Neutrophil Pathocytosis mechanism.
Incidentally, this shift in previously infected individuals is towards IgG1 with strong coordination of antibodies features, and in this case, Monocytes are the ones doing the phagocytosis. There are clear differences in antibody responses and classes and use of receptors between both groups.

This is the discussion part of the paper, where they state and by the evidence, it is clear, that there is both a shift and enhanced binding in “hybrid immune” people particularly skewed towards two specific Fc receptors. Now refer to the first piece of mine about Fc-mediated infection of monocytes, and setting off inflammation.
So far, given the nature of the antibodies from the vaccines becoming non-neutralizing astounding fast, with the body wanting to clear the “virus” (in truth, mostly the Spike) as fast as possible, with the increasing danger of lowering your white blood cells because the virus is infecting them, and your body aborting (killing) these cells, setting off small inflammatory bombs inside you.
Now we go to the main paper I wanted to cover for a while. What would the body do in the fact of continuous antibody-mediated inflammation ?
Class switch towards non-inflammatory IgG isotypes after repeated SARS-CoV-2 mRNA vaccination
Shortly after the first or second mRNA vaccine dose, the IgG response mainly consists of the pro-inflammatory isotypes IgG1 and IgG3 and is driven by T helper (Th) 1 cells. Here, we report that several months after the second vaccination, SARS-CoV-2-specific antibodies were increasingly composed of non-inflammatory IgG2 and particularly IgG4, which were further boosted by a third mRNA vaccination and/or SARS-CoV-2 variant breakthrough infections. While IgG antibodies were affinity matured and of high neutralization capacity, the switch in constant domains caused changes in fragment crystallizable (Fc)-receptor mediated effector functions, including a decreased capacity to facilitate phagocytosis.
IgG4 induction was neither induced by Th2 cells nor observed after homologous or heterologous SARS-CoV-2 vaccination with adenoviral vectors. In addition, IgG2- and IgG4-producing memory B cells were phenotypically indistinguishable from IgG1- or IgG3-producing cells. Since Fc-mediated effector functions are critical for antiviral immunity, the described class switch towards non-inflammatory IgG isotypes, which otherwise rarely occurs after vaccination or viral infection, may have consequences for the choice and timing of vaccination regimens using mRNA vaccines.
The first two paragraphs are rather easy to understand, and unlike some other papers, you need to go through the usual… rhetorical maneuvers from the writers this is bound by evidence. Since the vaccination efforts are rather young at this point, now more evidence arises from the rather profound changes the immune system is going through.
Here the authors report a change in IgG responses after many months following the second dose of the vaccines, with this change being a particularly strong anti-inflammatory response, and of major interest IgG4. These continuous changes are affecting the capacity of the body to phagocytize pathogens.

The timing of the measurement of all different types of IgG mattered, ten days after two doses of the vaccines the IgG 1, 2, and 3 were readily detectable in line with previous evidence and the paper above, with IgG4 completely undetectable. After a booster, the levels of IgG1 were elevated again and reached the same levels as the second dose but there was an increase in IgG4 in almost all vaccinated. And in some of these individuals, IgG4 became the second most abundant IgG, behind only IgG1, IgG2 also increased, while IgG3 increase was marginal. So either disproving the paper we just covered or… there is an immunological shift going on in regards to the mRNA vaccination.
They go further to test if mixing vaccines would cause a similar shift in IgG levels in which they found that IgG4 was detectable in half of the mRNA-mRNA group, but only in 1 of 51 of the other two vaccine groups.

This is compatible with the view that the mRNA vaccine response is still less diversified and/or affinity matured than the majority of all other memory B cells acquired over the lifespan of adults. Analysis of the limited numbers of available spikebinding memory B cells did not reveal significantly higher frequencies of somatic mutations in clones that use distal isotype sequences.
They go further to test if this was the case with other types of vaccines or the byproduct of repeated vaccination using tetanus toxoid, and Respiratory Syncytial Virus infection, finding that the switch to IgG4 is not a consequence of repeated antigen exposure from vaccination or infection.

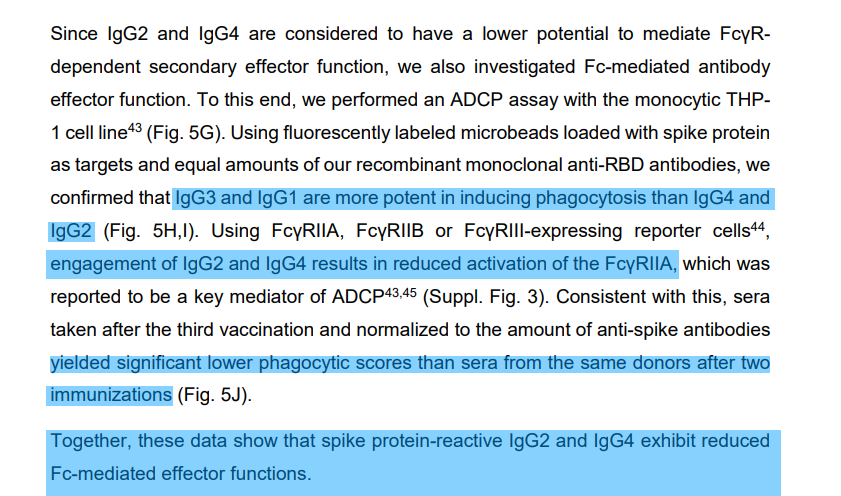
The presence of IgG4 correlated with the quality of the antibodies, but with poorer effector function. In line with the evidence discussed here both IgG3 and 1 had a more potent effect on inducing phagocytosis than IgG4 and IgG2 which are “weaker” antibodies in regards to this function. The discussion part of the paper will explain why this matters.

The timing of the breakthrough infection directly correlated with the IgG4 levels even more so than vaccination, which the more powerful (anamnestic) responses being 3 months later than the last vaccination, in which besides other many good points, they argue that there is a pool of memory B cells slowly forming, fixated on IgG4, meaning that the immune system will often fall into this immune response than the other more capable of phagocytosis, and this is not a feature of Spike exposure and most likely from the mRNA itself.
Antigen-specific IgG4 antibody responses are generally thought to develop in response to Th2-mediated B cell activation or as a consequence of chronic antigen exposure. Parasite infections or allergic antigens are known for their potential to drive CD4+Th2 cells producing cytokines such like IL-4, IL-5 or IL-13, whereas most viral infections promote Th1-biased cellular responses. Initial reports on the cellular response to the mRNA vaccine candidate BNT162b1 indicated a Th1 profile in the phase I/II clinical trial and also other reports did not identify Th2-biased immune response
Indeed, stimulating PBMCs from vaccinees showing high or low IgG4 levels with spike T cell epitopes did not reveal significant differences in the frequency of S-specific Th cells and rather suggested a Th1-biased CD4 response, based on the observed frequencies of IFNγ- and IL-4 producing cells. In contrast, a robust and persistent T follicular helper cell response for up to six month after mRNA vaccination has been characterized in draining lymph nodes by fine needle aspiration biopsis, which is in line with a long ongoing GC reaction. The underlying reason for this observation still requires clarification, but a prolonged presence of vaccine mRNA or antigen in the lymph node might be a potential explanation
However, the vast number of breakthrough infections caused by the omicron variant indicate that the current vaccination does not confer sterile protection. Once infection is established, Fc mediated effector functions become more relevant to clear viral infections
In this regard, IgG4 is considered as an anti-inflammatory IgG with low potential to mediate Fc-dependent effector function such as ADCC or ADCP.
For the control of viral infections not much is known regarding virus-specific IgG4 antibody responses. As shown here for RSV-specific IgG responses, IgG4 is hardly induced by acute respiratory viral infections even after repeated exposure. With the exception of measles-specific IgG4 antibodies induced by natural infection, even chronic viral infections like HCMV do not trigger significant specific IgG4 antibodies
Our findings on an unusual, mRNA vaccine-induced antiviral IgG4 antibody response appearing late after secondary immunization clearly require additional investigation. Apart from further clarification of the precise underlying immunological mechanisms driving this response, it has to be evaluated how an IgG4-driven antibody response affects subsequent viral infections and booster vaccinations. This is not only relevant for potential future vaccine campaigns against SARS-CoV-2, but also for new mRNA-based vaccine developments against other pathogens.
In the first paragraph, the authors argue something I did months ago, but now with more depth, IgG4 responses especially long-lasting are often related to Th2, allergic responses, and less on viral infections, especially from a respiratory type, and so far the published evidence goes the mRNA response is heavily skewed towards Th1 responses.
Among the possible reason for this shift in response is the continued presence and exposure of mRNA and/or antigens in Germinal Centers, which I said was incredibly bad by the simple fact that the Spike has too many antigens AND proteins mimicking our own all over itself. So one way the body would deal with this persistent inflammatory response would be shifting the overall immune response towards a less inflammatory one, which is a rock and a hard place. This response will lead the proteins to not be cleared properly, which in turn will lead to the continuous production of a less effective response.
As summary (gross simplification), in line with everything discussed so far in this piece, it is clear the immune system is shifting towards a less inflammatory antibody response (IgG4) to protect itself from both immune exhaustion, excessive inflammatory responses, and to preserve the function of various white blood cells, to avoid what at the very start of this year was a clear sign of initial levels of ADE. Also, an IgG4 response is often correlated to immune tolerance.
In line with what I usually do, I will leave you with this. There is a remarkably new class of disease, recently discovered.

I will end this will a few points, that I may leave answered, or may not.
There is a functional synthetic sequence added to the virus that directly acts in an immunologic activity with IgG4, which can lead to disease
Argued among many immunology researchers is why certain treatments aimed at B-Cells conditions are so effective, mainly treatments to Anti-CD-20 and Anti CD-19
In the Pfizer Spike sequence, they added a specific antigen. A CD-20 antigen. Functionally speaking it is an Anti-CD-20 embedded function. Why would they do it ?
Abnormal expression of CD20 on IgG4 plasma cells associated with IgG4-related lymphadenopathy
The anti-CD20 antibody rituximab reduces the Th17 cell response
You can make your own assumptions after this, there is enough here for you to go through. BMO or a shorter post coming tomorrow.
Massive appreciation to all supporters here and on Kofi !!!
"synthetic sequence added to the virus" by any red-pilled explanation would mean a chimeric bio-weapon released on all of humanity.
Covid did to me what no other pathogen did before [and I've had some pretty nasty flu bugs], and that's wiping out my sense of smell. It took me a good 7 full months to regain my sense of smell and I'm a hard core essential oil huffer and a foodie/baker and it was actually frightening to lose.
I'm a bit of a Pollyanna in that I try to find something good out of something awful. For me, it was regaining my sense of smell and appreciating it even when I smell something off-putting. It's a daily reminder of how blessed we are when we have our health in tact.
I hope and pray for humanity to survive this evil. Sadly, it doesn't look good for those who fell for the hot lot shots that completely cripple the immune system to the point where it literally turns on itself. Every effin' 'booster' is a potential suicide bullet. 😭💔
Wow, looks like you were well ahead of the curve on this one!