

You can use this link to see the search results of kynurenine in my Substack. for further context here is a summary from memory.
Many SARS-CoV-2 patients have a skewed Tryptophan catabolism, being rich in kynurenine
The kynurenine pathway is directly connected with many inflammatory, neurodegenerative, nervous system diseases
Endotoxin exposure can shift the body into the KP, endotoxic tolerance is contingent on it
I proposed this would affect how latent pathogens behaved and had implications towards Long Covid, and Spike Protein mediated damage
Later proposed the same pathway would be responsible for much more, and failed to mount proper clearance of virus/fragments
As I wrote in a few of my recent pieces, I would write about the importance of (proper) Tryptophan metabolism. What led me to this was a sudden lightbulb moment, as it often occurs in my weirdly wired brain, the thought is as follows.
All cells, especially T-Cells have a preferred metabolism, a faster way to create energy, some prefer lipids (fats), other glycolysis (sugar), but… what about Tryotphan, which is closely related to “cell energy” itself ?”
These questions were impulsed by the findings in the substack below.

In a portion of Long Covid, and I personally expect in a portion of the people damaged by the plagued combination of mRNA + multi-breakthrough infections there is a failure of the body to properly respond to the Nucleocapsid protein, especially the Memory cells (memory cells are able to respond really fast and aggressively to subsequent infections, like an already deployed battalion with proper intelligence/information), they also can function independently of secondary lymph organs, which other T Cells often can’t. Effectively they are somewhat the “fast responders” when you find the same pathogen or closely similar at a later time.
Keep in mind recent discussions about how this happens in regards to Covid, basically by engaging the Aryl Hydrocarbon Receptor, secondly by the Interferon-Gamma/IL-12 axis, present in infection, acute or prolonged, and over-represented in latent/chronic infections. There are many ways for the body to engage in a metabolic trap that drains tryptophan while producing too much of the Kynurenines or enzymes needed to produce them.
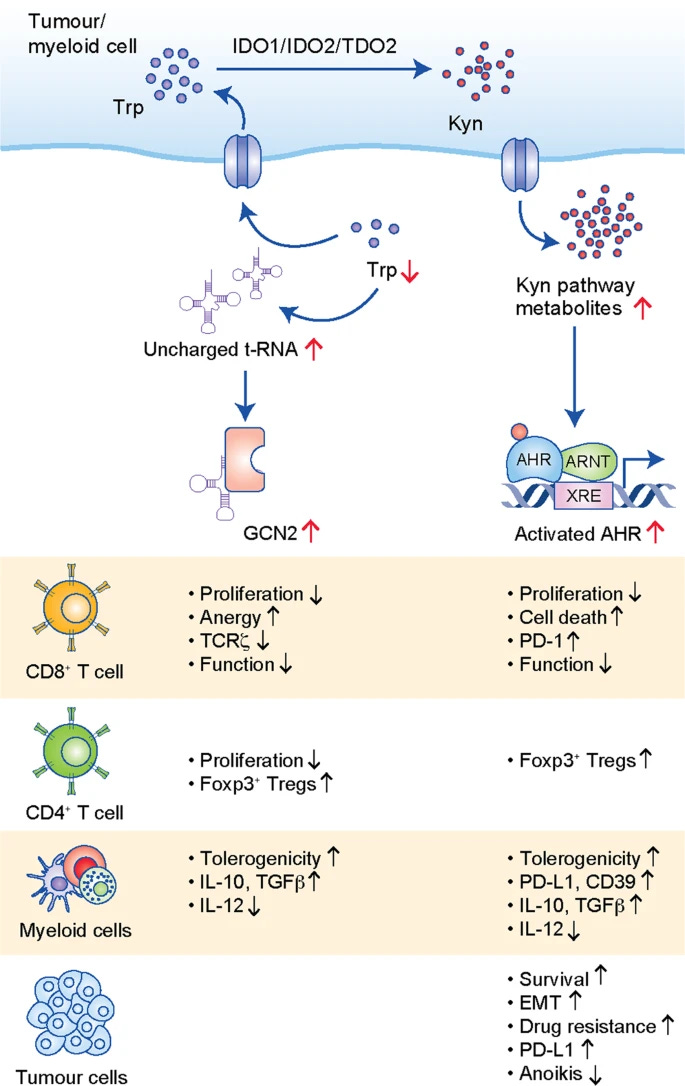
Suppression of memory CD8 T cell generation and function by tryptophan catabolism
We found that overexpression of IDO in vivo attenuated the generation of both central memory CD8+ T cells (T(CM)) and effector memory CD8+ T cells (T(EM)) while suppressing IDO activity promoted their generation. Moreover, IDO overexpression suppressed the effector function of T(CM) cells or T(CM) cell-mediated allograft rejection as well as their proliferation in vivo.
So here we partially found one of the reasons people with Long Covid or who get severe disease from the infection (any infection mostly) can fail to develop a proper response against the other proteins of SARS-CoV-2, by whatever mechanism if the body produces a significant amount of IDO, it attenuated (lowers the potency) of the generation of both central memory and effector memory CD8 cells, and suppressing IDO promoted their generation.
Viral persistence (or viral fragment persistence) will also induce this loop, but there is a hierarchical loss of function, it is not as some models point towards, where they made it sound like the T Cells just suddenly stop working properly. Meaning it is not “one and done” but rather “how long it remains unaddressed”. Proper metabolism of tryptophan is paramount to CD8 function to also keep cancer cells in check, so it isn’t merely the formation of immunological memory but the potency of the cells influenced by this dynamic.
IDO1 (the enzyme responsible to break down tryptophan into kynurenine) is an immunosuppressive enzyme, it shifts your cells into a tolerant state, and its higher presence enables cancer progression by affecting not only CD8 but Natural Killer and even B cells. Depletion of Tryotphan will lead the body to activate another enzyme (GCN2, a kinase) and it affects eIF2α, a protein responsible for controlling protein synthesis, in simple terms this leads to fewer CD8 cells and anergy, a state where the cell doesn’t respond as it should.
Even under different infections, proper Tryptophan metabolism has a deep effect, or in this case, IDO inhibition. In Zika infections, inhibiting the enzyme causes neuroprotection, and inhibition of the same augments the control of tuberculosis.
Here is where things get a little bit complicated. EBV, a known latent pathogen at first inhibits Interferon Gamma (one main proteins that make your body produce IDO), but afterward, it effectively induces IDO causing the CD8s to not work properly, thus effectively both escaping immune responses and aiding in tumor genesis. This can create a metabolic trap “IDO1-induced tryptophan consumption and production of tryptophan metabolites appeared to be responsible for inhibition of B-cell function”.
Belonging to the same family, Herpes Human Virus 6 (HHV-6) shares one very important gene with Alzheimer’s disease, IDO. In patients who develop HHV-6 encephalopathy, they found Kynurenine and Quinolinic Acid at higher levels, and Quinolinic Acid is known to potentially compromise the Blood Brain Barrier integrity. A similar trend can be found in many viral infections, where the pathogen manipulates IDO or Interferon Gamma signaling to establish chronic or latent infection, in fact, IDO itself is capable of inhibiting “tryptophan sufficiency signal” without the signal, the body doesn’t create cell growth, it hinders cell metabolism, growth factors, and mess with stress signals.
Influenza can also modulate the expression of IDO and creates a propitious immune-suppressed environment where bacterial co or superinfections take place. As per everything discussed so far in regards to T cell activity, inhibiting IDO enhances influenza T Cell responses.
The paper Tryptophan: A Unique Role in the Critically Ill should be read in its entirety by everyone. It touches on all major pathways and roles of the pathway, with many insights.
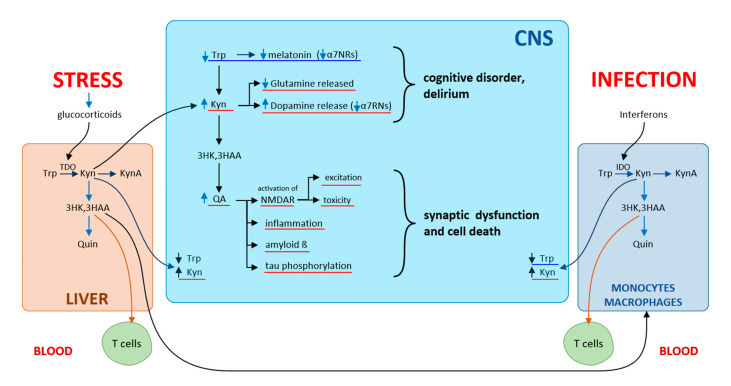
In critically ill patients, the Kyn pathway of Trp metabolism is activated due to inflammation and stress, further skewing immune balance. Kynurenines are important mediators of inter-organ communication. They are involved in immune response, inflammation, and excitatory neurotransmission. From a clinical standpoint, decreases in plasma Trp and an increased Kyn/Trp ratio are important predictors of an unfavorable clinical outcome. The modulation of Trp–Kyn metabolism using lifestyle (diets, BCAA, aerobic exercise), gut microbiome composition (probiotic based-therapies) and pharmacological interventions could help prevent and treat age-related disease with low grade chronic inflammation and immunosenescence, including PICS, of which persistent low-grade inflammation is a major component. Early mobilization and exercise in critically ill patients amplify skeletal muscle expression of KAT, and shifts peripheral Kyn metabolism towards production of KynA, which does not cross the blood–brain barrier. On the one hand, aerobic exercise can prevent the development of sarcopenia, and on the other hand, can act as an antidepressant as it reduces Kyn levels in the brain.
In fact, a sign of aging, or better yet “inflammaging” is precisely how the body shifts (shunts) into the Kynurenine pathway, effectively changing how Tryptophan metabolism works, an adaptative response towards anti-inflammation in an attempt to hinder the inflammatory burden in older age, since a hallmark of old age is poor protein absorption (meaning less tryptophan available), higher redox burden (you need a lot more antioxidants than a younger adult), and bioenergy failure (mitochondrial dysfunction, severely compromised NAD) A similar proposition to the viral infections above can be argued.
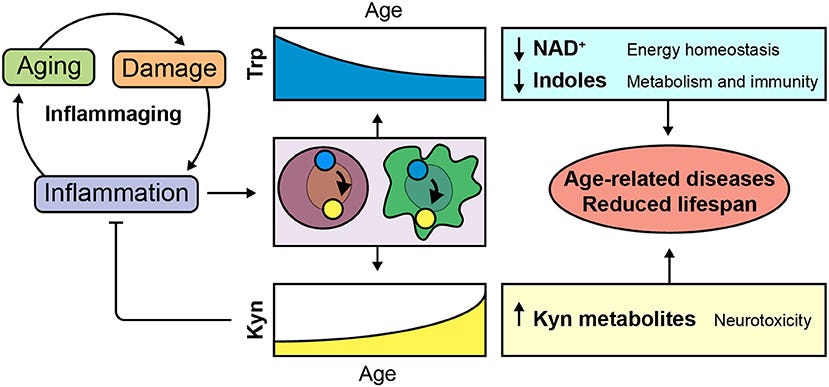
The body trades an overwhelming inflammatory response to immune tolerance, allowing certain pathogens to “stay around”. So far most of what is discussed here has been either directly, or tangentially implicated in severe and critical states of SARS-CoV-2 infection, but also in many of the injuries of the mRNA, and in Long Covid.
One continuous trend I have observed over the last 3 years, at moments transient, at moments long-lasting, besides brain fog that is, is memory issues. Acute tryptophan depletion, or poor tryptophan metabolism and availability will induce memory impairment. Tryptophan depletion specifically impaired long-term memory performance. In rats, a dose-dependent effect of tryptophan was found in learning and memory, later found in humans (below).
Before my closing remarks, to finish this linking many of my substacks for the best part of 12 months. The immune state of Endotoxic Tolerance itself is contingent on tryptophan catabolism, upon second exposure some of your immune cells express IDO to abrogate the severely inflammatory response from endotoxin. Same with other type of cells such as ovarian granulosa cells. Kynurenine itself can induce a tolerant state.
Besides physical exercise, tryptophan supplementation may be an avenue worth exploring but there are many caveats to it, since the metabolic pathway of tryptophan is the very definition of chaotic, but older people might benefit from it, people with gut inflammation or gut issues often benefit largely from supplementing it, and so does certain depressive/anxious states, I would advise proper dietary change and exercise first, but it is a powerful tool for you to explore.

Whey protein, one of the most researched supplements in scientific history, behind creatine alone, can help most people achieve proper tryptophan metabolism in the brain. It can also ameliorate anxiety and depression-like behavior by having an anti-inflammatory effect. Whey enriched with tryptophan enhances memory in MS. As a “joke” but with sound science behind it, whey has anti-viral properties.
If you go through the tryptophan or whey route you must add creatine. Creatine itself deserves a massive substack about it (if there is interest I could write about it, but truthfully there is a gigantic amount of content on the web already on it). Exercise, diet, and supplementing with these things are all things you may consider depending on your age, health, inflammatory status, and especially gut health status.
With the information present here, I may finally write the Long Covid, autoantibody substack, that took a massive turn in the last few days. What is discussed here is of high importance for a lot of what we will discuss there, and has significant implications for what the Spike is capable of inducing.

If you choose to support this work in whatever form, thank you !
A question for the reader, and input is welcome. The Long Covid post will be long, I will do my best to make it accessible and link everything else you may need to read for further context, but, the Endotoxin Tolerance one is ginormous, colossal. I personally hate "substack baiting" which is what I define as posting small, non-significant posts.
So choose. Either a massive, gigantic post in one single part, which will make it for a lengthy, difficult read. Or dividing into a few parts (2, 3 I don't know).
"What led me to this was a sudden lightbulb moment, as it often occurs in my weirdly wired brain, the thought is as follows." ❤....
Thank you for this soooo well researched article on Tryptophan.
And thank you for being so insightful & caring.
Do you take Trypthophan with carbs?
How often & how much you take? I was told to take Trypthophan with carbs to optimise absorbtion (otherwise to take 5HTP) at night.
In regards to Creatine, I was told to take 5gr(rounded teaspoon) before and after exercise and before sleep.
What are your thoughts?