
Persistent SARS-CoV-2 infections are more common
Than we previously thought

For the new subscribers or the ones unaware, I have been calling “out” the “persistently infected” state since 2020, and it has been one of my main interests, not only the fact that they would occur but the dynamics of how it would actually play out.
A couple of examples, with the second one bearing more related content discussed here.

Persistent, otherwise long-term infections are now known as one of the drivers of the evolutionary and antibody-evasive changes we can see in SARS-CoV-2, not solely to blame at first, but highly important dynamics to keep attention from here on out, as a considerable amount of people will start being “locked” in such a state.
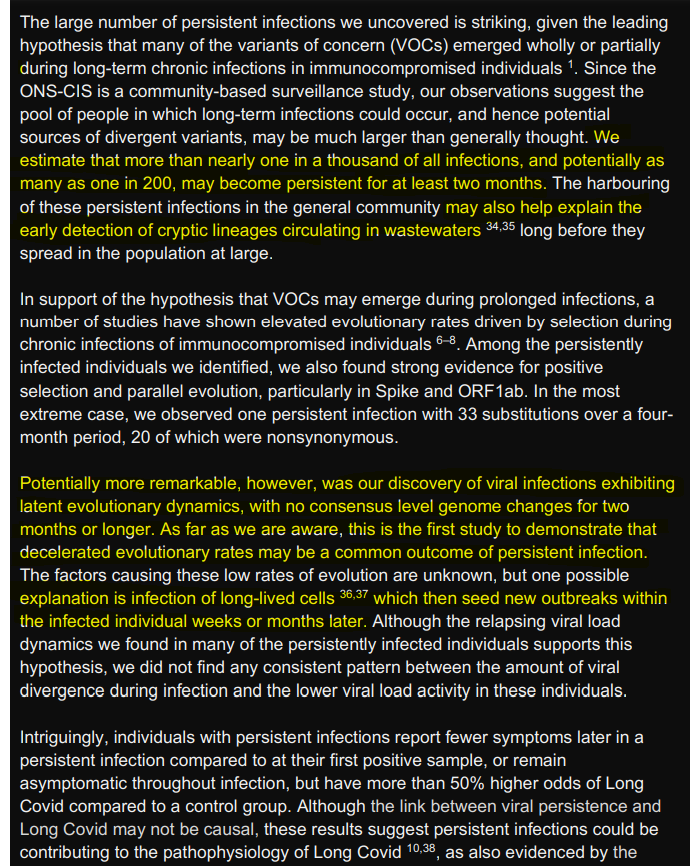
High number of SARS-CoV-2 persistent infections 2 uncovered through genetic analysis of samples from a 3 large community-based surveillance study
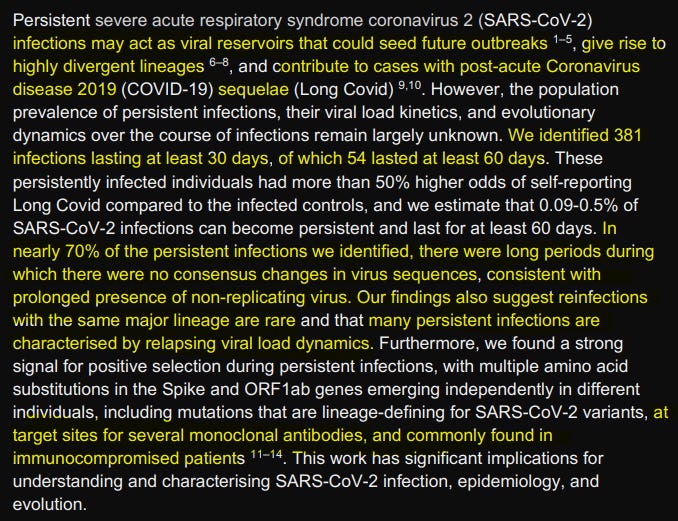
The image speaks for itself and now we get even closer to wider acceptance of the scientific and medical community of viral SARS-CoV-2 having potential viral reservoirs. The most intriguing highlight here is the “silent” phase of a persistent infection in which the viruses didn’t change, or replicate at all, lowkey implicating latency.
A lot of the mutations tracked down in this study fall in line with the mutations observed elsewhere, in which the virus achieves escape from different monoclonal antibodies, and these mutations are similar to the ones found in immunocompromised patients.
Identifying persistent infections
We considered more than 100,000 high-quality sequenced samples from the ONS CIS collected between 2nd November 2020 to 15th August 2022, and representing ~95,000 people living in ~75,000 households across the UK (see Methods). Individuals in the survey were typically sampled once a week for the first four weeks of their enrolment, and then monthly thereafter. To identify persistent infections we first limited the dataset to individuals with two or more RT-PCR positive samples with cycle threshold (Ct) values ≤30 (in which sequencing was attempted; a proxy for viral load), taken at least 26 days apart, and where the consensus sequences were of the same major lineages of Alpha, Delta, BA.1 or BA.2 (BA.4 and BA.5 not considered). If those sequences also shared the same rare single nucleotide polymorphisms (SNPs) at one or more sites relative to the major-lineage population-level consensus, we classified them as having a persistent infection.
We found 381 persistent infections with sequences spanning at least 26 days, of which 54 spanned at least 56 days, representing nearly 0.07% (54/77,561) of all individuals with one or more sequences (with Ct≤30) of the four major lineages we investigated in this study. Notably, 9% (2/23), 9% 135 (19/219), and 8% (8/208) of sequences from persistent infections with Alpha, Delta, and BA.1, respectively, were sampled weeks after when the corresponding major lineage has dropped to ≤1% frequency of all the ONS-CIS sequences; the longest infection was with BA.1 and lasted for at least 193 days.
To identify such infections they used 100.000 sequenced samples representing 95.000, the frequency of the sampling is also mentioned. A consensus (or canonical) sequence here is defined by the most common sequences of the virus, including mutations, and here they used Alpha, Delta, BA.1, and BA.2.
If the sequences from these individuals share rare SNPs (here is a great short video on SNP).
The interesting part that got my attention was the highlighted, in which roughly 9% of the sequences were sampled weeks after each lineage (Alpha, Delta, etc) dropped to less than 1% of all sequences in the database used, and the longest infection was BA. 1 lasting 193 days. An Omicron variant, known for being highly immune evasive lasting close to 200 days.
The authors also found that under their parameters, reinfections might be overestimated compared to persistently infected individuals, and in a very short section of the paper for what I could assume obvious reasons, they found evidence of a non-replicating period during this persistent infection, in other words, a latency period.
Emergence of notable mutations
We observed several mutations at the same genomic positions in multiple individuals over the course of their persistent infections. For example, three BA.2 infected individuals from different households acquired a mutation at codon position 547 in Spike ), two of which were the T547K mutation which is a lineage-defining mutation for BA.1, and one the K547T mutation). Strikingly, twelve individuals acquired a deletion (ORF1ab: Δ81-87) in the NSP1 coding region. A similar deletion has previously been observed during the chronic infection of an immunocompromised individual with cancer, and was associated with lower type I interferon response in infected cells.
Overall, we observed a strong signal for positive selection in Spike, with nearly nine fold more nonsynonymous compared to synonymous mutations With a total of seven nonsynonymous mutations, ORF8 had the highest per base number of nonsynonymous mutations followed by Spike with 61 nonsynonymous mutations.
Besides the specificity of the position of the mutations, the above paragraphs are straightforward to understand, different individuals from different households develop the same mutations, and some of these mutations are lineage defining, meaning these are the mutations that impact how the virus behaves/affect people the most, 12 people had a deletion in one of the proteins, found in a cancer patient, to say perhaps some of the persistently infected people have poor immune response towards the infection, especially in the first few days.
Besides the Spike, the ORF8 was one of the proteins with the most nonsynonymous mutations, in plain English, a nonsynonymous mutation means a mutation that has a “real” impact on how the virus affects the host, and this can be either positive or negative. Below is a rather complex substack covering the other proteins of SARS-CoV-2 and what they do (with ORF8 being one of the “nastiest” ones").
The closing remarks of the paper, as in line with many of my and others observations for the last 2+ years, and while outside the scope of this paper, hint at the potential for both viral latency and reservoir. Besides creating possibly creating reservoir inside certain cell types (it does not create in Lymphocytes, I have already written about this many months ago), it definitely can (more like will) create a reservoir in the gut, especially with bacteria, something I have hinted at more than once here.
Work in relation to both Long Covid and latency/reservoir/persistent infections is incredibly important by the simple fact that we effectively now have dozens of millions, potentially more than that, of people with various degrees of persistent infection, and while I will still cover this in the following weeks, this has many unforeseen outcomes. First, the immune shift in persistently infected people and the potential to become evolutionary pitstops for the virus, secondly autoimmunity, not solely by itself given its molecular mimicry, but the fact that SARS-CoV-2 is the best friend of every other latent and chronic infection, such as Lyme, Epstein Barr, certain Herpes viruses, and thirdly the potential for accelerated evolution between SARS-CoV-2 and other pathogens together, something that was merely one of my “crazy ideas” in 2021, now a verifiable fact.
Leaving the whole political narrative aside (virus was bad, the virus was never bad, etc) the fact remains the virus would always cause long-term damage and havoc, so a focus on avoiding such outcomes is not merely good from a public health standpoint, but necessary.
And since we are talking about Long Covid, a rather interesting paper was published just yesterday.
Persistent short nighttime sleep duration is associated with a greater post-COVID risk in fully mRNA-vaccinated individuals

Sleeping too little will literally change (for the worse) your immune response, but it goes far beyond that, it won’t merely change your immune response toward vaccination or infections. Sleeping too little will affect your entire metabolism and cellular function, one specific highly important in the context of SARS-CoV-2.
Effects of Sleep Deprivation on the Tryptophan Metabolism
Sleep has a regulatory role in maintaining metabolic homeostasis and cellular functions. Inadequate sleep time and sleep disorders have become more prevalent in the modern lifestyle. Fragmentation of sleep pattern alters critical intracellular second messengers and neurotransmitters which have key functions in brain development and behavioral functions. Tryptophan metabolism has also been found to get altered in SD and it is linked to various neurodegenerative diseases. The kynurenine pathway is a major regulator of the immune response. Adequate sleep alleviates neuroinflammation and facilitates the cellular clearance of metabolic toxins produced within the brain, while sleep deprivation activates the enzymatic degradation of tryptophan via the kynurenine pathway, which results in an increased accumulation of neurotoxic metabolites. SD causes increased production and accumulation of kynurenic acid in various regions of the brain. Higher levels of kynurenic acid have been found to trigger apoptosis, leads to cognitive decline, and inhibit neurogenesis.
In case you missed it or are new, the Kynurenine Pathway is one of the most important factors both short, medium, and long-term of this whole pandemic.
Changes in Tryptophan Metabolism will directly affect your entire body and especially your immune system, creating many metabolic “traps” and feedback loops of your immune cells, such loops are easily exploited by latent and chronic pathogens to further induce damage, bioenergy dysregulation (no energy, long-lasting fatigue, brain fog, etc), and can even help induce autoimmunity. And of course, it does has a correlation with another topic I am highly interested in and covered here Endotoxins.
Would be ironic if in hindsight most people, regardless of vaccination status, could have avoided both autoimmunity and Long Covid by merely supplementing Tryptophan and Melatonin. This isn’t exactly the first time I say this too. In the end, the Kynurenine Pathway and Tryptophan Metabolism play a very significant role in many of the dynamics I wrote and will write, but I will leave these for when I write the pieces.
In summary, a lot of people should supplement either one of those (melatonin or tryptophan) for the foreseeable future, and the more symptomatic you are, the higher the likelihood you will respond well to them. I personally take both daily and have for years FYI.
Also as a point of interest, if the reader wants to dig further, a quick search engine query in regards to tryptophan+choose any chronic/latent infection will give you hours of reading material and quite a few insights.
The next topic will definitely be in regards to Endotoxins unless some meaningful paper is published in the next few days.
I am grateful for the support, and for the ones who share anything they find useful.
Igor- do you really believe whoever created this virus knew all these “effects” we are seeing today? Somehow I don’t think they knew all this, yet I don’t think they are upset by it either.
I think you give the creator of the virus too much credit.
I was under the impression that one should not take melatonin on a regular basis as it can interfere with the body own mechanism of producing it. Perhaps, John, you have written plenty in this regard. I take plenty of supplements a day and have also read warning about giving the liver too much work. I do have melatonin among them but refrain to take it on a daily basis. Very few stacks cover the depth and complexity you address in yours. Covid is a full encyclopaedia for those who started at Volume I and I can tell that several more volumes are yet to be written.