

SARS-CoV-2, the Brain and the Sugar
SARS-CoV-2, the Brain and the Sugar
Part II, kinda...

Today I will be covering seamlessly unconnected papers, but trust me, we are going somewhere with them, and they link to a broader “hypothesis”.
Directly correlates to this post.

SARS-CoV-2 spike protein induces long-term TLR4-mediated synapse and cognitive loss recapitulating Post-COVID syndrome
Abstrac
Cognitive dysfunction is often reported in post-COVID patients, but its underlying mechanisms remain unknown. While some evidence indicate that SARS-CoV-2 can reach and directly impact the brain, others suggest viral neuroinvasion as a rare event. Independently of brain viral infection, the ability of SARS-CoV-2 spike (S) protein to cross the BBB and reach memory related brain regions has already been shown. Here, we demonstrate that brain infusion of S protein in mice induces late cognitive impairment and increases serum levels of neurofilament light chain (NFL), which recapitulates post-COVID features. Neuroinflammation, hippocampal microgliosis and synapse loss are induced by S protein. Increased engulfment of hippocampal presynaptic terminals late after S protein brain infusion were found to temporally correlate with cognitive deficit in mice. Blockage of TLR4 signaling prevented S-associated detrimental effects on synapse and memory loss. In a cohort of 86 patients recovered from mild COVID-19, genotype GG TLR4 61 -2604G>A (rs10759931) was associated with poor cognitive outcome. Collectively, these findings indicate that S protein directly impacts the brain and suggest that TLR4 is a potential target to prevent post-COVID cognitive dysfunction
Alongside many of the papers that I have already covered here, we got another paper demonstrating the mere presence of the Spike [S] Protein alone is enough to initiate and set off inflammatory changes and elicit a specific immune response.
I would like to make a remark very early before we go further. This research was done with brain infusion, meaning the Spike was directly injected into the bloodstream going to the brain. First some sciency words explanation.
Microglias are the immune system cells of the nervous system and the brain, and Microgliosis is the activation of said cells in response to some sort of insult, like an infection, or a pathogen. Synapses are the “wiring” in your brain.
So what does the abstract means in common terms ? The Spike Protein alone, without all the complexity of the viral infection, is enough to cause inflammation and activate the immune cells in the brain causing neuroinflammation and affecting cognitive function driven by Toll-Like Receptor 4. This post of mine will give you an idea of what is going on “under the hood”
During SARS-CoV-2 infection, cells produce and release variable amounts of viral particles and proteins, including the S protein. The S1 was shown to cross the BBB, reaching different memory-related regions of the brain in a mouse model of SARS-CoV-2 infection. Inflammation and increased BBB permeability were also shown in in vitro models of S1 exposure. Likewise, the protein was detected in the central nervous system (CNS) of 90 COVID-19 patients, irrespective of viral RNA detection. In addition, increased levels of proinflammatory cytokines and brain gliosis have been reported in severe COVID-19 patients. Nonetheless, proof concerning the acute and chronic impact of S protein on COVID-19 brain dysfunction and its underlying mechanisms are still lacking.
Most experimental studies investigating the effects of SARS-CoV-2 have focused on acute infection, especially on peripheral tissues. Few studies have used experimental models to evaluate the possible mechanism of post-COVID syndrome. Here, we developed a mouse model of intracerebroventricular (icv) of S exposure to understand the role of this protein in late cognitive impairment after viral infection. Here, we infused S protein in the brains of mice and performed a long-term (45 days) follow-up of the behavioral, neuropathological, and molecular consequences. We report late cognitive impairment, synapse loss, and microglial engulfment of presynaptic terminals after icv infusion of S protein.
I like the honesty of the authors on raising a point many, MANY, well, everyone refuses to elaborate or even think about it. The variability of how many viral particles and proteins are produced during a viral infection. And how most of the studies are done with acute or severe patients, using other tissues and biomarkers, not actually the brain. They are attempting to elucidate the cognitive decline and neuroinflammation after the viral infection, and why they sometimes persist.
I would like to add the human brain is unbelievably more complex than any other animal, and we are much more resilient, so don’t read this as a doom scenario.
RESULTS
SARS-CoV-2 spike protein induces long-term cognitive impairment and synapse loss in mice
The S protein had no impact on memory function in the early phase after brain infusion while in later time points infused mice failed to recognize the novel object…
Late cognitive dysfunction induced by S protein infusion was confirmed by the Morris Water Maze (MWM) test, a task widely used to assess spatial memory in rodents. Mice infused with S protein showed higher latency time to find the submerged platform in sessions 3 and 4 of MWM training, when compared to control mice. Also, S protein-infused mice showed reduced memory retention, as indicated by the decreased time spent by these animals in the target quadrant during the probe trial.
Synapse loss is strongly correlated to the cognitive decline observed in neurodegenerative diseases. Thus, we next investigated whether S protein induces synapse damage in the mouse hippocampus, a brain region critical for memory consolidation. S protein-infused mice did not show changes in synaptic density at the early stages
The infusion of Spike doesn’t cause short-term changes and no perceptible measurements, only after weeks, the changes are measurable.
SARS-CoV-2 spike protein triggers late neuroinflammation in mice Neurodegeneration associated with viral brain infections can be mediated either by direct neuronal injury or by neuroinflammation. To advance in the understanding of the genuine impact of SP on neurons, cultured primary cortical neurons were incubated with S protein for 24h. Neuron exposure to S protein did not affect neuron morphology…Also, S protein incubation also had no effect on the neuronal synaptic density and puncta suggesting that neurons are not directly affected by S protein.
We found that S protein stimulation increased Iba-1 immunoreactivity ) and upregulated TNF, INF-β and IL-6 expression, without affecting IL-1β and IFNAR2.
We found that at the early stage after icv. injection of S protein neither changed the number and morphology of microglia nor increased the levels of TNF-α, IL-1β, IL-6, INF-β and IFNAR1.
The Spike protein itself did not affect the morphology [shape, incredibly important in molecular biology], nor the synaptic density [how many “wires” are together in a crude way] therefore demonstrating the Spike does not in fact directly affect neurons (an argument made by a few).
What it does demonstrate, and what many were aware of already was the Spike Protein itself upregulates [increases the production of] inflammatory proteins inside your brain, which are a problem under specific circumstances. And again, in line with previous papers, they found this inflammation does not happen very early, it takes weeks to develop. This is usually a sign of either persistent inflammation, latent infection, or minor immune dysfunction in your brain.
I have made this observation many times, and I will do it many other times (in fact, I have whole posts written about it), what is happening is “easy” to understand. You need to superficially understand this highly important paper first.
When you get infected (or injected), your immune system will attack the virus, it will break it down into small pieces so your body can identify the pieces and know what to “target”. In my opinion, a lot of these highly inflammatory outcomes, both short and long-term are being driven by what the paper above mentions. Similitary in antigenic sites to other pathogens, leading to an immune response towards those pathogens. For what could be many different reasons, the body sometimes doesn’t get rid of these small Spike Protein pieces for weeks, leading to what I referred many times as Low-grade Long-term inflammation.
The paper goes into discussing how the Spike Protein itself uses C1q, a complement, to induce microglia synaptic phagocytosis. I will skip this part because what they write is small, and complements are really complex, I would need 3 extensive pieces alone for this. But this process is important because it is how many degenerative diseases progress.
This leads to my previous Covid and the Brain post. The Spike alone is inducing injury, but I agree with the authors of that paper, it is more like Hit and Run. The virus and Spike Protein are hitting you hard and draining the body of resources fast enough that secondary anything will hit harder and drive injury and inflammation. And it all goes back into Mitochondria, and metabolism. Even that C1q mediated loss.
As a good friend said, “It is all the mitochondria, bro”.
They go further to discuss the following.
TLR-4 mediates cognitive dysfunction induced by SARS-CoV-2 spike protein
Together, these data suggest that TLR4 activation mediates cognitive deficit and synaptic pruning induced by S protein in mice.
I want you to do something. The highly important paper I just referred to above, remember ? Is it opened in another tab ? Search each of the pathogens listed there on Google and add “TLR-4”. Here is also another clue. You can easily connect the dots yourself at this point.
The Discussion section makes it easier to understand the rest of the paper for the layperson.
“Ok, I get the brain part of the title, but where the hell the sugar comes in ? That little mention of microglia metabolism ?” Not quite. I finally have a sizable piece of my puzzle.
Since mid-2020 I have been asking myself, and the whole point of my entire research was always the question “Why this viral infection drains your body from resources so fast, so aggressive, often inducing inflammation BEFORE the active phase of infection, undetected, not after” (Back in Alpha/Delta variant days mind you). Why not only if feed on sugar, drain your body out of fuel, but apparently actively harms you by using the sugar. Glutathione deficiency was argued as the most likely cause of serious damage and death in Covid-19 patients back in *check notes
May. 2020.
Elevated plasma level of the glycolysis byproduct methylglyoxal on admission is an independent biomarker of mortality in ICU COVID-19 patients
Biomarkers to identify ICU COVID-19 patients at high risk for mortality are urgently needed for therapeutic care and management. Here we found plasma levels of the glycolysis byproduct methylglyoxal (MG) were 4.4-fold higher in ICU patients upon admission that later died (n = 33), and 1.7-fold higher in ICU patients that survived (n = 32),compared to uninfected controls (n = 30). The increased MG in patients that died correlated inversely with the levels of the MG-degrading enzyme glyoxalase-1 (r2 = − 0.50), and its co-factor »»glutathione«« (r2 = − 0.63), and positively with monocytes (r2 = 0.29). The inflammation markers, SSAO (r2 = 0.52), TNF-α (r2 = 0.41), IL-1β (r2 = 0.25), CRP (r2 = 0.26) also correlated positively with MG. Logistic regression analysis provides evidence of a significant relationship between the elevated MG upon admission into ICU and death (P < 0.0001), with 42% of the death variability explained. From these data we conclude that elevated plasma MG on admission is a novel independent biomarker that predicts mortality in ICU COVID-19 patients.
One of my main questions, and arguably by my own observations, driving the disease was something directly linked to this paper. How or why the virus drains your antioxidant levels so fast, at the point you get all the different pathologies after a medium to severe infection, and why it is so highly inflammatory. ROS, Oxidative stress alone [cell rust produced by different mechanisms] alone couldn’t account for it.
Methylglyoxal [MG from here on] is a known byproduct of carbohydrate metabolism, and one of the co-factors [needs another substance to do X] to degrade MG is Glutathione.
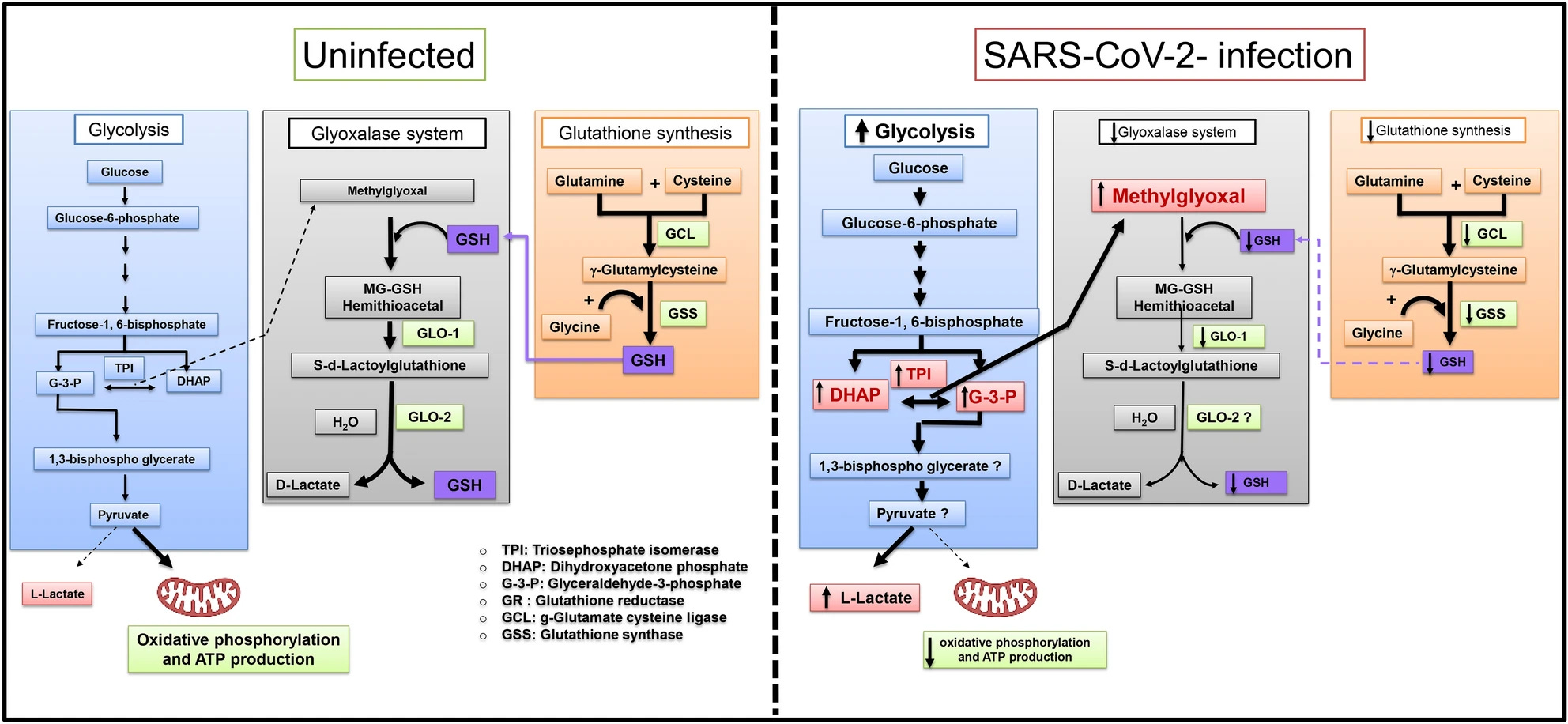
Like most viruses, after entry SARS-CoV-2 reprograms metabolism in the infected cells to obtain the building blocks needed for replication. These metabolic changes include upregulating glycolysis for faster production of ATP, upregulating the oxidative arm of the pentose phosphate pathway (PPP) for synthesis of nucleotides, amino acids, and lipids, and attenuating oxidative phosphorylation in the mitochondria of the infected host cells23,24,25.
In addition to metabolic changes in the infected cells, the immune cells of the host also upregulate these pathways to orchestrate their highly specific series of responses to clear SARS-CoV-2 infection and repair the cellular damages26,27,28,29,30.
Polarized M1 pro-inflammatory macrophages rearrange their metabolism to utilize glycolysis rather than oxidative phosphorylation for rapid ATP synthesis, and the PPP for the oxidative burst needed for destroying the infectious agent30. The latter process is commonly termed the Warburg effect28. M1 macrophages also upregulate glycolysis by increasing hypoxia-inducible transcription factor 1α (HIF-1α) and glycolysis-related proteins in an O2-independent manner28,33. Danger-associated molecular patterns (DAMPs) from damaged and dying cells also activate Toll-like receptors and inflammasomes to increase inflammation and oxidative stress34.
In addition to ATP, anaerobic glycolysis also generates the highly cytotoxic byproduct, methylglyoxal (MG) from the interconversion of glyceraldehyde 3-phosphate and dihydroxyacetone phosphate by topoisomerase-1 (TPI-1)35. In healthy, uninfected individuals, plasma and tissue of MG levels are kept low by the actions of dual-enzyme glyoxalase system36
The increase in oxidative stress will also increase demand for GSH. The increase in MG synthesis arising from upregulation of glycolysis coupled with decreases in free GSH and Glo1 levels should lead to accumulation of MG in blood and tissues of COVID-19 patients. At supraphysiologic levels, MG disrupts the function of endothelial and epithelial cells, resulting in microvascular leakage, and clots42,43,44,45. Supraphysiological levels of MG will also potentiate inflammation in many cell types by activating NF-κB46, the NLR family pyrin domain containing 3 (NRLP3) inflammasome47, and by inducing expression of the ectoenzyme vascular adhesion protein 1 and its cleaved analog semicarbazide-sensitive amine oxidase (SSAO)48. Elevated MG is also an underlying cause for tissue fibrosis49, a pathobiology reported in COVID-19 patients.
These paragraphs are really hard to understand if you are not into metabolic medicine or metabolism in general, but they are important for anyone to read. Ignore the words of biochemicals and proteins and molecules you don’t understand, the general idea is what is important.
The second paragraph is of similar importance because your own body will use a similar response [making your cells use more of this sugar > fuel pathway], the upregulation of HIF-1α, activation of Toll-Like Receptors, and inflammasomes. All this leads to a continued depletion of the necessary resources to produce Glutathione, further leading to a decrease of the same in the whole body. Supraphysiologic literally means at higher levels than the body would naturally have. I have covered every single of these markers.
Inflammasome.
HIF-1α
Others have shown that glycolysis and the oxidative arm of the PPP are upregulated in SARS-CoV-2-infected cells to provide the substrates needed for replication55,56, and in immune cells to eliminate SARS-CoV-2 infection and repair any cellular damage27,28,29. As such, we concluded that MG synthesis is likely increasing in COVID-19 patients. In this study, we focused on whether MG degradation is being compromised in COVID-19 ICU patients. We found that plasma levels of glutathione, and Glo1 were significantly lower in ICU COVID-19 patients that died compared to ICU COVID-19 patients that survived. In an earlier report Horowitz et al.57 showed that oral and intravenous glutathione and the glutathione precursors (N-acetylcysteine) attenuated activation of NF-κB, cytokine storm syndrome and respiratory distress syndrome seen in COVID-19 patients with pneumonia. Thus, it is likely that intravenous glutathione and the glutathione precursors (N-acetylcysteine) administration were alleviating the oxidative stress and providing the glutathione needed for the formation of MG-glutathione hemiacetal.
Who would have thought that NAC would be helpful from so many perspectives one could look into this virus… further reading into the effects of too much sugar in your bloodstream.
Now, why this is a paper on carbs, inflammation, and severity of Covid is in a post about the brain ? How this ties with neurodegeneration, amyloid, and everything else ?
Methylglyoxal Induces Mitochondrial Dysfunction and Cell Death in Liver
Degradation of glucose is aberrantly increased in hyperglycemia, which causes various harmful effects on the liver. Methylglyoxal is produced during glucose degradation and the levels of methylglyoxal are increased in diabetes patients.
Collectively, our results showed that methylglyoxal increases cell death and induces liver toxicity, which results from ROS-mediated mitochondrial dysfunction and oxidative stress.
From here.
Accumulation of methylglyoxal (MG) contributes to oxidative stress, apoptosis, and mitochondrial dysfunction, leading to the development of type 2 diabetes and cardiovascular diseases. Inhibition of mitochondrial abnormalities induced by MG in the heart may improve and delay the progression of heart failure.
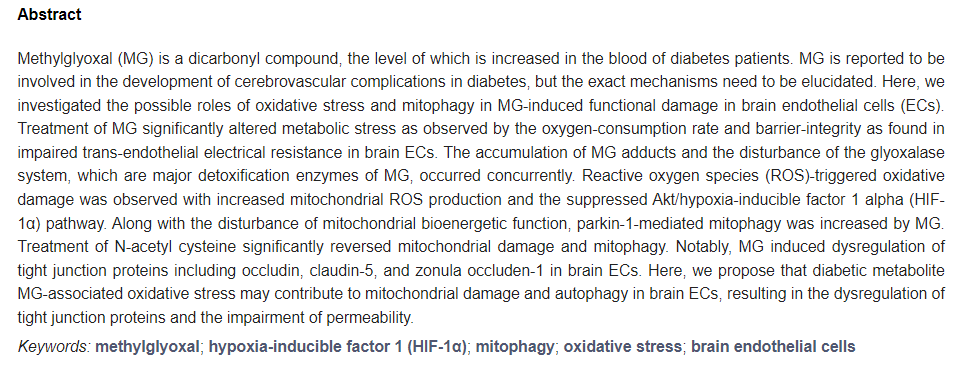
Methylglyoxal-Induced Dysfunction in Brain Endothelial Cells via the Suppression of Akt/HIF-1α Pathway and Activation of Mitophagy Associated with Increased Reactive Oxygen Species
Methylglyoxal and Glyoxal as Potential Peripheral Markers for MCI Diagnosis and Their Effects on the Expression of Neurotrophic, Inflammatory and Neurodegenerative Factors in Neurons and in Neuronal Derived-Extracellular Vesicles
Serum concentration of an inflammatory glycotoxin, methylglyoxal, is associated with increased cognitive decline in elderly individuals
I don’t want to spoil my Amyloid post, but I left enough clues in many pieces lately so you can make sense of what is happening, and where it is coming from. Does the Spike Protein induce magical interactions and possessing properties unknown to science, or it is all about mitochondrial function, too much sugar, and uncontrolled inflammation ? You tell me.

I hope you all have a very nice weekend.
Certainly seems to parallel our household experience. Two of five vaxxed had more severe symptoms - both pre-diabetic with almost completely carb based diet. One had less severe symptoms - lower carb diet. (Three others didn't get sick including myself - unvaxxed low carb diet.) There's always more to the story and much we don't know yet.
A lot to digest and I will get through it with a coffee. I have/had covid, pureblooded, had literally zero symptoms. What is weird is that I have asthma and generally that is my warning that i am about to get sick i start getting worse asthma 2 or 3 days before the cold comes. Since I got covid my Asthma has been very good. It could even be better than it usually it, or at least not at all worse. This is very strange as everyone has been telling me for 2yrs to get the jab "because you have asthma"..