

It is no secret recombination in regards to SARS-CoV-2 has been an interest of mine for quite a while, and I have kept an eye and tracked down interesting and enlighting papers here. Recombination is an amazing strategy employed by viruses to further evolve and evade the host’s immune response, and my attention was always on how said events would affect the evolutionary direction when faced with a massive population of mildly immunosuppressed hosts.
Especially under what I named over a year ago “Chronic Infection”. Another question I raised was if the virus would/could evolve to evade monoclonal antibody treatment, I marginally knew it was possible, but wanted evidence of it, and an understanding of how.

SARS-CoV-2 evolution and evasion from multiple antibody treatments in a cancer patient
Infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in immunocompromised patients may lead to accelerated viral mutation rate, immune evasion and persistent viral shedding over many months. Here we report the case of a severely immunocompromised cancer patient infected with the Delta variant of SARS-CoV-2 for over 8 months. Genome sequencing of samples taken after repeated monoclonal antibody treatments reveal the emergence and accumulation of mutations enabling escape from neutralization by antibodies. Mutations emerging in accessory and non-structural viral proteins target specific residues of immunomodulatory domains, potentially leading to loss of some functions, while preserving others. The mutated virus managed to completely overcome neutralization by monoclonal antibodies while remaining viable and infective. Our results suggest that the loss of specific immunomodulatory viral functions might confer a selective advantage in immunocompromised hosts. We also compare between mutations emerging in the presence and absence of neutralizing antibodies.
Highlights
SARS-CoV-2 undergoes rapid evolution in an immunocompromised, chronically infected cancer patient, overcoming neutralization by two monoclonal antibody cocktail treatments
Receptor binding domain (RBD) mutations emerging after monoclonal antibody treatment enable effective escape from neutralization in the absence of adaptive immunity
Some emerging mutations are predicted to disrupt immunomodulatory viral proteins, including prevention of ORF8 homodimerization, mislocalization of ORF3a in host cells and alteration of the host-suppressive function of NSP1
The abstract says it all, and brings us to a theme I will slowly (not really) write about. There is a massive overfocus on the Spike Protein, but SARS-CoV-2 research has reached such an advanced stage that our understanding of its other proteins is now reaching an adequate level. And they are nasty, more on this at a later date.
The subject of the paper had a chronic infection lasting astounding 8 months, and by sequencing the virus, the authors were able to track its evolution, how it adapted and the substitution of amino acids.
Oncological findings included: Malignant melanoma, Diffuse large B-cell lymphoma (DLBCL) and Squamous Cell Carcinoma (SCC). Background diseases included: fibromyalgia, treated asthma and Chronic Obstructive Pulmonary Disease (COPD).
These are all important to note because they affect your immune response and modulate your immune memory too, there is quite a few papers on B-cell dysfunction and your immune response towards the virus and the vaccine.
The distribution of emerging mutations is uneven, with the accessory proteins, ORF8, ORF10 and ORF3a, accumulating the most mutations (10.9, 8.6 and 6 mutations per kilobase (mKb), respectively). The Spike gene is the most mutated structural protein coding gene, with 23 distinct nonsynonymous mutations, 8 of which overlap the locus coding for the receptor binding domain (RBD), making it the most densely mutated locus overall (∼6 mKb in the Spike gene, ∼12 in the RBD alone).
The ORFs will be important later, I find it intriguing that the ORF10 was among the accessory proteins with most mutations, and obviously, as usual, the one with most mutations was the structural protein S, the famous Spike you are familiar and heard about for over 2 years.
The patient was initially diagnosed with SARS-CoV-2 infection in September, 2021, with high viral load (17Ct), characteristic of Delta variant infections from this period.. Within the same month, the patient was treated with the monoclonal antibody cocktail REGEN-COV (casirivimab and imdevimab). Following the monoclonal antibody treatment, two negative PCR test results indicated the infection was resolved and cancer therapy was initiated. Over the two following months, the patient received immunochemotherapy, according to the R-CHOP protocol, including the immunosuppressant Rituximab (Anti-CD20). In December, 2021, a positive PCR test indicated that the infection persisted and the first viral genome sample was sequenced.
We see an accumulation of RBD mutations over time, specifically in amino acids found to enable escape from binding by antibodies (Figure 3). The mutations G446D, E484K and Q493E all confer escape from the REGEN-COV monoclonal antibodies used to treat the patient, according to deep mutational scanning11.
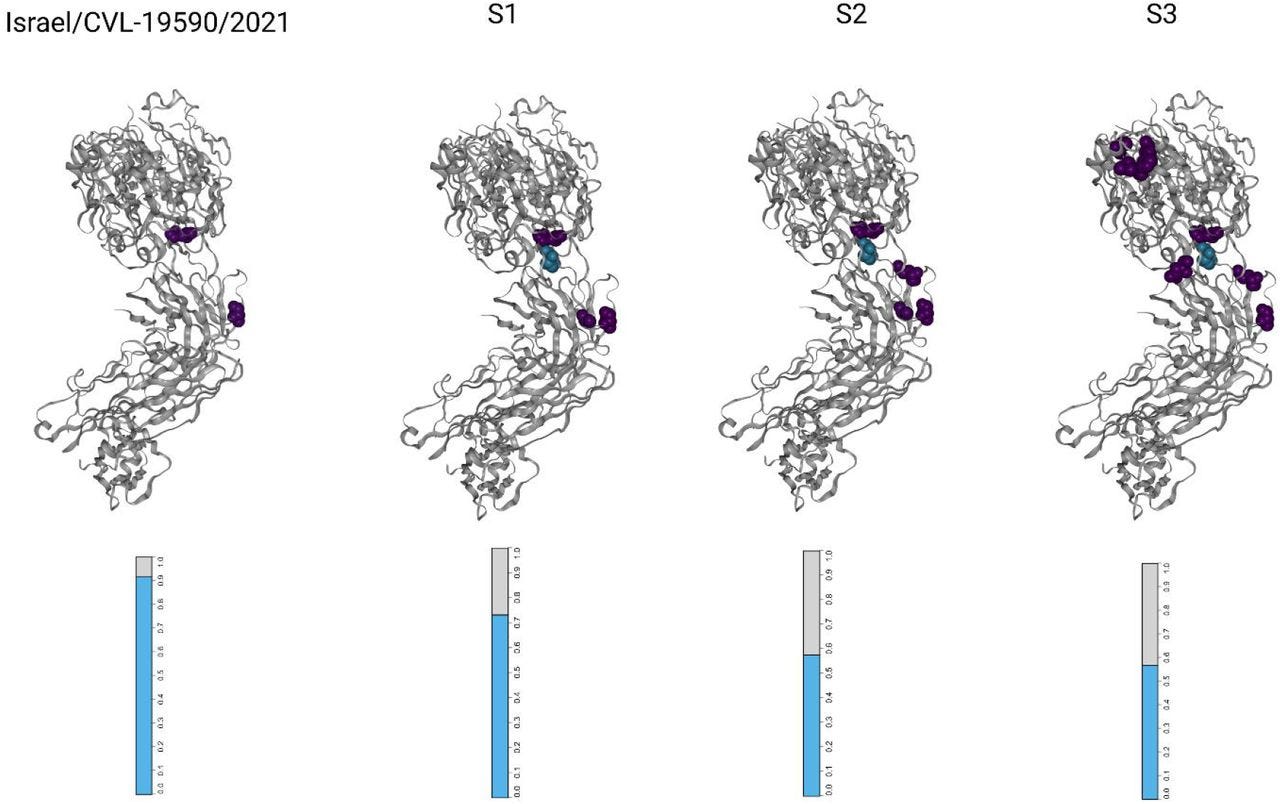
As I usually write, I think there is an argument to be made, that under specific circumstances, propitious to viral persistence within someone, especially attentive to the portion of “starts immunosuppressive treatments, tests positive again”, while there is the real chance this could be merely a breakthrough infection, the higher likelihood would be the same infection merely acting up again, since the mutations were tracked down.
The mutation E484K is one known for being a case of convergent evolution, present in multiple other variants and with extensive evidence of its capacity to grant the variant fairly extensive immune evasion.
In this case study, we characterize the evolution of SARS-CoV-2 in an immunocompromised cancer patient, covering 6 out of 9 months of infection (the infection remains unresolved at the time of writing). Over the long course of infection, the virus survived two treatments of potent monoclonal antibody therapy, remaining infectious and viable despite an exceptionally high concentration of serum antibodies. The inability of adaptive immunity to mitigate the infection could be partly attributed to treatment with Rituximab, an anti-CD20 immunosuppressant known to severely impair serological response to SARS-CoV-2
After so many months, and extensive treatment, the infection remains unresolved, the virus is still infective, therefore somewhat transmissible, and this person becomes a factory of a unique supercharged variant. I would like to add that even with an immunosuppressant treatment, it is much more likely that the exceptionally high serum antibodies weren’t useful because of the mutations, and not just the anti-CD20 treatment.
I highlighted such a passage because this is exactly what you find in many of the vaccinated with breakthrough infections. High levels of non-neutralizing antibodies. And the literally of how these useless antibodies led to the evolution of the virus is extensive by now.
Here is an old piece with plenty.
I will briefly cover this paper published at the end of May. It is important.
The effect of COVID-19 mRNA vaccine on human lung carcinoma cells in vitro by means of Raman spectroscopy and imaging
The effect of COVID-19 mRNA vaccine on human lung carcinoma epithelial cells (A549) in vitro as a convenient preclinical model has been studied by means of Raman spectroscopy and imaging. The paper focuses on Raman imaging as a tool to explore apoptosis and oxidative phosphorylation in mitochondrial dysfunctions. The Raman results demonstrate alterations in the oxidation-reduction pathways associated with cytochrome c. We found that the COVID-19 mRNA vaccine downregulates the concentration of cytochrome c upon incubation with tumorous lung cells.
Cytochrome c activity in the efficiency of oxidative phosphorylation and apoptosis, is down-regulated by the COVID-19 mRNA vaccine. Lower concentration of oxidized cytochrome c observed in mitochondria in human lung cancer cells upon incubation with COVID-19 mRNA vaccine leads to reduced oxidative phosphorylation (respiration), and lessened ATP production. Incubation in vitro cells with mRNA vaccine increases significantly de novo lipids synthesis in lipid droplets and rough endoplasmic reticulum.
Why is this important ? Because I have covered this precise mechanism in another type of cells.
The paper titled Decoding COVID-19 mRNA Vaccine Immunometabolism in Central Nervous System: human brain normal glial and glioma cells by Raman imaging. (Incidentally one of the authors is the same as the paper above).
“Are you analyzing both papers solely based on the fact they have cancer in common ?” No, the cancer patient and her underlying diseases, the paper above, and the one linked above all have something in common, even cancer.
Mitochondrial dysfunction, among some other variables. The Decoding paper is one with remarkable prescience I would say. It shows under the design of their study that the mRNA vaccine from Pfizer changes mitochondrial metabolism, producing less respiration and energy, and therefore it can lead to a lower immune response, both towards the vaccine, the consequential viral infection, or any other type of infection.
It is not the first paper to propose that the vaccinations reprogram the immune system, to what degree is anybody guess so far, yet the one most “close to home”, because of the importance of mitochondrial function.
I will try my best when I delve deeper into this subject to make it clearer (since it is intimately linked to all the damage, short and long term Covid does), but for now, it will do.
Both the virus using other mechanisms and the vaccine using another are wreaking havoc in your bioenergetic state, some people sometimes end up functioning at half-voltage, in a crude simplifaction. Even when we function at normal levels, our bodies can have a hard time dealing with the healing process, and mitochondria will dictate much of your whole physiology.
Chronic infections, which do exist, will not only affect viral evolution, and bring forth nastier variants, but they also play a big role in how, and why the virus behaves as it does, and the specific damage certain people claim it does (using all the wrong evidence and not demonstrating any of the pathways, even wrong ones). Long-lasting infections are important to understand because I fear we will experience a growing number of those as the months go by.
You should keep in mind the nonstructural proteins of SARS-CoV-2, they will be fairly important soon enough and explain quite a few numbers of the mysteries of the virus in relation to all the weird immune responses we had so far.
This paper is also amazing and people should be aware of it. https://www.biorxiv.org/content/10.1101/2022.06.27.497883v1 - The Staphylococcus aureus iron-regulated surface determinant A (IsdA) increases SARS CoV-2 replication by modulating JAK-STAT signaling
"Using chemical inhibition, we determined S. aureus IsdA modifies host Janus Kinase – Signal Transducer and Activator of Transcription (JAK-STAT) signalling, ultimately leading to increased viral replication"
"Bacterial co-infection is a common and significant complication of respiratory viral infection,
including in patients with COVID-19, and leads to increased morbidity and mortality. The
relationship between virus, bacteria and host is largely unknown, which makes it difficult to
design effective treatment strategies. In the present study we created a model of co-infection
between SARS CoV-2 and Staphylococcus aureus, the most common species identified in
COVID-19 patients with co-infection. We demonstrate that the S. aureus protein IsdA
enhances the replication of SARS CoV-2 in vitro by modulating host cell signal transduction
pathways. The significance of this finding is in identifying a bacterial component that
enhances CoV-2 pathogenesis, which could be a target for the development of co-infection
specific therapy in the future. In addition, this protein can be used as a tool to decipher the
mechanisms by which CoV-2 manipulates the host cell, providing a better understanding of
COVID-19 virulence. "
Of possible interest: SARS Survivors, 10 yrs later
https://globalnews.ca/news/404562/sars-10-years-later-how-are-survivors-faring-now/