


SARS-CoV-2 causes gastric damage and Galectin-3 deficiency
Long time coming.

A few years ago, as I attempted to uncover all the hidden things in SARS-CoV-2’s Spike Protein, specific parts of the chimeric protein came to mind quite quickly, especially the now-infamous “HIV inserts”. The Furin Cleavage Site is one of them, acting as a multi-functional protein, enabling the virus to bind to ACE2 and infect your cells, acts as a superantigen, it acts like GP120 in regards to how toxic it is to your body, among other effects. A very pernicious effect is that it enables the virus to bind to Endotoxin, catapulting its inflammatory prowess.
Another “insert” wasn’t exactly an insert, it is a naturally occurring section in certain coronaviruses. It’s N-Terminal Domain (NTD), or otherwise called “The Galectin-fold”, because it is a perfect mimic of human Galectin, specifically Galectin-3. The article below has an overview of what Galectin is, with an intense focus on 3.
In the context of the virus, the NTD is what immunology calls a “super antigenic site”, meaning your immune system is highly sensitive towards that specific part of the virus, and it will seek it like a highly sophisticated missile. Mutations in this region enable the virus to escape the immune system and your antibodies, and it also enables the virus to change how sugars coat itself, enabling it to further escape immune responses.

While being distinct classes of proteins, if HMGB1 is the One Ring of proteins, Galectin-3 is a literal chimera, a promiscuous protein (meaning it interacts with things that it shouldn’t), able to interact with almost as many other proteins as HMGB1, and it is able to interact with the One Ring itself.
These sugar-binding proteins are critical to regulating numerous processes, but 3 is especially important for its propensity to interact with “anything”, and it is a critical immunoregulatory protein. It acts on all three stages of inflammation, it can start, it can mediate (change the inflammatory process and response), and lastly, potentiate, increasing the entire thing. Gal-3 is incredibly sensitive to higher amounts of glucose, the more sugar one has in their bloodstream and body, the higher the expression of Gal-3, making it a nasty contributor to long-term disease.
As I often mention, too much of anything is bad for you, and our bodies, while incredibly resilient, are prone to paradoxical responses that, from the surface, look harmful, but they are often compensatory. The infamous short-term gains, long-term pains. Given how similar in every aspect (amino acid and shape) the NTD is to human Galectin-3, I stated that at some point, in some people, the body would produce significantly less Gal-3, which is a problem on its own… From this article.
If, for whatever reason, your body is “forced” to produce large amounts of Galectin-3 in response to cellular signaling, infection, or damage, it will produce much less of it soon after in an attempt to reach equilibrium.
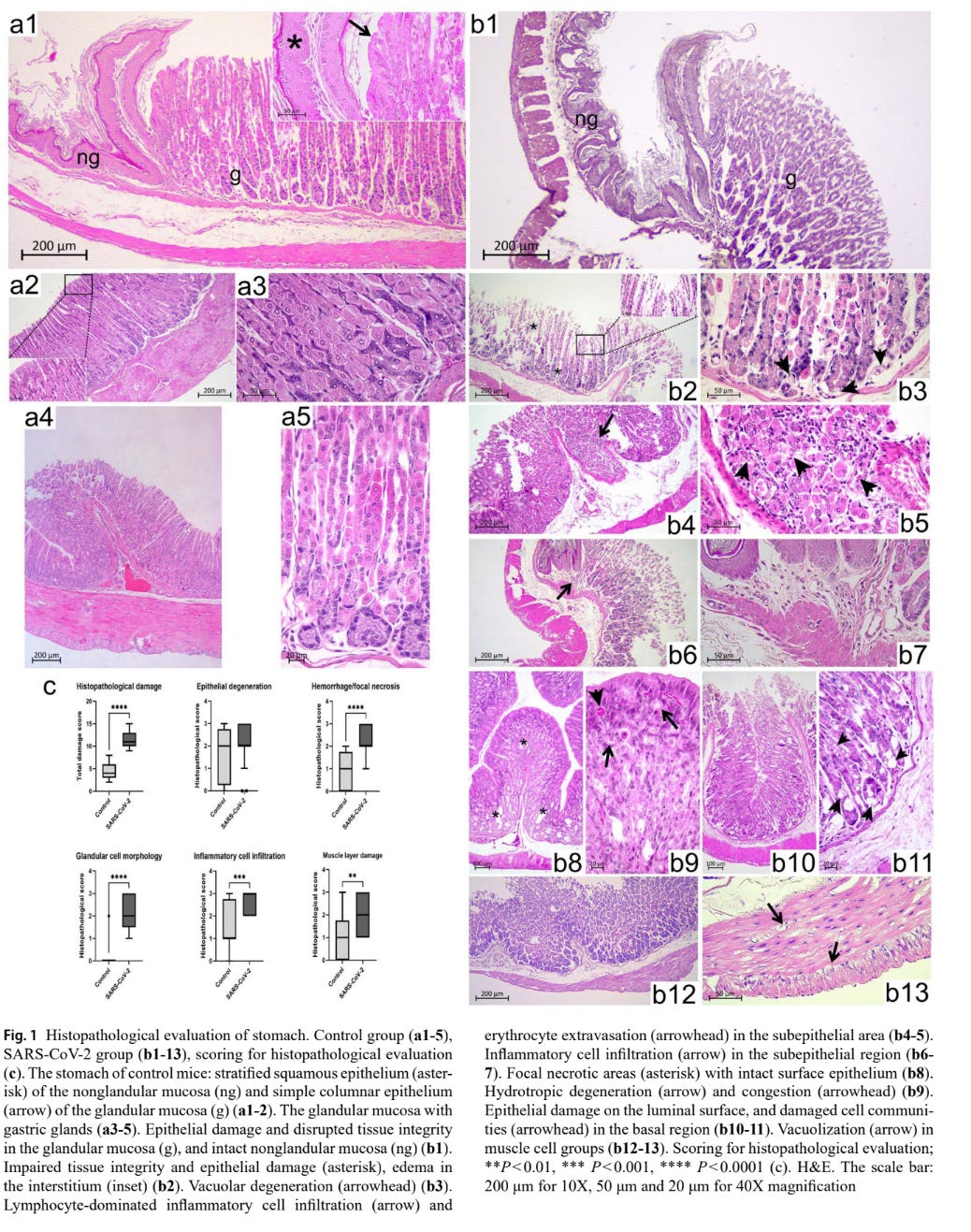
SARS-CoV-2 causes gastric damage: structural and ultrastructural evaluation
As a long-time sufferer of gastric disease, now drastically improved and much better and under control, another one of my focuses in regards to SARS-CoV-2 has been the gut, after all, the more you learn about human biology and immunology, the more the old saying becomes solidified truth. Everything begins in the gut.
The gut-brain and thus nervous system axis is among the most important axes for long-term health outcomes, contributing to either health or pathology. Even before the pandemic became a pandemic, gut symptoms and severe gut issues were observed in Wuhan, Alpha, and especially Delta variant patients, as the gut is rich in ACE2.
Many papers have tried to provide evidence that SARS-CoV-2 not only damages but also infects the cells, and progressively damages the tissue, causing a host of issues, given that many Long Covid patients and patients who experience severe infection have “leaky gut” problems, with a large number not having any gastrointestinal disease prior to Covid.
The mice were infected with Alpha, arguably the second most nocive strain to the gut, behind only Delta (in my opinion, prior to the recent Omicron strains), isolated from a patient, which to me would make it something different than Alpha, but I digress. In case you are wondering, in the process of infection, the virus changes, and in the process of isolating and replicating in a lab, it also adapts to this process, we could say it is Alpha 1.2.
In the SARS-CoV-2 infected group, significant damage and compromised gut integrity were observed, in the lining responsible to secreting mucus which protects your gut. The cells responsible for this process were impaired, misshapen, and the tissue itself was swollen, these cells are the cells responsible for producing acid and digestive enzymes, directly impacting digestion and especially nutrient absorption.
Infiltration of lymphocytes and leaking of Red Blood Cells into the tissue was also observed with signs of congestion. The muscle cells themselves showed signs of damage. What all of this means in layman terms ?
The part of the stomach that works the most is severely damage, its integrity compromised, which creates a cascade of problems, as the damaged and dying cells spread their content around, thus spreading inflamamtion and leading to further damage. This also allows bacterial toxins to flow out of the stomach, the cells are no longer healthy.
Lymphocyte infiltration leads, meaning moving from elsewhere towards a place they shouldn’t be, leads to this cycle of damage as they move to fight the virus, in this process, they release inflammatory proteins that cause collateral damage, leading to damage to the blood vessels, thus the Red Blood Cells leaking into the tissue. Damage to the muscle cells affect gut motility, delayed motility is resposible for that feeling of being too full after eating little, nausea and other gastric issues.
Loss of mucin means the protective barrier is just gone, this leads to increased inflammation and damage from the stomach’s own acid, which in turn makes the whole process of the viral infection worse. These alterations make an individual susceptible to secondary infection. In theory, this could help explain the sudden explosion of norovirus and enterovirus, especially seasonal spikes closely following SARS-CoV-2 infection spikes.
The researchers also observed that the virus has a preference towards infecting areas where the gut is more sensitive to damage, avoiding the thicker, more resilient region.
This level of damage is often preceded or accompanied by cell death, and that is what the authors measure, 3 forms of cell death, apoptosis, pyroptosis, and necroptosis, followed by measuring Galectin-3, which can regulate cell death in a context-dependent manner.
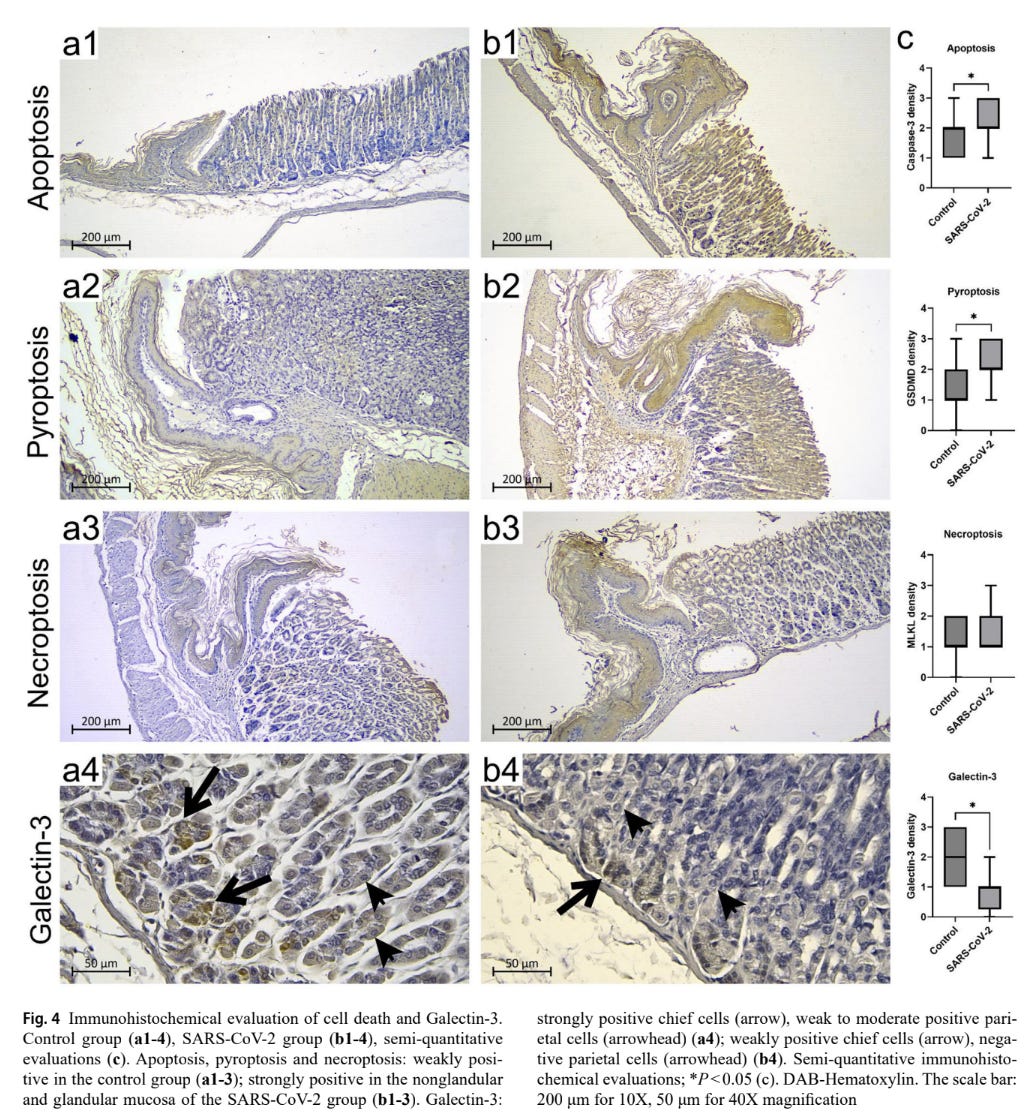
As we covered recently, SARS-CoV-2 can induce necroptosis and thus necrosis via multiple mechanisms, as a direct effect of its infection, but also as a byproduct of the damage and the body's responses because of the infection. In this study necroptosis wasn’t as present as in other studies, which is normal, there is significant variance between research and even individuals.
Apoptosis, “normal cell death”, was more abundant, and it can be induced by the process of infection or by stimulation of receptors related to cell death, it can also occur as a regerative responses, cleaning dead cells, so new ones grow and tissue regenerates.
Pyroptosis was also substantial, and this is a form of cell death that is incredibly damaging, because it is highly inflammatory, and SARS-CoV-2 has almost a literal dozen ways of inducing this napalm-esque form of cell death. The parietal cells, the cells that produce stomach acid, were the ones most affected by pyroptosis.
Lastly, the authors measured Galectin-3, which they found to be deficient.
What is the importance of all of this ?
This section is purely my own thoughts, outside the scope of the author’s research and words. This paper provides significant primary evidence towards profound lasting effects of the viral infection. First, it gives us a glimpse of why so many people experience varying digestive symptoms, sometimes for months after SARS-CoV-2 infection.
It also provides initial assessment on poor vitamin absorption, especially present in severe and Long Covid cases, where supplementation with certain B vitamins (especially 12) has little effect, this is because they lack the necessary digestive enzymes and factors to properly metabolize it. This can be bypassed by infections.
Secondly, the physical damage seen here, allied with the changes in the cells and capacity of the gut to produce its protective coating and even acid, affects the entire gut immune health. It leaves one open to secondary infections, and your gut becomes leaky, which enables toxins to go elsewhere, and in a worst-case scenario, pathogens, too.
Not only this, but these changes can also allow the virus or its fragments to persist for months, because your tissue is damaged, the virus and its fragments are embedded into cells and tissue, and the body is unable to properly clean itself, thus creating an environment of low-grade but lasting inflammation.
But the most remarkable find here was the lower levels of Galectin-3. There may exist a few reasons why the body producing less Gal-3 during and after the viral infection. The first reason, as presented earlier in this article, is the fact that SARS-CoV-2 has a perfect mimic of Gal-3, thus, the body may interpret this as excess Gal-3.
The second hypothesis is another direct effect of the infection. Given the extensive damage observed here, the body may increase production within a short period and severely downregulate Gal-3 production. A longer study could provide insight into this, but also into the third hypothesis.
SARS-CoV-2 directly interacts with gut microbes and bacteria, and half of the reason it can act as an Endotoxin delivery system is the NTD (the other half is the Furin Cleavage Site) both this interacts, and the Spike carrying endotoxin inside cells, starting a signaling cascade which would force the body to produce less Gal-3.
Even if the lower production of Gal-3 is transient, lasting only briefly, can cause problems, given the drastic changes observed here, it is clear it leaves the gut open for secondary infections, and Gal-3 is one of the most important mediators of cellular metabolism and immune defense. Lack of it can both increase and decrease fungal infection (how many Long Covid patients are developing fungal issues right about now ?).
Gal-3 is crucial for tissue regeneration, it helps recruit cells to clean damaged tissue, so the body can heal, and also avoid fibrosis (the formation of scar tissue, a big problem in any organ). Without Gal-3, the process is severely diminished, and this can lead to long-term gastrointestinal issues.
The observations in this paper provide evidence for why so many Covid patients experience lasting neurological symptoms, especially related to mood and psychological disorders, given that the serotonin factory of the body is directly damaged, the inflammation further starves the body of proper tryptophan supply, and creates a feedback loop.
Whenever you have significant damage, inflammation or dysfunction (or excess sugar), you have Galectin-3, and whenever you have one, you have the other. Its sister, Galectin-9.
Spike Protein induces intestinal barrier dysfunction via Galectin-9

This article was supposed to be published yesterday but I got lost writing a short story lol.
I could write two, three closing paragraphs, and I did, but I decided to delete them. There is a more prescient, forecasting-inclined closing remark that does the job with greater accuracy and more poignantly.
In 1961, the Seventh Cholera Pandemic started. And we are still living in it.
If you are a supporter, thank you very much. If you are not, consider becoming one.
Another week, another forecast being accurate. It brings me no satisfaction being either right or ahead anymore. Awareness of how damaging all of this is can be soul-sucking.
I wish all of you a great week ahead anyway. New article sometime later this week.
Since 2020, I have seen, by far, the most severe B12 deficiencies I have encountered in my career (my own family members included). I suspected parietal cells were being decimated by covid and had been explaining that as the probable cause since none of these individuals had a history of b12 deficiency. Thank you for sharing the mechanism! One more covid mystery solved!