


SARS-CoV-2 - Antibody Dependent “Enhancement”
More like inflammation really….

We now have real evidence for a specific form of Antibody-Dependent “Enhancement”.
I usually resize the images, but given the text in the paper, I will leave the images as they were uploaded by Substack.
FcγR-mediated SARS-CoV-2 infection of monocytes activates inflammation
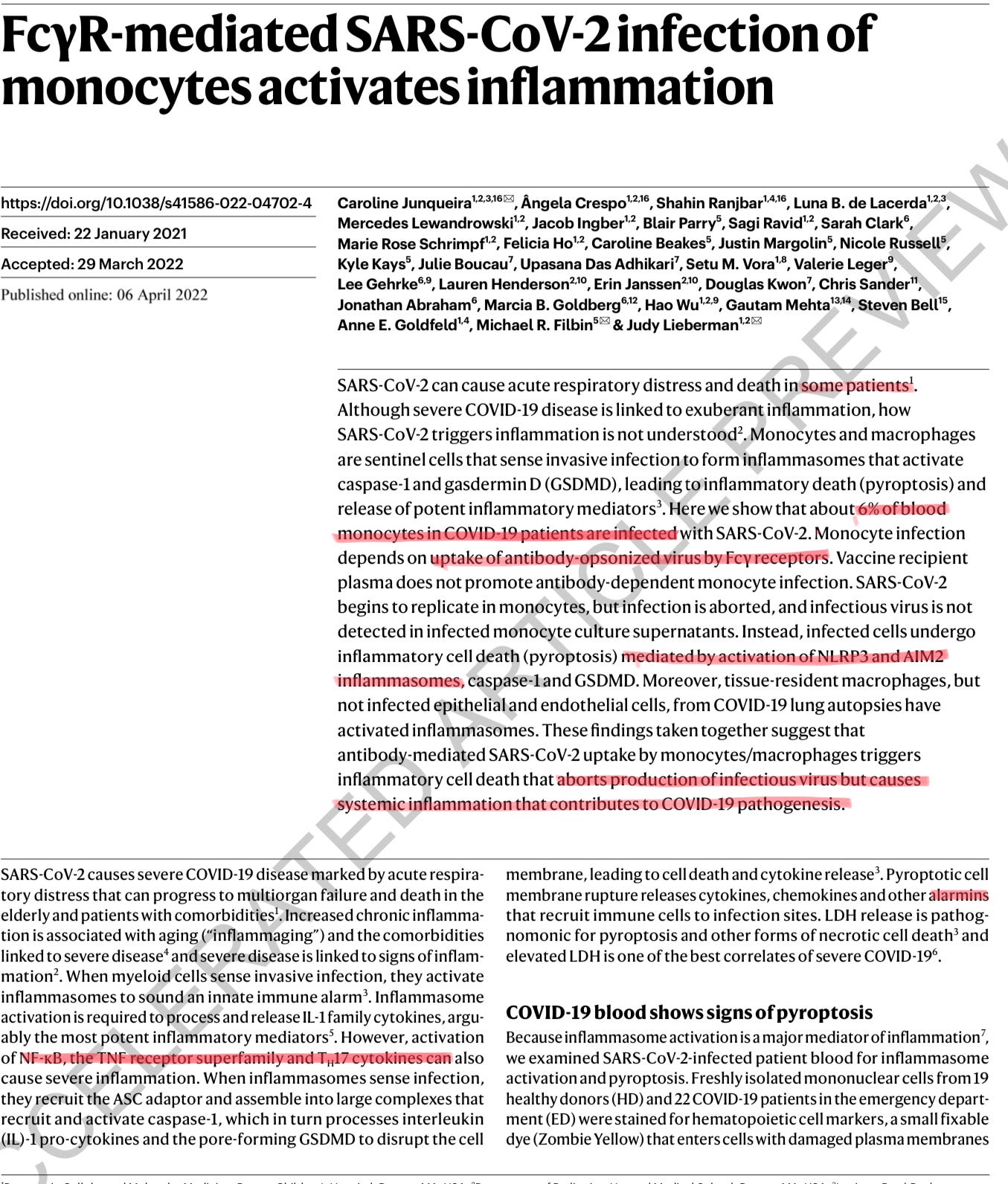
This paper is rather complex and has a lot to unpack. The authors sought to discover how SARS-CoV-2 triggers inflammation. Here they found that 6% of the blood monocytes were infected. This is dependent on “antibody opsonizing by Fc gamma receptor”. Opsonizing is a term used to describe covering a pathogen in antibodies, so it can go to phagocytosis (meaning a specific cell eating that pathogen/infected cell).
The red part is the other pathway of the disease (and vaccines), that I already covered extensively.
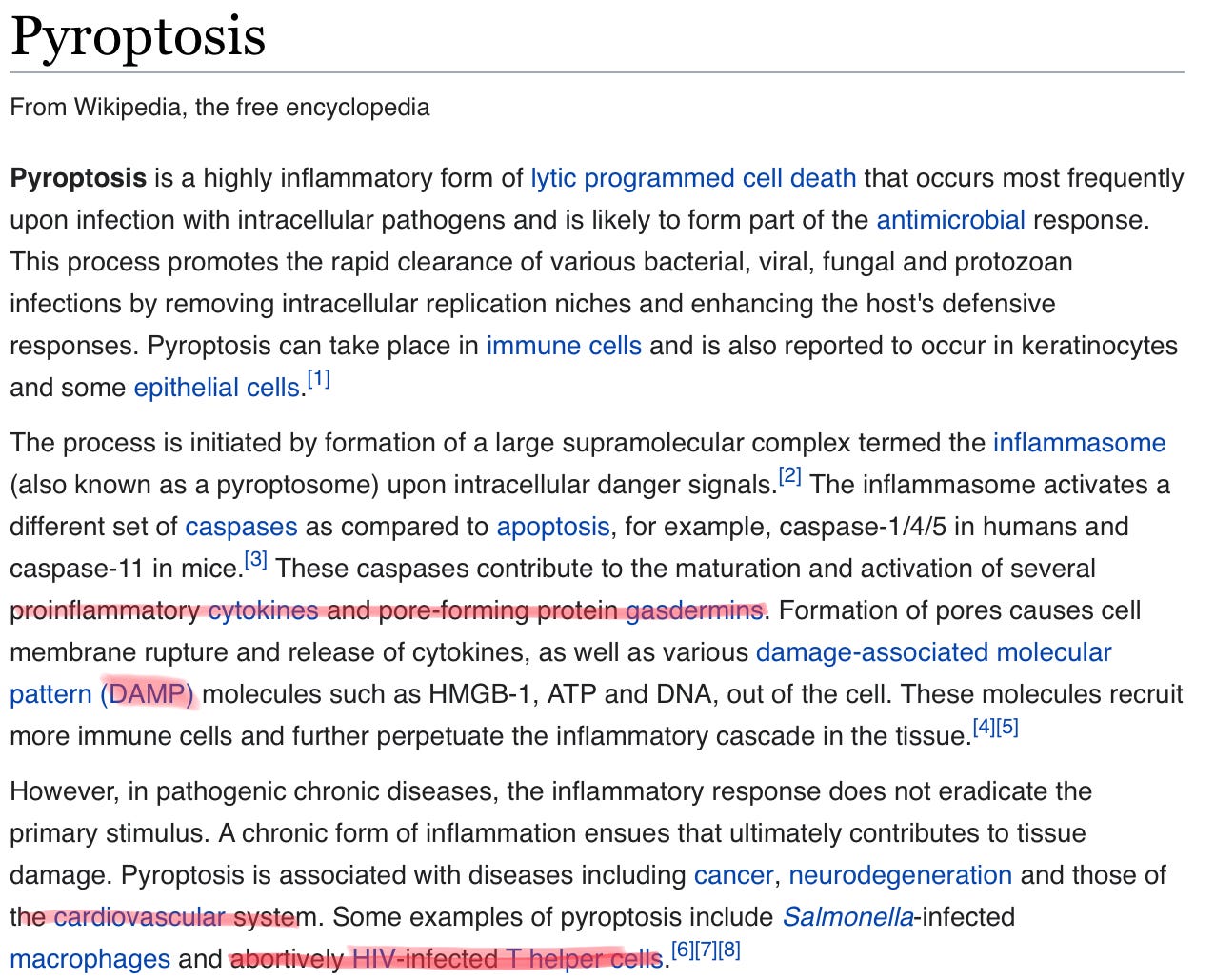
The abstract is self-explanatory, monocytes do not enable viral replication, but die via pyroptosis, and contribute to a massive inflammatory response. What is pyroptosis :
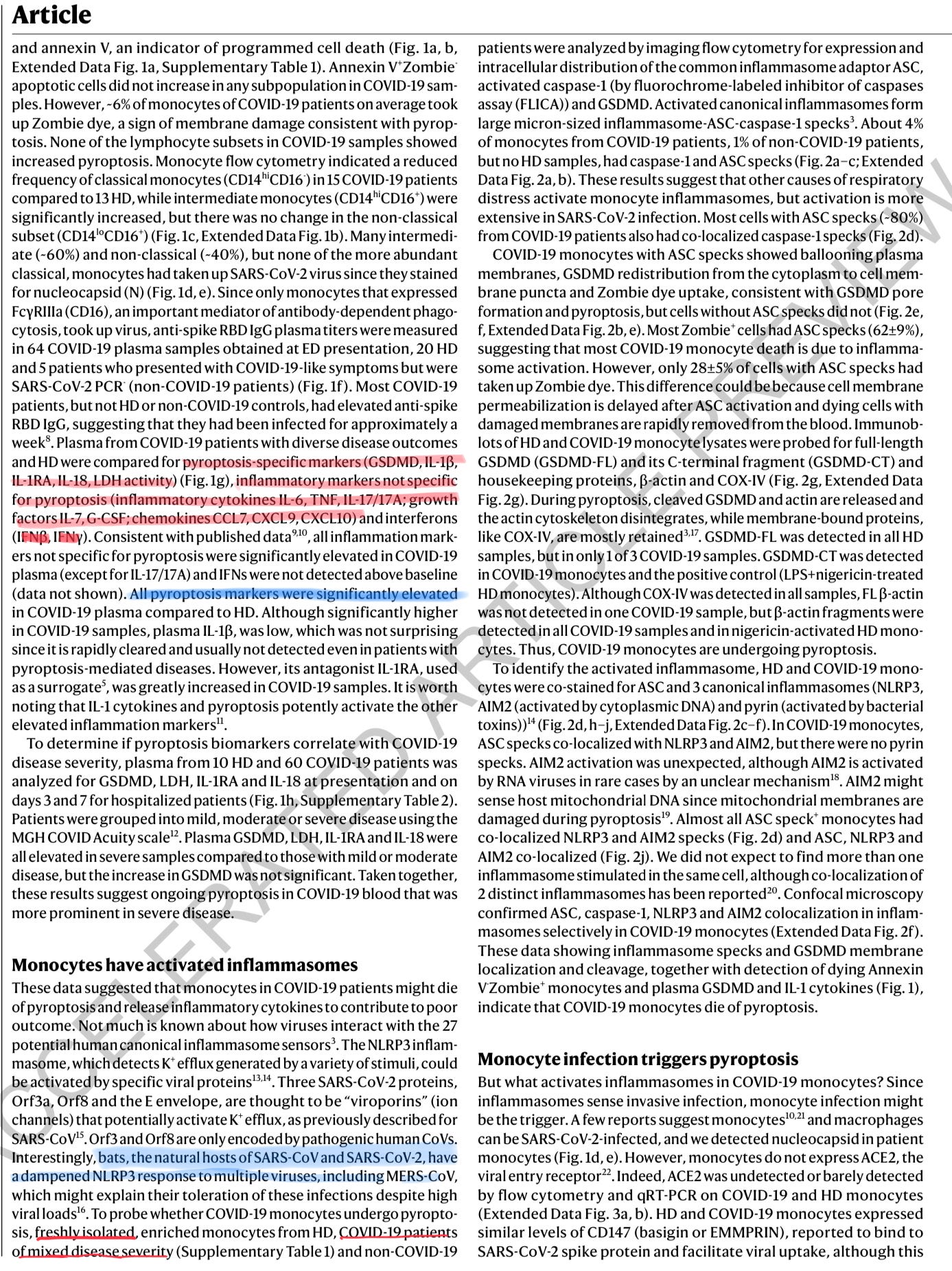
This paper has a lot to unpack. First things first, as I said a couple of times here, and multiple on Twitter, the design of papers matters, and details matter. The red underlined is exactly that. Most studies are done with frozen cells, cell lines, etc. This one was done on freshly isolated monocytes. It makes a huge difference, and they mixed disease stages.
It is my opinion given the current evidence, and my own observations that the fate of the cells SARS-CoV-2 enters, and hijacks are solely dependent on the receptor it used, as per the other macrophages papers I shared previously.
The measured specific markers for pyroptosis, being GSDMD, Interleukin 1-Beta, Interleukin 1RA, Interleukin 18, and LDH (lactate dehydrogenase) activity, and found they were significantly elevated.
LDH is an interesting pathway to go down because it is directly linked with glycolysis, ATP, and…mitochondria.
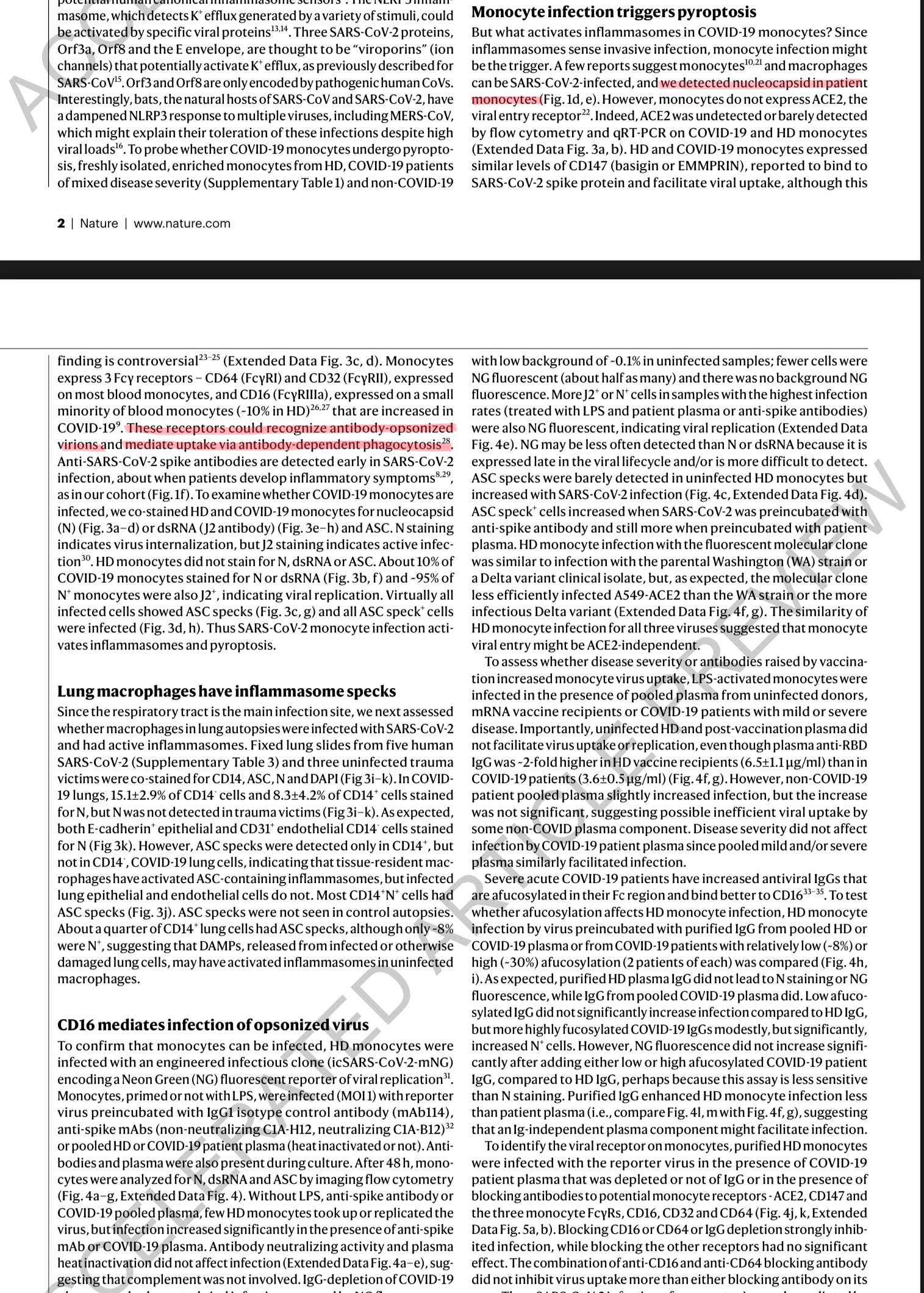
To confirm that the virus was inside the monocytes, the authors tested and found the N protein in them. They went to find which specific Fc gamma receptors were used. As I side note, this paper on B cells Antibody-dependent enhancement (ADE) of SARS-CoV-2 pseudoviral infection requires FcγRIIB and virus-antibody complex with bivalent interaction, Had a similar finding uncovering that the virus will use one of the Fc receptors and inflict ADE.
The authors described the pathway and mechanism using a different one from the paper above, it uses FcIII, and it needs the virus to be opsonized (covered in antibodies) to “infect” the monocyte, which they proved. The paper is well designed, and I won’t bore you with the details, and it is relatively bad.
One thing I will argue to death, and will mildly criticize the authors, is the “vaccinated plasma” and this mechanism not happening among vaccinated individuals. Perhaps vaccination timing and getting the plasma, perhaps methodology, or at a small chance, a different mechanism, but it is happening disproportionately among vaccinated individuals. It is literally the case I presented in the post below.
Also, laughable that it “prevents infection”.

The paper in question is the “Suboptimal” one, but the entire series, and my proposal stands, and with evidence and time it will prove itself. Perhaps we need a different name for the mechanism the authors found, and the type of antibody enchantment I propose in some vaccinated individuals. Antibody-dependent inflammation ?
They go to find that, similar to other papers I covered, the infection in these cells is “aborted”, meaning, the virus enters the cell, but doesn’t replicate, instead it sets off a small cascade of inflammatory responses after the cell dies (to save itself, they go to describe how it does, basically expressing a protein that makes a bunch of holes from inside the cell).
I said this once and will do it again. The fate of infected cells is decided by the types of receptors used to enter the cells. If it uses the X receptor, it will set off a specific form of cell death, and specific inflammatory signals, if it uses Y, so on, so forth.
I think a proper term for this paper would be Antibody-Dependent “Infection” and not Enhancement. It is a good path forward, but not the main reason I choose to analyze this paper.
Another receptor, other pathways, but the end result is similar. IL-18, you should read the post above to understand where I am going with this one.
And this one.
Even a mild SARS-CoV-2 infection changes the inflammatory response in macrophages (macrophages are “born” from monocytes), changing your immune response towards other pathogens, and Covid itself. To summarize, we now have more evidence that SARS-CoV-2 infects monocytes, and how it sets off a powerful inflammatory cascade, by using receptors of cells covered by antibodies.
After reading the Reverse Marek post, this one, and the ones above, I will leave you with the same question I often ask.
Are breakthrough infections, with non-neutralizing antibodies, really harmless ? Or are we modulating and inflicting a persistent, low inflammatory state upon hundreds of millions, chipping away at their physiology ?
If you are worried, just read Part 3 of my Things Hidden series. It is in the Index post below. Ketones, or to be precise, Beta Hydroxy Butyrate modulates NLRP3 inflammation.
The next Covid post is even better. Yes, better than finding ADE evidence.
You can use Ko-Fi to buy me a coffee whenever you feel like it.
If you enjoy independent, complex, interdisciplinary analysis, and forecasting consider becoming a free or paying subscriber, support is very much appreciated. Sharing also helps me tremendously. Deep appreciation for all the supporters.
I am writing an article right now and I will link to yours, great job.
Regarding your comment on the vaccinated plasma: "One thing I will argue to death, and will mildly criticize the authors, is the “vaccinated plasma” and this mechanism not happening among vaccinated individuals. Perhaps vaccination timing and getting the plasma, perhaps methodology, or at a small chance, a different mechanism, but it is happening disproportionately among vaccinated individuals."
....why would they obfuscate with this statement?
What if this is true? The unvaccinated would be most at risk...right?