


Recovery from Long Covid after 12-months
And other news

Today’s article will still be serious but on a positive note, rather than… whatever note the old one was. It will be concise and simpler so anyone can understand too. This first article is for my own amusement.
A few days ago, Phase 1 trial results for a new SARS vaccine were published, but this isn’t your average SARS-CoV-2 vaccine, no. This is cutting-edge, potentially pan-coronavirus vaccine.
Ferritin nanoparticles are the next choice for some researchers for similar reasons to other particles, they are quite potent immunomodulatory, and monophosphoryl Lipid A is just detoxified LPS (Endotoxin), which already raised my eyebrow. Reading through the paper, something catches the eye of the attentive reader. “High CD4+ cells”.
I have heard this one before, in fact, I have heard this one multiple times since 2021. From the graph that started all of this.
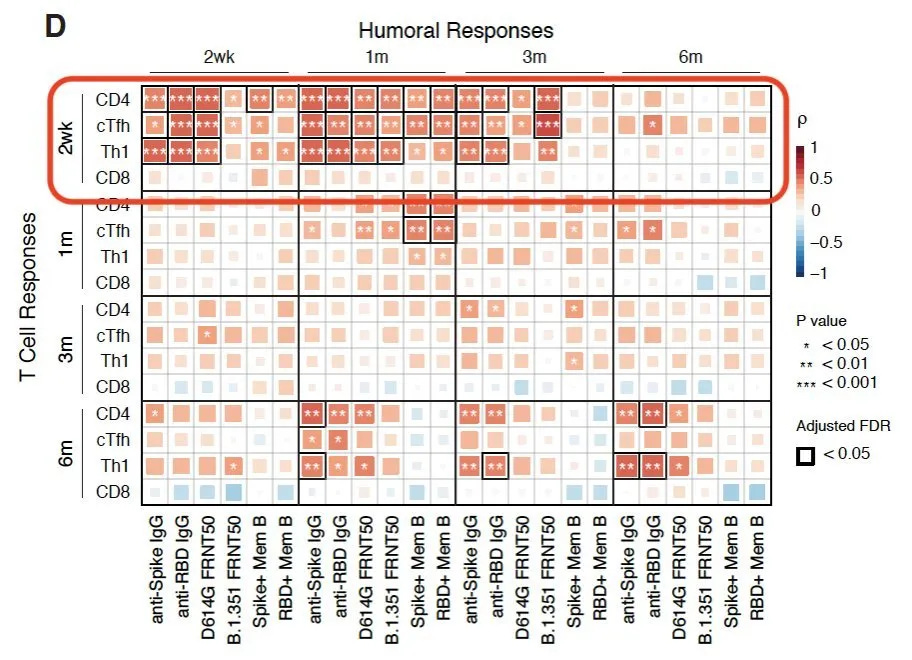
Whenever you read “We detected high CD4+ cells”, your next step is to look for if the author mentioned or measured CD8.
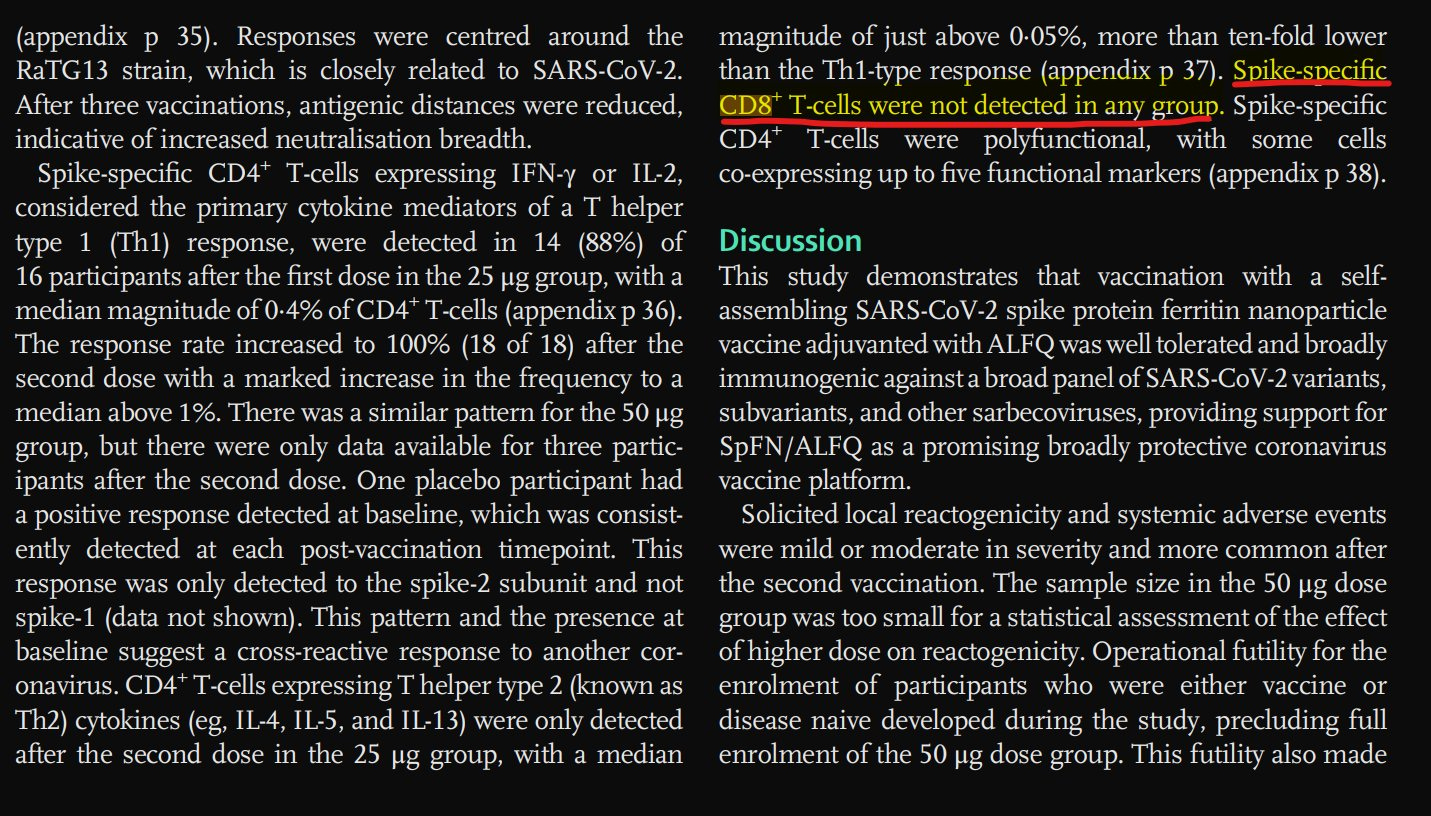
Well, color me NOT surprised. A potentially pan-coronavirus vaccine, that produces almost no CD8+ T-cells. This is important because CD8+ T-Cells are the ones you need to properly neutralize the virus, this is repeating the same (mRNA) mistakes.
My only posthumous correction would be “death sentence after lots of jabs” at this point. More like a slow crawl to immunological death, given all the evidence. Otherwise, everything stands. A lack of proper, mucosal CD8+ response is exactly what got us here, it is exactly why the immunological dysfunction in unvaccinated, vaccinated, infected, and reinfected gets so complex. No CD8+ will provide you short-term protection even if neutralizing. We are entirely into testing things to gather data to feed Machine Learning leviathans anyway… To the next one.
One of my biggest points of contention in 2021 was the “Amyloid” trend. Amyloid this, amyloid that, and I persisted in correcting some people for a while on how that is not how amyloids work, it wouldn’t be how amyloids in SARS-CoV-2 work.
Whenever you truly talk about misfolded proteins and the role of their different morphologies (their shape), it tends to get extremely complicated, very fast, which makes very difficult for a layperson to understand, and misinterpretations are frequent even among people with knowledge in the subject. The paper can be found here, I will summarize everything below the image.
The authors have been hard at work on uncovering the complexity of amyloid and SARS-CoV-2 amyloidogenic peptides, meaning very small fragments of the virus that can induce the creation of amyloid, and uncovering how these small fragments do this is key to understanding and remediating.
Here they still use two of the previously mentioned (both here and in their research) ORF6 (ILLIIM) and ORF10 (RNYIAQVD). They dissolved the peptides before diluting them into phosphate-buffered saline (PBS), the researchers ensured the removal of insoluble seeds that typically promote amyloid formation. This approach allowed them to observe the spontaneous assembly behavior of the peptides, leading to the formation of various polymorphic structures, including oligomers, fibrils, and crystals.
Without pre-existing “seeds”, the peptides tend to form higher energy, less stable assemblies. ILL fragments result in fewer crystals and more fibrils, RNY fragments have more oligomers and fewer crystals and fibrils. Seeds are exactly what they sound, a protein that will act as a seed for further growth, in this case aggregation, of more of the “bad” proteins. A reminder that HERVs are one of the primary seeds for misfolded proteins.
Why is the state of the amyloid formation important ? Because it influences both how “dissolvable” and toxic that state of amyloid is. Given enough time amyloid proteins tend to want to reach a global energy minimum, a state of the least amount of energy possible, which is the crystallized form. All forms of amyloid can be toxic to your cells, oligomers (clumps), fibrils (fibers that interact with other “stuff”, and also can “glue” with other fibrils and form plaques), and finally crystals.
Here the authors found that the oligomers were the most toxic form, capable of interacting with many cellular components and inducing cytotoxic effects (a hallmark of the “bad amyloid”).
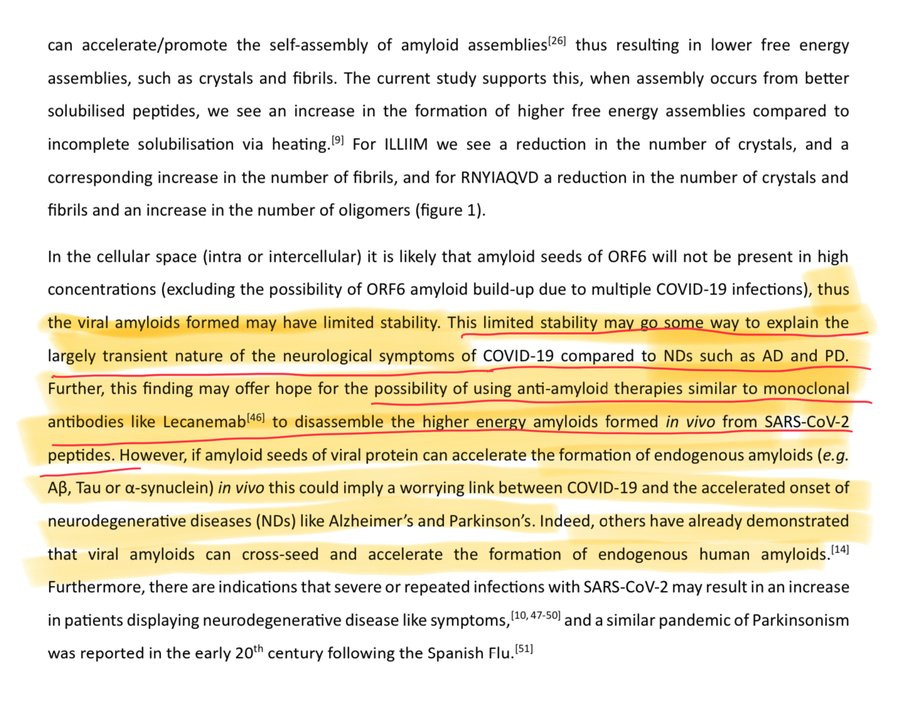
And here we will see a recurring (coming) trend, in vivo (meaning inside a person) there is limited presence of amyloid seeds inside or outside cells for the most part, and this indicates that the viral amyloids forming during SARS-CoV-2 infection may not reach the necessary stability to induce chronic (lasting) neurodegenerative states. This can explain why most of the neurological symptoms observed in Covid infection are transient.
This leads to a couple of my misfolded proteins article, in which I argued that the problem is not accumulation of bad proteins in and by itself, which can be, but clearance. The entire body of evidence points out towards not “dissolving” the bad proteins fast enough, leading to their accumulation and thus the infamous effects. In their high energy state here, they are “easier” to dissolve, therefore many forms of intervention can be done to help the body clean itself.
Of course, this doesn’t exclude the fact that these proteins can interact with all other proteins that can go bad such as Tau, α-synuclein. But I will stick to my assessment it can be remediated if taken care of early enough. Since we mention about Alpha-Synuclein, more good news, in a way.
This research is incredibly important but to be abundantly clear so the more anxious don’t jump to conclusions, here they injected 0.5 grams, at once, of S1 intranasally in male rates. First, the dosage is incredibly high, as usual per studies like this, you need a very high dosage to mimic a severe/ICU infection, and second, intranasally means almost direct into the brain given the dosage, bypassing many of the body defenses, even in mice. By injecting S1 intracerebral the authors observed typical aggregation of a-Syn and brain inflammation, so the next step is understanding how S1 causes aggreagation of a-Syn in vitro.
In their in vitro studies, the authors exposed BE(2)-M17 dopaminergic neurons, which are a type of nerve cell susceptible to Parkinson's disease, to the S1 protein. They observed a marked increase in α-synuclein aggregation, which was further intensified when these neurons were co-cultured with BV-2 microglial cells, a type of immune cell in the brain. This thus led to an increase in inflammatory protein, converting the microglial cells into a pro-inflammatory type, and this inflammation triggered by S1 increases the aggregation of a-Syn.
Interestingly treating the M17 dopaminergic neurons with S1, only one form of a-Syn, called p-α-Syn (Ser129) was increased by S1, meaning that S1 alone can induce aggreagation but only if sufficient a-Syn is accumulated. One of the main aspects of a-Syn diseases is mitochondrial damage and mitochondrial dysfunction.
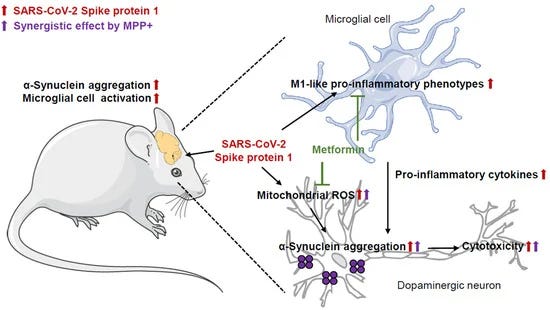
As covered in this publication multiple times and argued by my mentor-friend and I, this is a bioenergetic disease, and all the evidence so far points out that mitochondrial dysfunction is one the biggest contributors. Replicating the findings of other groups here the authors observed that S1 increases mitochondrial ROS and thus causes mitochondrial damage. Both effects (mitochondrial damage and a-Syn aggregation) were mitigated by using a mitochondria-specific ROS scavenger called MitoTempo.
Next, they tested if S1 could achieve any effect with a neurotoxin used in Parkinson’s Disease models called MPP+, and yes, S1 + MPP+ significantly increased a-Syn aggregation and mitochondrial ROS production. And here is something that is often overlooked, especially in in-vitro models.
It should be tested how the Spike Protein reacts and binds to other toxins, besides Endotoxin. One example, and purely theoretical, MPP+ is positively charged and Endotoxin is negatively charged, could both form toxic aggregates ? This would affect many in-vitro or even in-vivo tests because you are enhancing the effects of the Spike Protein. I came to learn in the past few months that Endotoxin is somewhat of a promiscuous toxin, it can bind to other toxins and turbocharge their effects.

Given recent trials on the positive effects of Metformin on treating Long Covid, and the somewhat extensive list of positive effects Metformin has on misfolded proteins and neuroinflammation the authors tested if Metformin had a positive effect in their disease model. And yes it did, metformin attenuates the effects of S1 and its synergy with MPP+ and its aggregator effect on a-Syn. Metformin ameliorated the S1-induced M1-like phenotype (TNF-α, IL-1β, and Iba-1), while CD163 levels remained unchanged, in simple terms Metformin lowered the inflammation here.
It is one of the reasons a few random netizens find my suggestions, to get a prescription for Metformin and add antioxidants (mimicking the Mito treatment in this paper) and experience a sudden improvement in their symptoms. Metformin is getting a lot of good rep among clinicians and Long Covid patients, so if you have long-term sequelae from the virus you now can easily get a prescription. Remember to add all Vitamin B complex, daily if you take metformin.
I plan to get back to both of the following papers later on because they are full of insights that can give us answers but the focus here, today, is recovery.
Improvement of immune dysregulation in individuals with long COVID at 24-months following SARS-CoV-2 infection
This study investigates the humoral and cellular immune responses and health-related quality of life measures in individuals with mild to moderate long COVID (LC) compared to age and gender matched recovered COVID-19 controls (MC) over 24 months. LC participants show elevated nucleocapsid IgG levels at 3 months, and higher neutralizing capacity up to 8 months post-infection. Increased spike-specific and nucleocapsid-specific CD4+ T cells, PD-1, and TIM-3 expression on CD4+ and CD8+ T cells were observed at 3 and 8 months, but these differences do not persist at 24 months. Some LC participants had detectable IFN-γ and IFN-β, that was attributed to reinfection and antigen re-exposure. Single-cell RNA sequencing at the 24 month timepoint shows similar immune cell proportions and reconstitution of naïve T and B cell subsets in LC and MC. No significant differences in exhaustion scores or antigen-specific T cell clones are observed. These findings suggest resolution of immune activation in LC and return to comparable immune responses between LC and MC over time. Improvement in self-reported health-related quality of life at 24 months was also evident in the majority of LC (62%). PTX3, CRP levels and platelet count are associated with improvements in health-related quality of life.
This paper focuses solely on the immunological aspect of Long Covid and its related impacts on quality of life, and here we see my disagreements with how “science” measures “exhaustion” but I digress. The immunological dysfunction in Long Covid could be measured and was different between them and the control at two-time points, 4 and 8 months.
PD-1 and TIM-3 expression on both CD4+ and CD8+ T cell subsets were elevated in LC participants at 3- and 8-, but not at 24-months. This resolution of inhibitory markers was also seen when assessed at transcriptomic level by the exhaustion scores in CD4+ and CD8+ T cells at 24-months.
However, the majority of the LC patients in this study recovered their immunological function and achieved a significant increase in their quality of life at the 24-month mark. It is interesting that some of the patients had no changes in their B-cell frequencies but exhibited high antibody levels, which indicates that may there be persistent viral antigen/fragments in tissues, adding to the body of evidence towards this mechanism.
Recovery of neurophysiological measures in post-COVID fatigue: a 12-month longitudinal follow-up study
One of the major consequences of the COVID-19 pandemic has been the significant incidence of persistent fatigue following resolution of an acute infection (i.e. post-COVID fatigue). We have shown previously that, in comparison to healthy controls, those suffering from post-COVID fatigue exhibit changes in muscle physiology, cortical circuitry, and autonomic function. Whether these changes preceded infection, potentially predisposing people to developing post-COVID fatigue, or whether the changes were a consequence of infection was unclear. Here we present results of a 12-month longitudinal study of 18 participants from the same cohort of post-COVID fatigue sufferers to investigate these correlates of fatigue over time. We report improvements in self-perception of the impact of fatigue via questionnaires, as well as significant improvements in objective measures of peripheral muscle fatigue and autonomic function, bringing them closer to healthy controls. Additionally, we found reductions in muscle twitch tension rise times, becoming faster than controls, suggesting that the improvement in muscle fatigability might be due to a process of adaptation rather than simply a return to baseline function.
Another side of Long Covid is the scientifically observable impact it has on muscle tissue as covered here recently. The fatigue is not merely cellular, but somewhat structural, and here similar to what was observed in the immunological dysfunction paper above, the authors observed an improvement in many measurements at the 12-month mark.
Oxygen transport, muscle aches, and fatiguability all improved at 12 months. And here the authors also bring to attention that these long-lasting changes are most likely mediated by mitochondrial dysfunction, rather than other mechanisms, that is most likely secondary here. And the muscle recovery and improvement is most likely adaptation to the deep changes the virus and its deluge of inflammation brought, rather than recovery.
This is why I suggest many people with Long Covid, or any form of viral after-effect (that can be short-lived damage but with lasting effects) to supplement because it will speed up recovery and help the body either heal or adapt. Anyone with LC has to consider supplementation as a long-term deal, and most likely depending on the type of LC you developed, you may as well need to accept (like me) that you will need to supplement certain nutrients for the rest of your life.
For clarification I don’t mean taking a dozen pills each part of the day, morning, lunch, noon, but a few, because some of the changes may be ever-lasting, and you don’t want to crash at year 3, or 5. At least so far, given what I know, this seems the most beneficial and safe strategy.
On a personal level, I am not saying your life will be a field of flowers, sunshine, and rainbows, depending where some find themselves in the path of recovery, it will suck. Sometimes it can be miserable, so you should definitely read from whatever your preferred source, on how to build resilience, I am a very good of mind over body. I don’t expect everyone to learn how to love being miserable, but you should learn how to use discomfort and a little pain as fuel and motivation.
I know how miserable life is when your brain and muscles are so inflammated, that you do one exercise, crash, and spend 5 weeks bedridden. There is a way out, just takes time, some testing, and resilience/perseverance. I hope this article helps or brings some positivity to some of my readers who may need it right now.
Your support is both appreciated and welcome. If you supported me at any point, thank you !

I intend to write an essay on Cyberpunk 2077 and how close to our reality it is, so I highly advise you to either play the game or watch "lore" videos on YouTube, otherwise it will be spoiler heavy.
And yes, it is an experience that is worth the time investment, otherwise "lore videos" are your next best bet. Just go on YouTube and search for the keywords "Cyberpunk 2077 lore" and you will get 1 to 3 hours long video recommendations. Or read the essay which will be spoiler heavy (even for people who played the game).
In the regard you described in this essay, is Berberine analogous to Metformin? Great essay. Thank you.