


Promising Alzheimer’s therapy and related drugs shrink brains and vitamins fix them
Lyme brain changes are real !!!

I plan to bring to your attention certain articles or papers that don’t fit the overall centered themes of most of my posts, I welcome any ideas for the title, there are many things that would be good to share here, but just don’t need an entire substack, and sharing a small piece of news would mean flooding subscribers with notifications and e-mails. These will be at most once per week, or once per 2 weeks.
Coincidentally, all the articles here are mostly related to Alzheirmer’s Disease, with one of them being quite the “good news” and probably memory-holed into oblivion because of the content.
Also in case you missed it, the field of Alzheimer’s research itself has been in a huge “uproar” since one of the leading researchers has been ousted for faking a lot of the findings, a major problem because the paper itself was high-impact, meaning these types of papers have an outsized influence on the entire field. And now “more” news.
Promising Alzheimer’s therapy and related drugs shrink brains
A class of Alzheimer’s drugs that aims to slow cognitive decline, including the antibody lecanemab that was granted accelerated approval in the United States in January, can cause brain shrinkage, researchers report in a new analysis.Although scientists and drug developers have documented this loss of brain volume in clinical trial participants for years, the scientific review, published yesterday in Neurology, is the first to look at data across numerous studies. It also links the brain shrinkage to a better known side effect of the drugs, brain swelling, which often presents without symptoms.
The analysis, which found that trial participants taking these Alzheimer’s drugs often developed more brain shrinkage than when they were on a placebo, alarmed Scott Ayton, a neuroscientist at the Florey Institute of Neuroscience and Mental Health in Melbourne, Australia, who led the work. “We’re talking about the possibility of brain damage” from treatment, says Ayton, who was invited by Eisai to join an advisory board on lecanemab’s rollout in Australia if the drug is approved there. “I find it very peculiar that these data, which are very important, have been completely ignored by the field.”
Some of the treatments for Alzheimer’s (I would personally argue most of the heavily pushed ones) have long-term side effects and are actually harmful, inducing brain damage, and proving little benefit overall. And one of these treatments is Lecanemab.
Anything that ends with mab is a monoclonal antibody, currently the preferred treatment chosen by a lot of doctors, and sometimes the primary care, a massive problem, since I already covered here mAbs literally affected the evolution of some of the most recent Omicron strains, but I wish this was the only problem with mAbs. I have mentioned this once or twice before, but mAb treatment has very serious side effects.
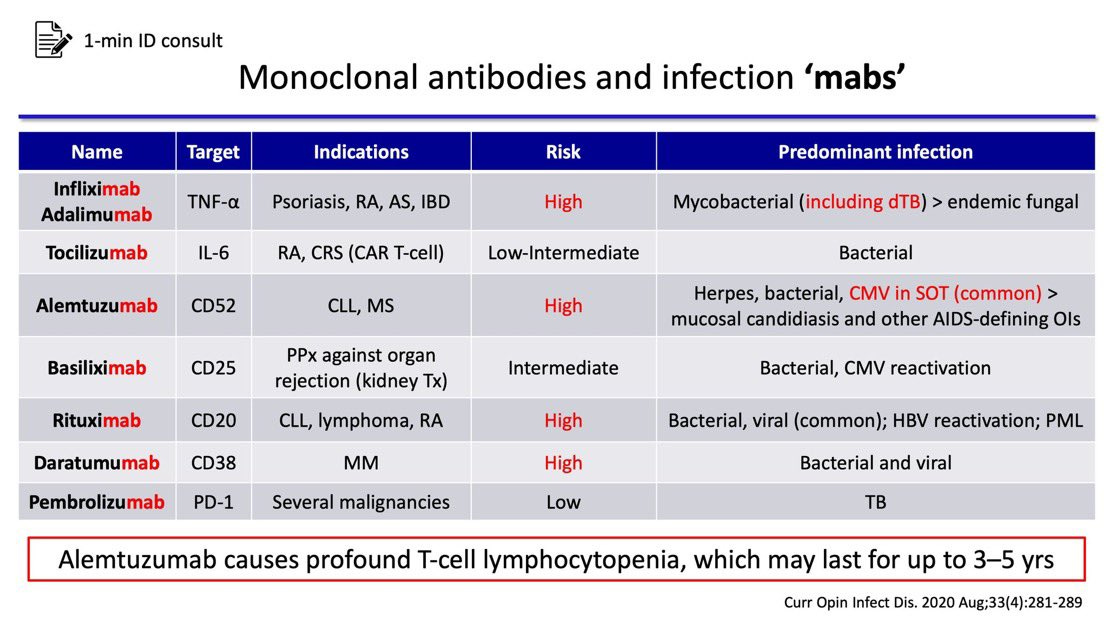
Monoclonal antibodies can have severe long-term consequences, and the incidence of some of their adverse effects are quite high, Rituximab being one that I mentioned in my last substack, widely used to treat many “conditions” and being explored to treat many more, since it is an immunomodulatory treatment it can make the patient susceptible to bacterial infections which on themselves have profound long-term effects.
Bringing this to attention by the fact that mAbs will become the treatment norm in a very short time, antibody treatments are all the rage (arguably the mRNA vaccines used for SARS-CoV-2 are antibody therapeutics with another name).
The second is quite an amazing paper I found today.
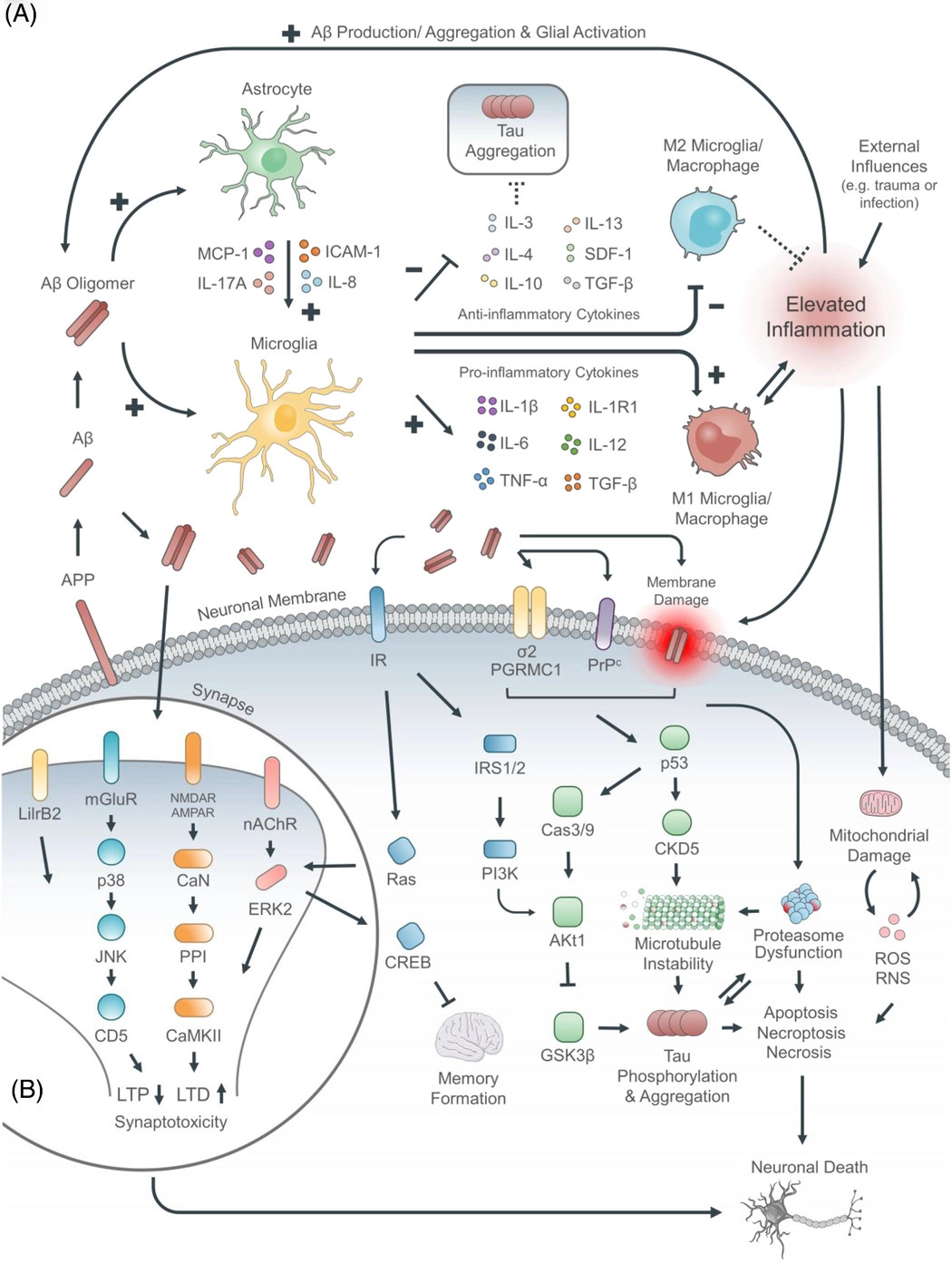
Alzheimer's disease as an autoimmune disorder of innate immunity endogenously modulated by tryptophan metabolites
In response to various stimuli (e.g., infection, trauma, ischemia, air pollution, depression), Aβ is released as an early responder immunopeptide triggering an innate immunity cascade in which Aβ exhibits both immunomodulatory and antimicrobial properties (whether bacteria are present, or not), resulting in a misdirected attack upon “self” neurons, arising from analogous electronegative surface topologies between neurons and bacteria, and rendering them similarly susceptible to membrane-penetrating attack by antimicrobial peptides (AMPs) such as Aβ. After this self-attack, the resulting necrotic (but not apoptotic) neuronal breakdown products diffuse to adjacent neurons eliciting further release of Aβ, leading to a chronic self-perpetuating autoimmune cycle. AD thus emerges as a brain-centric autoimmune disorder of innate immunity. Based upon the hypothesis that autoimmune processes are susceptible to endogenous regulatory processes, a subsequent comprehensive screening program of 1137 small molecules normally present in human brain identified tryptophan metabolism as a regulator of brain innate immunity and a source of potential endogenous anti-AD molecules capable of chemical modification into multi-site therapeutic modulators targeting AD's complex immunopathic–proteopathic pathogenesis.
Any medium-term reader of this Substack will be fully aware of how much time I researched and wrote about Tryptophan and its metabolic pathway, the Kynurenine Pathway, and its importance on both neurological disorders but special attention given its significant role in SARS-CoV-2 infection and long-term perturbation/damage.
Here the authors propose a new framework to analyze AD from the perspective of the disease being an autoimmune disorder., proposing that the release of Amyloid Beta by different stimuli, and its antimicrobial properties create a cascade effect against your own neurons, which releases inflammatory proteins, which in turn changes the immune state around the neurons, therefore creating a pathogenic loop.
Analyzing over 1000 small molecules in the brain, they identified tryptophan metabolism as the regulator of brain innate immunity, something I covered before in another piece (about protein mimicry).
Although the relationship between tryptophan metabolism and innate immunity is complex, IDO-1–mediated catabolism of tryptophan is the earliest step in the metabolic cascade and is a recognized immunoregulatory target, working in concert with IL-1β, tumor necrosis factor alpha, and nuclear factor kappa B.29 It is also well established that IDO-1 inhibition downregulates immuntoxicity and ameliorates cognitive impairment in the APP/PS1 AD mouse model;30 moreover, tryptophan analogues, including 1-methyltryptophan, are known IDO-1 inhibitors.31 Additionally, IDO-1 inhibition may contribute to reducing neurotoxicity by diverting tryptophan to the hydroxylase-initiated serotoninergic pathway, thereby increasing the biosynthesis of anti-oligomeric tryptophan metabolites, such as 5-HT.
As I wrote about while covering the Kynurenine Pathway and its complex relationship with both metabolism (bioenergy) and the immune system, here the authors went to great detail to find very specific molecules to inhibit this pathway and diverge the Tryptophan metabolism towards the “right” side, since supplementation with merely Tryptophan can be “chaotic”, you often don’t hit the right target and it needs a lot of trial and testing to find the correct dosage of many supplements in each person to ‘get it right’.
Their conclusion is similar to a few aspects I covered before.
A pathogenic-therapeutic role for tryptophan metabolism in AD is compatible with various clinical data: serum tryptophan levels show a statistically significant reduction with age, people with AD have reduced plasma levels of tryptophan, and acute tryptophan depletion in people with AD causes increased cognitive dysfunction.48, 49 From these observations, multiple therapeutic approaches emerge. The important role of the gut microbiome in producing neuro-active tryptophan metabolites represents one novel approach for therapeutic intervention.50
Leading us to the good news section of this substack, and rather…intriguing one…
Expert calls for vitamin B test on dementia patients
EXCLUSIVE: A new meta-analysis of 14 studies found those aged 60-70 who were supplemented with a combination of B vitamins and omega 3 fats had less cognitive decline than those who did not.
All patients suspected of dementia should be tested for vitamin B insufficiency, a leading expert says. Professor David Smith, former Chair of Pharmacology and Deputy Head of the Division of Medical Sciences at Oxford University says patients with early age-related memory loss should be checked for B vitamin and omega 3 levels with a simple blood test.
If levels are inadequate, patients should be prescribed supplements of B6, B12 and B9 (folic acid) together with omega 3 fats which when combined have been shown to slow or halt cognitive decline.
Prof Smith said the trial, which was part-funded by Alzheimer’s Research UK, showed the effects of B Vitamins plus Omega 3 outweighed any benefits shown in any drug trials.
He said: “The effect is greater than that of any drug treatment to date - with no adverse effects.”
He added: “This effect has more recently been confirmed by other studies - one of which found the benefits of this combination of supplements has more than three times the clinical dementia benefit of any drug trial.”
He added: “There is currently no cure for Alzheimer’s and there will never be a cure. By the time a person has developed this disease the brain is too shrunken and damaged to be repaired by any pill. Even if we could find a way to replace lost nerve cells we cannot replace the memories lost with those and ultimately those drugs will stop working. With such striking results why are these findings being ignored?”
“This combination of supplements has been shown to dramatically slow the progression of this disease. If a drug company trial had results like this it would be described as a multi-billion pound blockbuster overnight.”
Earlier when I was researching the Kynurenine Pathway, I was also looking for ways to modulate it, since this is at the core of everything I analyze and write, understanding a specific something to find a “way out” of that something. A very talented subscriber named Paul Traynor commented about a very peculiar set of papers in relation to the KP.
A common trait among many neurological and central nervous system disorders is the lack of Pyridoxine, also known as Vitamin B6, a good article centered around B6 and kynurenines can be found here. The same could be said for cardiovascular diseases. Similar effects could be ascribed to B12 and Folic Acid given the importance of both for many functions of our bodies and consequentially a lot of old foil, chronic sick, or suffering from chronic inflammation is often subclinically deficient in B12 and Folic Acid.
The body of evidence on the role of simple supplementation of certain vitamins and minerals in many diseases especially neurological ones at an older age keeps increasing by the day, yet is often overlooked by most of the scientific and medical community. From the article itself.
Alan Norris, 68, a former computer programmer and father of one, from Worthing, Sussex was diagnosed with dementia last December.
He carried out a cognition test at foodforthebrain.org which highlighted he was missing vital B vitamins. When started taking these in the form of supplements and improved his diet and became more physically and socially active he says his “brain came back to life.”
His wife Dorothy, 73, a former midwife, said: “The transformation in three months has been remarkable. I feel like I’ve got my husband back.”
Last but not least.
Advanced imaging shows Lyme-related brain fog is real
There are approximately 476,000 people diagnosed with Lyme disease annually in the US. Of these, an estimated 10-20% suffer from impairing symptoms well beyond the acute phase of infection.
Persistent symptoms include severe fatigue, pain, and cognitive problems. Vexingly, these symptoms can be difficult to validate using current diagnostic tests.
Patients are often told by their health practitioners: “your tests are normal, it’s in your head” (aka psychosomatic).
Researchers have discovered, however, that by using more advanced imaging modalities, brain changes can be objectively detected in Lyme disease patients.
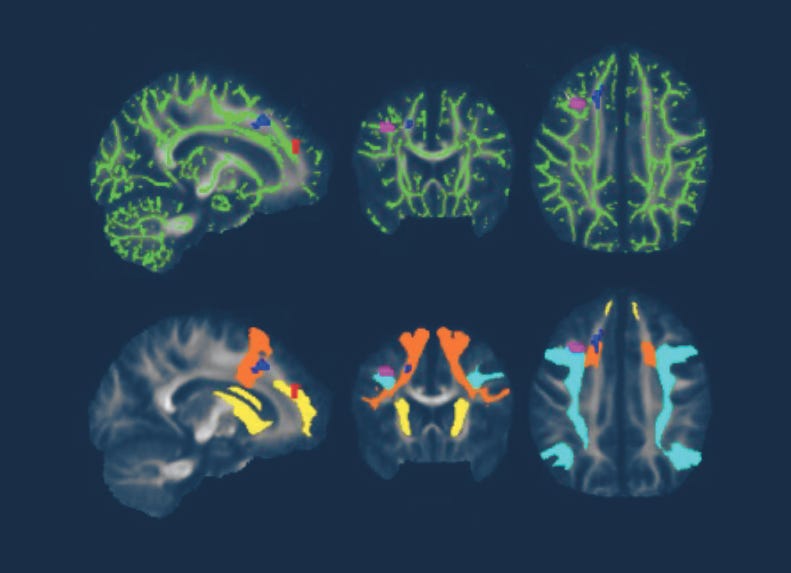
For example, clinical researchers at Johns Hopkins University School of Medicine have used novel PET imaging, functional MRI (fMRI), and diffusion tensor imaging (DTI) to identify inflammatory, functional, and structural abnormalities in the brains of Lyme disease patients as compared to healthy controls.
Their findings indicate that Lyme-disease-associated brain alterations are biologic and measurable, not psychosomatic. These discoveries are significant but not yet well known by the physician community or broadly available to clinicians.
A 2022 Johns Hopkins University School of Medicine neuroimaging study utilized fMRI and DTI brain scans in conjunction with each other. These scans identified striking functional abnormalities as well as distinct structural changes in the white brain matter of Lyme disease patients.[iv]
A similar trend can also be found in Long-Covid after severe infections and long-term stay in ICU, among many other variables (use of certain medications, including mAbs, hypoxia, etc), at least finally, after many years, all other post-viral dysfunctional states are getting the attention they deserve and being taken seriously by some researchers.
Something I thought would occur when Long Covid first showed its ugly face, that post-viral syndromes would be taken seriously, come hell or high water.
I wish everyone a nice Sunday.
If you chose to support this work, thank you, you make building the Substack possible, also thank anyone who shares whatever they like.
Thank you for this article. My friend is a director of the Neurological Hospital in one of the European Countries. He has been "prescribing" a coctail of B vit + other vitamins, herbs, supplements, probiotics, prebiotics and Krill Oil for over 2 decades. Also, he has specific protocols how to take them (some dissolve in water some require oil, some need carbs only (like tryptophan) to cross b/b barrier, some are better taken in the morning on empty etc) however he still says it is a progressive disease, sadly. John, would be great if you would do an article on protocols you would consider taking for certain "conditions" either for "optimisation" of health, "prevention" of some diseases, "first line intervention" etc....that would be awesome and would help bring all your thoughts together in the context of protocols that one might consider taking. Thank you for this article. Hope you are enjoying your weekend and breathtaking landscapes you get go to for your weekend hikes.
A tremendous thank you for all your efforts to educate us and keep us up to date. This is pertinent information for the non-expert to use to take actions to improve their health by simple means. As a nutrition and exercise trainer who stresses wholistic methods to the modern ills people suffer these days every post from you helps me help others.
A heartfelt thank you and appreciation for your deep dives and insights.