


mRNA vaccination in children alters immune responses
Up to 6 months

As I wrote shortly ago, I will cover the following paper, but in the same article I wrote that DoorlessCarp also covered this paper, you should definitely read his article, so I will look into it from a different perspective. But first a clarification of changes, the paper uses the term “heterologous” many times, and it is just a fancy academic term for off-targeted, unintended. I will change each mention to off-target for easier digestion of the content.
Off-target effects can be both positive or negative, it is like everything in life, context-dependent. A perfect example of a positive off-target effect is Metformin, a glucose management drug that has over 20 “off-target”, but positive effects.
First, a little bit of history. A couple of years back a peculiar paper was published, to wide criticism, this paper, was the first paper to propose that the mRNA vaccines reprogram the innate and adaptive immune system.
There is a substantial likelihood the authors revised the paper based on “public and private” pressure, and revised data 3 or 4 times since 2021, the paper is now peer-reviewed, and I dare say, the current version is the best one. It is important to note this little bit of history because the paper we are about to cover and “connect the dots” with other non-linear dynamics replicated the findings. In children.
BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists

I will first cover the most important sections of the paper and build the complexity from that point forward.
They tested the blood of the kids enrolled in this study at different time points, usually 28 days after the first and the second dose each. In line with all the evidence, when each sample was challenged (fancy speak to introducing something to a sample of something you are testing) with the first half (S1) and the second half (S2), there was an increase in cytokine response, those being TNF-α, G-CSF, PDGF-BB, VEGF, FGF-basic, IL-4, IL-12p70, IL-17, and IP-10, you are probably familiar with a few of these if you are a long time reader, as expected vaccination alone wasn’t enough to create a immune response towards the Nucleocapsid protein.
When tested against a myriad of different substances, such as fungi, bacteria, viruses, and TLR agonists, there was a general decrease in immune response in the children between 28 after Dose 1 and 2. You can see the measurements below.
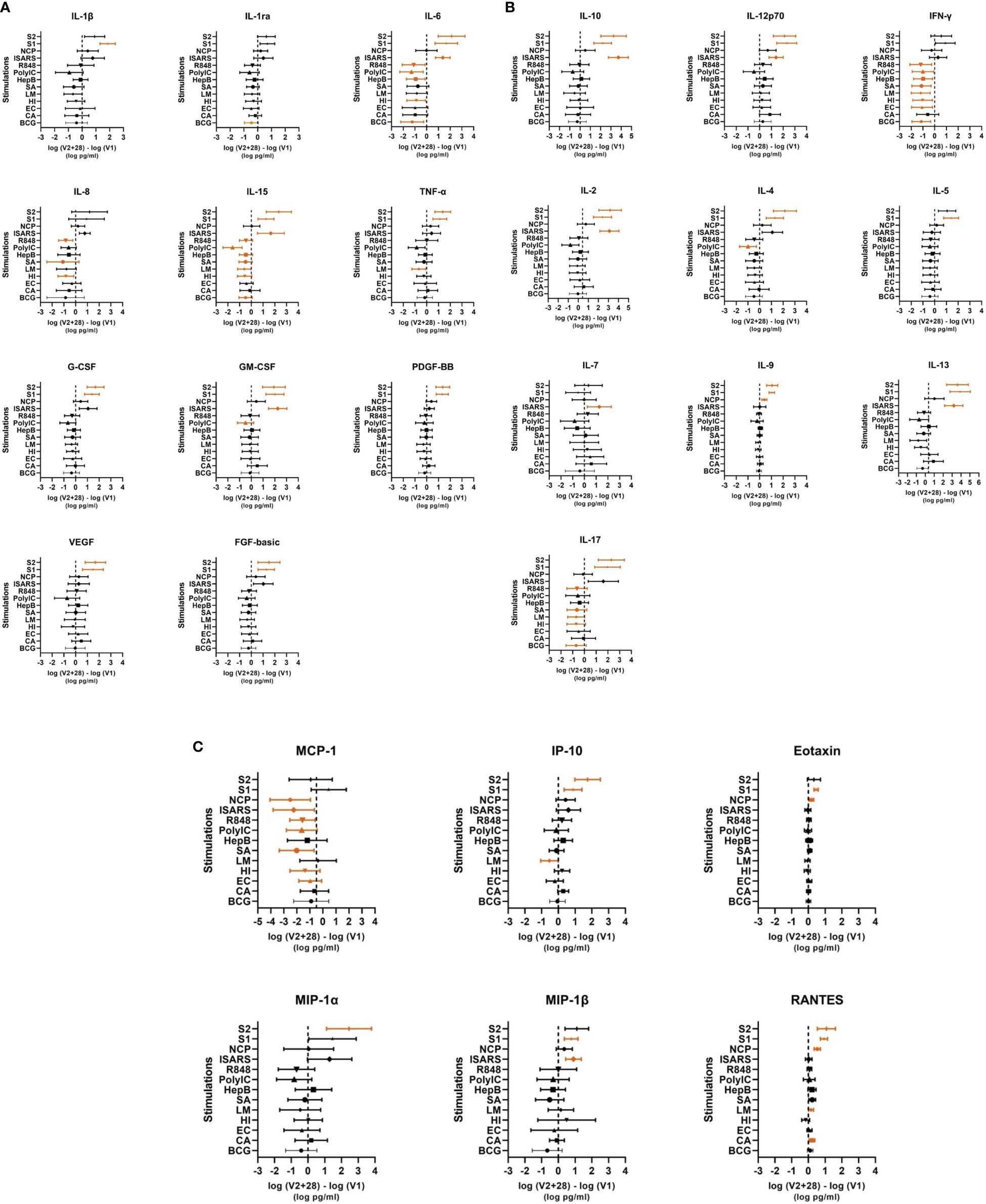
The largest decreases were seen for IFN-γ and MCP-1. IL-6, IL-15, and IL-17 were also decreased following the “challenge” with different stimulants (the dead pathogens such as EC, HI, or chemicals such as the R848 and PolyIC). In simple terms, in the first 28 days after each dose, your immune system responds very weakly against an assortment of pathogens.
It is worth noting that another “lie” from the vaccine manufacturers and government agencies, is one of the most important dynamics of long-term consequences here is the immune response against SARS, IL-4, IL-10, and IL-13, among other important proteins was high. This is indicative of a Th2 (allergic) immune response. While there is a labyrinth of pathways and overlapping mechanisms here, they all end up the same way.
Predominant Th2 and Th17 responses. Allergic reactions and stronger inflammatory reactions when encountering the virus. If the virus ever changes enough to bypass both antibody and T-cell immune responses and develop real ADE, this is how it can do it, by this specific immune response. But the SARS-CoV-2 immune response here is closer to a “tolerant” state, which may explain why the vaccinated don’t die of SARS-CoV-2 (at the cost of some of them dying from almost anything else).
In the first 28 days after vaccination in children, the children are very susceptible to responding poorly against SARS-CoV-2 (it is guaranteed they will be infected), while developing a detrimentally negative immune response against a myriad of common pathogens, with special attention to functional desensitization towards TLR3, 7 and 8, I will explain the meaning shortly. The only “improved” immune response, but actually not, was against Candida Albicans.
Their next step was to follow up with 8 of the children after 6 months, and they made sure they were Nucleocapsid negative (meaning somehow they avoided SARS-CoV-2 infection for 6 months). At 6 months, there is a measurable loss of sufficient immune response against viruses and a minor loss against bacteria infection, but there is a sufficient perceptible loss of chemokines response to both. Poorer chemokine responses mean your immune cells won’t move towards the locals of infection and a poor immune response is a guarantee.
For viral/TLR agonists (hepatitis B antigen, poly(I:C), R848) stimulations, there were decreases in several cytokine and chemokine responses in children at V2 + 182 compared to V1. Hepatitis B antigen and poly(I:C) stimulation responses were decreased for IL-6, IL-15, TNF-α, GM-CSF, PDGF-BB, VEGF, FGF-basic, IL-10, IFN-γ, IL-2, IL-4, IL-5, IL-9, IL-13, and Eotaxin at V2 + 182 compared to V1. In addition, at V2 + 182 compared to V1, hepatitis B antigen stimulation responses also decreased for IL-1β, IL-12p70, IL-17, and MIP-1β. Poly(I:C) stimulation response to IL-1ra, IL-7, and MIP-1α were also decreased at V2 + 182 compared to V1. Comparison of V2 + 182 to V1 did not show any decrease in cytokine responses to R848 stimulation except for a marked increase in IL-1β
Depending on the exact substance used to test the specific immune responses, they either remained low at 6 months or trended towards “normalization” at 6 months, in some cases they trended towards “compensation” rather than normalization. This effectively means the mRNA vaccine causes a profound and lasting impact on the immune system, irrespective of how you may interpret the “real” effectiveness of the vaccines.
Below the image is where I connect the dots and break down some of the complexity.
One topic I took a significant interest in this entire year was Endotoxic Tolerance, and the only reason I have yet to write is that the world doesn’t stop with all historical events. Regardless, I didn’t stop researching, and along the way I learned Endotoxin Tolerance is merely one side of the dice, it effectively means “Toll-Like Receptor 4 Tolerance”, and all other receptors can develop a “tolerant” too.
When faced with an Endotoxic Tolerant state, the body will effectively compensate by significantly lower production of IFN-γ, TNF-Alpha, and IL-6, followed by a lower but not as drastic drop in MCP-1 and IL-12. Endotoxin Tolerance trends towards normalization after weeks if no secondary infection occurs. The complex immune response of SARS-CoV-2 + all other pathogens chosen here are very reminiscent of this state.
For a long while I have proposed what happens after vaccination is a sequential feedback loop of immune dysfunction, in which a new infection creates a cascade effect of poor immune response. Given that the response to Influenza is affected by the vaccines both at a protein and microbiome level if infected by Influenza, desensitization to bacterial TLRs will happen after a flu infection, thus leading to a secondary bacterial infection.
The poor immune response against different viruses will initiate a months-long cascade of dysfunctional immune responses, and small chance of developing immune paralysis, a state where the immune system doesn’t respond well to any subsequent infection, but still produces inflammation.
Everything describe here is not only a perfect mixture of multiple pathway that are able to induce autoimmunity (known as loss of immune tolerance against yourself), but also contribute to long-term consequences, such as describe below, and in many other articles here.
The “stronger” response against Candida Albicans, at first sight, looks productive, but with the breakdown of the proteins involved, it shows a trend at an inflammatory, but not proper anti-fungal immune response, thus it may lead Candida to just develop biofilms.
Candida Albicans, together with Aspergillus Fumigatus are known to produce Gliotoxin, in simple terms you can imagine it as the endotoxin of fungi. Biofilms formation is correlated to higher levels of gliotoxins, and gliotoxins are a well-known disruptor of proper glutathione function, basically, it causes a antioxidant failure cascade. This may explain why people with Long Covid and with Candida problems are so “starved” of antioxidants, and why some of them.
This can lead the body to compensate by “starving” itself of serotonin and tryptophan to produce Kynurenine, a double-edge backup antioxidant system. TLR7 is also involved in the responses against Candida.

But the most important aspect of the following paper was not potential outcomes or my proposed hypotheticals (Candida), but the significant impact of Toll-Like Receptor 3, 7, and 8 responses towards viruses. These TLRs play an important part in “sensing” and controlling HERVs. Loss of TLR3 and TLR7 function leads to HERV “viremia” meaning uncontrolled production and presence of HERVs, and the loss of 3, 7, and 9 can lead to HERV-induced tumors (aka another mechanism for turbo cancer).

This leads us back to my Misfolded Protein article. While I try very hard to avoid doom and gloom now, cancer, but especially the following will become commonplace at uncharacteristic younger ages. The changes in the immune system covered here happen in almost any age group but 65+, and at still to be uncovered and categorized, to a very different and smaller level in anyone infected with any Omicron variant.

The next article will take a few days, as I planned it will be about how the body deals with misfolded proteins.
If you support this work or choose to at any time, thank you !

Hopefully I did a good job so most people are able to understand the significance of these finding (together with DoorlessCarp article btw).
One thing I didn't have the time to cover yet, at least at a sufficiently good level is how Omicron is causing a bunch of neurological issues in children, in China. Once again, vaccine is merely faster at inducing the worse SARS2 can do. I am not liking this predilection of omicron into going up to the brain every infection =(.
Dear JP related and unrelated... didn’t look for a more appropriate place to post this:
I wanted to shortly share some experience I recently had with a friend who tried some stuff with my humble assistance (treated for depression, 4 good professionals on the case, reported to me exhaustion after exercise, another MD had linked her symptoms back to hepatitis vaccine more than 10 years ago, thus my conclusion: chronic fatigue syndrome, she was good on the usual supplements D, C, Zn etc., some indication of leaky gut (serum zonulin, I know, probably unspecific), and, at the time I came in, she was at significant suicidal risk). She started with adding taurine (and reported significantly more energy), we wanted to add creatine but it never came to that, we added acetyl carnitine, for the leaky gut, glutamine (quite low dose) was already in her usual supplements; then she added 1.8g of butyrate (meant to feed certain nicer bacteria and to increase endogenous melatonin, I was not yet aware of the GLP1 stimulation) for 2 weeks (now reduced the dose). After these 2 weeks complete recovery from that suicidal phase. I assume butyrate (in combination rather than as a single fix) regulated the messed up tryptophan metabolism (and, whatever this is worth, the zonulin was back to normal as well).
Thanks for all the work you are sharing.