
mRNA induced thyroid problems, its axis and further vaccine failure
And endless drug shortages

For a number of months, I kept track and incidentally wrote whenever a felt necessary about drug shortages, or in better terms, the ever-growing list of drug shortages. And in one specific class of drugs, I obfuscated some of the reasons for the shortage, which I will get into it soon.

Pfizer recently sent a warning a few days ago that the company will run out of antibiotics for the penicillin family.
After the FDA first reported a nationwide penicillin shortage in April, Pfizer updated its hospital customers on the expected limited supply of its Bicillin prefilled syringes. The Pfizer antibiotic comes in a long-acting form or in a combination of two different penicillin types.
Pfizer attributes the supply hiccup to a “complex combination” of factors, including “significant” demand increases and a rise in syphilis infection rates, the company's hospital’s opioids and prefilled syringes director, Kevin Martyn, wrote in the update. It is not solely a US problem or a “Pfizer clientele” problem, but rather a global problem, especially in rich, highly vaccinated countries.
Per the news article excerpt above, Pfizer, and other drug companies too, attributed the shortage of many drugs to a complex combination of factors often alluding to the logistical chaos of 2021 and early 2022 to bear a sizable part of the burden here. Partially true, and as I wrote several times, the drug supply is extremely lethargic and slow to react and fix its problems.
Pfizer estimates its supply issue to be fixed at some point in 2024, but here is partially what I obfuscated before, while it is true that demand is growing, and I put most of the fault on both SARS-CoV-2 and the mRNA vaccines (most on the vaccines after 2021), demand will only increase for years to come.
While Omicron is mild, as in it lacks the ability, or propensity to penetrate deep into your lungs and cause the onset of pneumonia inducing slow respiratory failure, it is inducing a long of change, undiagnosed for the majority of the cases. There is an absurd amount of antibiotics being prescribed for all age groups after asymptomatic Omicron infection, and before the mundane argument “only in the jabbed”, yes mostly the vaccinate but not solely.
Omicron is an attenuated version of SARS-CoV-2, it doesn’t mean “incapable of inducing harm” it means less capable, especially if harm is measured by the severity of infection and mortality. China and India dominate the drug manufacturing market, and it is not different for antibiotics, anything goes wrong in the supply chain, or conflict breaks between China and Taiwan, and that line is cut abruptly and supply drains fast.
If everything is discussed so far, I will reiterate again (something I dislike doing too often) you should build a small stash of life-saving drugs. There are natural alternatives, yes, but a lot of conditions (to come) need drugs.
This leads me to the second part of this substack. I outgrew “dunking” on vaccine failure, not only I forecasted, I covered and wrote in depth the mechanisms by which they fail, they cause antibodies to be lethargic, and especially the potential harm, it is just “boring”. But surprisingly to me, there are still countries pushing it, so first things first.
Risk of Coronavirus Disease 2019 (COVID-19) among Those Up-to-Date and Not Up-to-Date on COVID-19 Vaccination
Results
COVID-19 occurred in 1475 (3%) of 48 344 employees during the 100-day study period. The cumulative incidence of COVID-19 was lower in the “not up-to-date” than in the “up-to-date” state. On multivariable analysis, not being “up-to-date” with COVID-19 vaccination was associated with lower risk of COVID-19 (HR, 0.77; 95% C.I., 0.69-0.86; P-value, <0.001). Results were very similar when those 65 years and older were only considered “up-to-date” after receiving 2 doses of the bivalent vaccine.
Conclusions
Since the XBB lineages became dominant, adults “not up-to-date” by the CDC definition have a lower risk of COVID-19 than those “up-to-date” on COVID-19 vaccination, bringing into question the value of this risk classification definition.
Summary
Among 48 344 working-aged Cleveland Clinic employees, those not “up-to-date” on COVID-19 vaccination had a lower risk of COVID-19 than those “up-to-date”. The current CDC definition provides a meaningless classification of risk of COVID-19 in the adult population.
This study and the first graph in the figure section are making the rounds today, demonstrating a lack of effectiveness of the bivalent booster vaccine, to the evidence of the past few months which already demonstrated the same multiple times before and especially after the Omicron variant surfaced. Also in line with previous evidence, it demonstrates that the more recently vaccinated are at a higher risk of infection.
Sadly unlike a few other similar studies with the same methodology, we don’t have viral loads, I suspect a lot of the bivalent boosted have higher viral loads, for longer periods. If you want to understand the disparity even among vaccinated, I have written about it recently.
A simplistic summary. Even vaccinated, if you get infected with any Omicron variant, argumentatively the more recent the variant “the better”, the immune system attempts to compensate for the immune imprinting, and develops immunity against the other parts of the virus, leading to better control of infection, even avoiding it sometimes.
Given recent evidence linking some of the immune axis I proposed as early as 2021 as being problematic or leading to long-term inflammation, it is time to gaze upon a can of worms I avoided for a while.
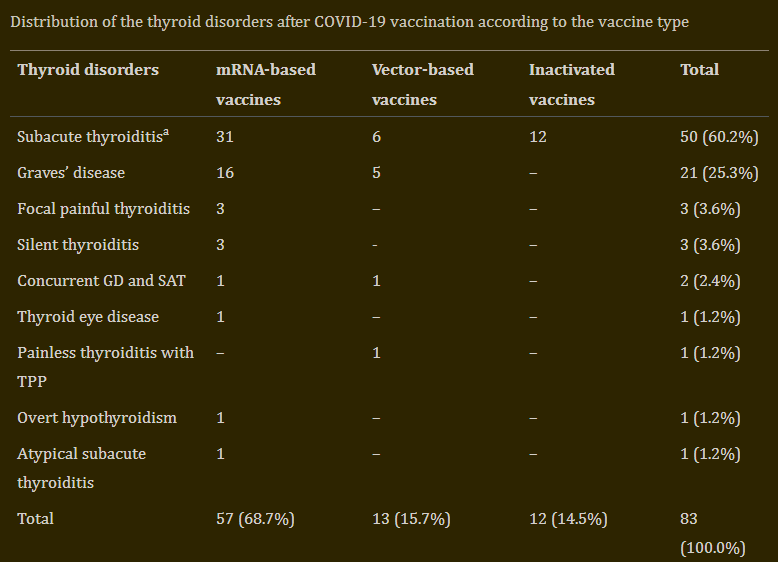
Endocrine diseases induced by mRNA vaccination. It is no secret that people with endocrine problems can have a harder time with Covid, especially thyroid problems, but now there are many cases of endocrine problems after mRNA alone. The most recent is Grave’s disease, a rare thyroid disorder, and here the authors argue is the adjuvant, but it isn’t in my opinion. In 2022 we had cases reports of thyroid disease after mRNA, another study had more cases (mostly with good outcomes after treatment).
I think this is enough to make the argument and link between the two, and I personally avoid cataloging vaccine injury just for the sake of it. Very recently I wrote about how SARS-CoV-2 directly affects the liver and Covid infection and vaccination are linked with developing diabetes (another aspect I wrote extensively about). One thing I didn’t mention before was the Gut-Liver-Thyroid axis.

At the end of my most recent Covid substack (above) I had this.
The reason I bring this paper up, besides its importance on its own is two-fold.
IL-12/IFN-gamma axis is a known modulator of the IDO pathway, leading to both immune suppression and inflammation, and abnormal activation of the Kynurenine Pathway, shifting Tryptophan to the “wrong side”. It is, effectively, a fairly well-known metabolic trap
The genes that are regulated and shifted with the persistent or high levels of this axis are one of my main arguments against the mRNA vaccine and are responsible for a lot of diseases of many etiologies
Now I want you to do a little research, it is simple, won’t take much time, and will not be hard to understand. The second bullet point links to the substack below, I want you to use the search function on your device and search for thyroid.

There is also an unspoken link between Endotoxins (especially sepsis…you should pay attention to this word…) and Thyroid disorders. There is a wave of endocrine and thyroid problems coming the healthcare way. And in line with the substacks linked here.
The Kynurenine Pathway—New Linkage between Innate and Adaptive Immunity in Autoimmune Endocrinopathies
Experimental hypothyroidism raises brain kynurenic acid - Novel aspect of thyroid dysfunction
My next two substacks will be about sepsis and covid, and the importance of proper tryptophan metabolism, the second I found quite interesting…results. Also if you have interest in me covering other subjects.
Have a nice rest of Saturday and a chill or fun Sunday everyone.
Thank you for supporting this work so far !
As helpful as your substack is (and I find it very helpful) it scares the shit out of me! The level of attack we are up against seems way beyond what I can defend against. I have a husband and 8 children to protect.
I try my best. But all this destruction of our innate immune systems seems so overwhelming! I look ahead and all I see are years of battle battle battle. I suspect I won’t win every battle and therefore I’m bracing for the reality that my loved ones will be hurt badly by all this shit. May God help me.
Reading this got me to realize a hypothesis that I believe should be explored. When I was in my 20s (after a lifetime of eating the standard American diet) I developed *hyper* (not hypo) thyroidism.
I previously attributed this to some environmental exposure (such as fallout from Chernobyl) but now I am wondering if *hyper*thyroidism, which is an overactive thyroid causing a person to have higher heart rate and metabolism (in turn driving weight loss) is the body's first attempt to naturally reverse obesity induced by diabetes.
Overactive thyroids often burn out leading to *hypo*thyroidism, which is low thyroid function that would make the standard American diet triggered diabetes even worse.
It took me years to discover my *hyper*thyroidism, and I'm guessing this same process may be happening with a lot of diabetics. Hyperthyroidism, followed by thyroid burnout, followed by hypothyroidism.