

December was a slow month because of many reasons, and now getting “back to it” I feel the need to share a few papers that I don’t think to deserve such in-depth write-up, but they do deserve some attention, given the current circumstances.
As XBB rips through North America and soon the rest of the globe (a most likely scenario), I do feel the need to bring this one to your attention.
Well, as a matter of fact, and as my usual work method, I used the Substack search feature to see what I covered so far, and to my surprise, I already did write about this particular paper in November of 2022, at the time a pre-print.
I find it somewhat interesting that many papers that present evidence against the current vaccine strategy and some very concerning papers (IgG4 as an example) are now peer-reviewed in “big” scientific journals. Something changed in the editorial section of said papers…
Yet one has to wonder how world governments and health authorities will push for mass adoption of all the other mRNA vaccines in the pipeline of the biggest pharmaceutical and biotech companies on the planet, over 2 dozen new vaccines for different diseases, let alone all the other myriad of uses for mRNA intervention (muscle, organs, cancer).
I have a long list of substacks following the evolutionary trajectory of SARS-CoV-2 in regards to novel antiviral treatments, with the most recent one being one talking about Paxlovid usage becoming dangerous on many levels, and now we can add the blatantly obvious to the list, as many scientists warned very early Merck’s drug was a mutational factory.
Antiviral treatments lead to the rapid accrual of hundreds of SARS-CoV-2 mutations in immunocompromised patients
The antiviral Molnupiravir (Lageviro) is widely used across the world to treat SARS-CoV-2 infection. Molnupiravir reduces viral replication by inducing mutations throughout the genome, yet in patients that do not clear the infection, the longer-term impact of the drug on virus evolution is unclear. Here, we used a case-control approach to monitor SARS-CoV-2 genomes through time in nine immunocompromised -patients with five treated with Molnupiravir. Within days of treatment, we detected a large number of low-frequency mutations in patients and that these new mutations could persist and, in some cases, were fixed in the virus population. All patients treated with the drug accrued new mutations in the spike protein of the virus, including non-synonymous mutations that altered the amino acid sequence. Our study demonstrates that this commonly used antiviral can ‘supercharge’ viral evolution in immunocompromised patients, potentially generating new variants and prolonging the pandemic.

We are finally getting data and evidence in what the authors themselves see as a knowledge gap and one that is pretty significant given the broad impact certain measures have on the grand scale.
My biggest concern/problem with many of said papers is how strict the definition of an immunocompromised patient usually is, from a clinical standpoint only real, “severe” cases of a very dysfunctional, compromised immune system are taken into account, but these should be no surprise I have written for over a year many of the vaccinated are effective paradoxically immunocompromised at different levels and aided viral evolution.
How many of the mutations that define Omicron, and the new dominant variant XBB didn’t merely come from poor neutralization from vaccine-elicited antibodies, but also from widespread usage of both Pfizer’s useless drug, and Merck’s dangerous one ?
For laypeople, a fixated mutation means exactly that, a mutation that persists and will be passed down, the virus now “achieved” a change (meaningful or otherwise would remain to be seen/tested). I do not expect newer drugs to be any better. We have numerous interventions that work on the virus at different levels and are aimed at different proteins, such as this paper.
We previously showed that Erythromycin, Retapamulin, Pyridoxine, Folic acid and Ivermectin inhibit SARS-COV-2 induced cytopathic effect (CPE) in Vero cells. In this study and using validated quantitative neutral red assay, we show that the inhibition of CPE is concentration dependent with Inhibitory Concentration-50(IC50) of 3.27 μM, 4.23 μM, 9.29 μM, 3.19 μM and 84.31 μM respectively. Furthermore, Erythromycin, Retapamulin, Pyridoxine, Folic acid and Ivermectin dose dependently inhibit SARS-CoV-2 Papain-like Protease with IC50 of 0.94 μM, 0.88 μM, 1.14 μM, 1.07 μM, 1.51 μM respectively and the main protease(MPRO) with IC50 of 1.35 μM, 1.25 μM, 7.36 μM, 1.15 μM and 2.44 μM respectively. The IC50 for all the drugs, except ivermectin, are at the clinically achievable plasma concentration in human, which supports a possible role for the drugs in the management of COVID-19. The lack of inhibition of CPE by Ivermectin at clinical concentrations could be part of the explanation for its lack of effectiveness in clinical trials.
Pyridoxine is a form of Vitamin B6, one I shared recently as being potentially helpful to treat and ameliorate different cases and degrees of sequelae of Covid (and this was brought to my attention months ago by a subscriber named Paul). Erythromycin, and Retapamulin are both antibiotics, and I found it rather peculiar that two antibiotics directly interfered with different effects and mechanisms the virus induces. Erythromycin itself directly inhibits certain effects of LPS…
And since IgG4 and allergies are all the rage.

In line with the papers I shared above, a new article was published raising concerns about the development of anti-PEG (polyethylene glycol) after the use of SARS-CoV-2 mRNA vaccines.
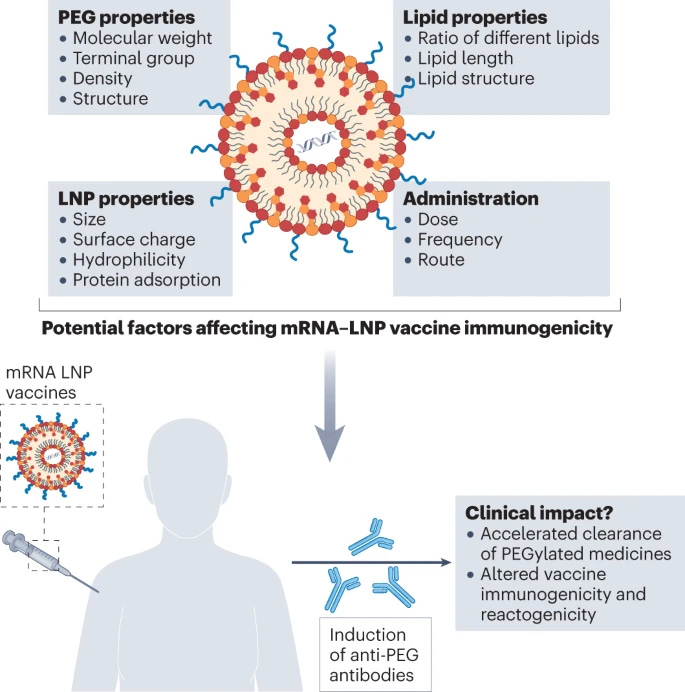
Nonetheless, larger long-term clinical studies, supported by incisive animal studies, using multiple booster mRNA vaccines are needed to assess whether anti-PEG antibodies may ultimately limit vaccine effectiveness.
This suggests that elevated levels of anti-PEG antibodies may promote sequestration of PEG-containing nanomedicines through complement opsonization, which may lead to accelerated blood clearance. However, further studies are needed to understand whether anti-PEG antibodies induced by mRNA–LNP administration can promote accelerated clearance of other nanomedicines.
It has also been proposed since the very proposition of using mRNA as a vaccine platform and the information of the composition of said vaccines containing PEGylated components would potentially increase systemic adverse reactions and could induce autoimmunity issues in certain people. Here is an extensive paper on the relevance of pre-existing anti-PEG antibodies and what it means. The number of drugs and chemical compounds used in daily life that contain different, even trace amounts of PEG is really big, so developing different levels of anti-PEG antibodies at a societal level can end up being quite the problem.
If you search “PEG allergy” you will be bombarded by many scientific papers between PEG and one of its most common allergic reactions, anaphylaxis. Anti-PEG antibodies have been proposed as one of the reasons for hypersensitivity when vaccinated with mRNA.
And since I rather not send a short e-mail today, a very important aspect I covered weeks ago. Drug shortages, and now price increases.
Exclusive: Drugmakers to raise prices on at least 350 drugs in U.S. in January

NEW YORK, Dec 30 (Reuters) - Drugmakers including Pfizer Inc (PFE.N), GlaxoSmithKline PLC (GSK.L), Bristol Myers Squibb (BMY.N), AstraZeneca PLC (AZN.L) and Sanofi SA (SASY.PA) plan to raise prices in the United States on more than 350 unique drugs in early January, according to data analyzed by healthcare research firm 3 Axis Advisors.
The increases are expected to come as the pharmaceutical industry prepares for the Biden Administration's Inflation Reduction Act (IRA), which allows the government's Medicare health program to negotiate prices directly for some drugs starting in 2026. The industry is also contending with inflation and supply chain constraints that have led to higher manufacturing costs.
The increases are on list prices, which do not include rebates to pharmacy benefit managers and other discounts. In 2022, drugmakers raised prices on more than 1,400 drugs according to data published by 46brooklyn, a drug pricing non-profit that is related to 3 Axis. That is the most increases since 2015.
This isn’t a US issue, it is a global issue, the Greek pharmaceutical agency is now looking into the issue, meeting with wholesalers and pharmacies to understand and attempt to tackle the issue, Pakistan and other countries find themselves in a similar spot. Germany is also suffering from drug shortages, and it is getting rather bad for producers.
The inflation created by the EU is also threatening the supply of generic (affordable and necessary) drugs.

Inflation can damage production viability of European drugs
Once a drug’s patent expires, numerous pharma companies offer generic versions, which can then reduce drug pricing by as much as 80-90%, leading to small profit margins for generics makers. Even before the current period of high inflation, many pharma companies were already seeking to exit the generics space because of pricing pressures. This could endanger the supply chain; decreased competition often enables price increases but also involves a higher risk of drug shortages.
Rising inflation has been a problem globally but particularly in Europe, which was heavily reliant on Russian gas and oil before the Russia-Ukraine war and ensuing international sanctions and embargoes on Russian goods. The EU has banned the export of crude oil (from December 2022) and refined petroleum products (from February 2023), as well as coal and other solid fossil fuels. This has significantly increased the cost of energy in Europe.
The annual inflation rate in parts of Europe has increased to above 10%. This has led to increased manufacturing costs for generics which form the majority of medicines dispensed across Europe, often for serious illnesses. Raw materials, transport, fuel, and energy have all increased in price. Europe also enforces rigid pricing policies for essential medicines to be available at the lowest possible price. These factors combined affect the commercial viability of generic medicines, with some European drugmakers already warning that they may stop making cheap generic medicines. Additionally, some generic products are becoming loss-making, however, many companies are contractually tied into long-term deals with governments or hospitals.
I will cover this other side of the things on another substack, but since both are connected, I thought I should bring it up, especially because the situation will not improve anytime soon.
This problem has been developing for the most part of 2 years, and given the decisions of world governments in the last 18 months, the likelihood is for different drugs to experience and go through shortage for the entirety of 2023, and price increases will be but a reality in certain regions, if no type of big epidemic suddenly surfaces, draining an already strained global supply system. Case and point, when China reversed its 0 Covid policy, letting the virus just run through the entire population, it created massive shortages almost overnight.
As anything to do with China and its responses to SARS-CoV-2, the impact of its policy changes is always systemic and bears significant global impact, regardless of how severe a variant or any pathogen comes to be in the near future if too many countries experience simultaneous outbreaks, it will more likely than not “break the system” and cause months-long shortage of common, yet important drugs. The energy price/aspect of it all also directly correlates with supply and prices.
These paragraphs are a reminder for you to stock at least drugs that you need or might need in the near future (such as antibiotics). Rather be safe, than sorry (that is why in the last year I have been slowly building my antibiotics stash, which is ironic since I hate using antibiotics and basically used than only one time in my entire life).
Also, another reminder that most drugs don’t have an actual due date, and lose a very little small percentage of their potency after years and years of being stashed. Unless you are using opiates, such as Fentanyl, and ANY drugs that use patches as a delivery method, after its due date, the quantity delivery by skin changes drastically and one can easily overdose on said patch.
A friend learned that lesson with Fentanyl the hard way (survived though, yay).
I welcome and appreciate the support of those who choose a paid subscription, or who decide to buy me a coffee whenever they feel like it, and everyone who shares my Substack. Without all of you, this wouldn’t be possible.
Good to know the expiration date on drugs isn't necessarily an indication they no longer work. I use very few pharma products but keep a few things on hand.
Some symbiotic gut bacteria induce intestinal epithelial cells to express glycans, the complex proteosugars that can help protect gut mucosa against messages that could produce upregulation of inflammation. A molecular cross-talk clearly exists between the microflora and the mucosal epithelialium