Months ago, I wrote and proposed a scenario, which I called Reverse Marek’s Disease. For those unfamiliar, Marek’s Disease is a nasty poultry disease, airborne, in which if you don’t vaccinate your flocks against the current circulating strain, and one of your chickens gets infected there is a massive likelihood your entire flock will be either wiped out or culled. Marek’s has been studied for a long time because it is a perfect example of a leaky vaccine leading to disaster.
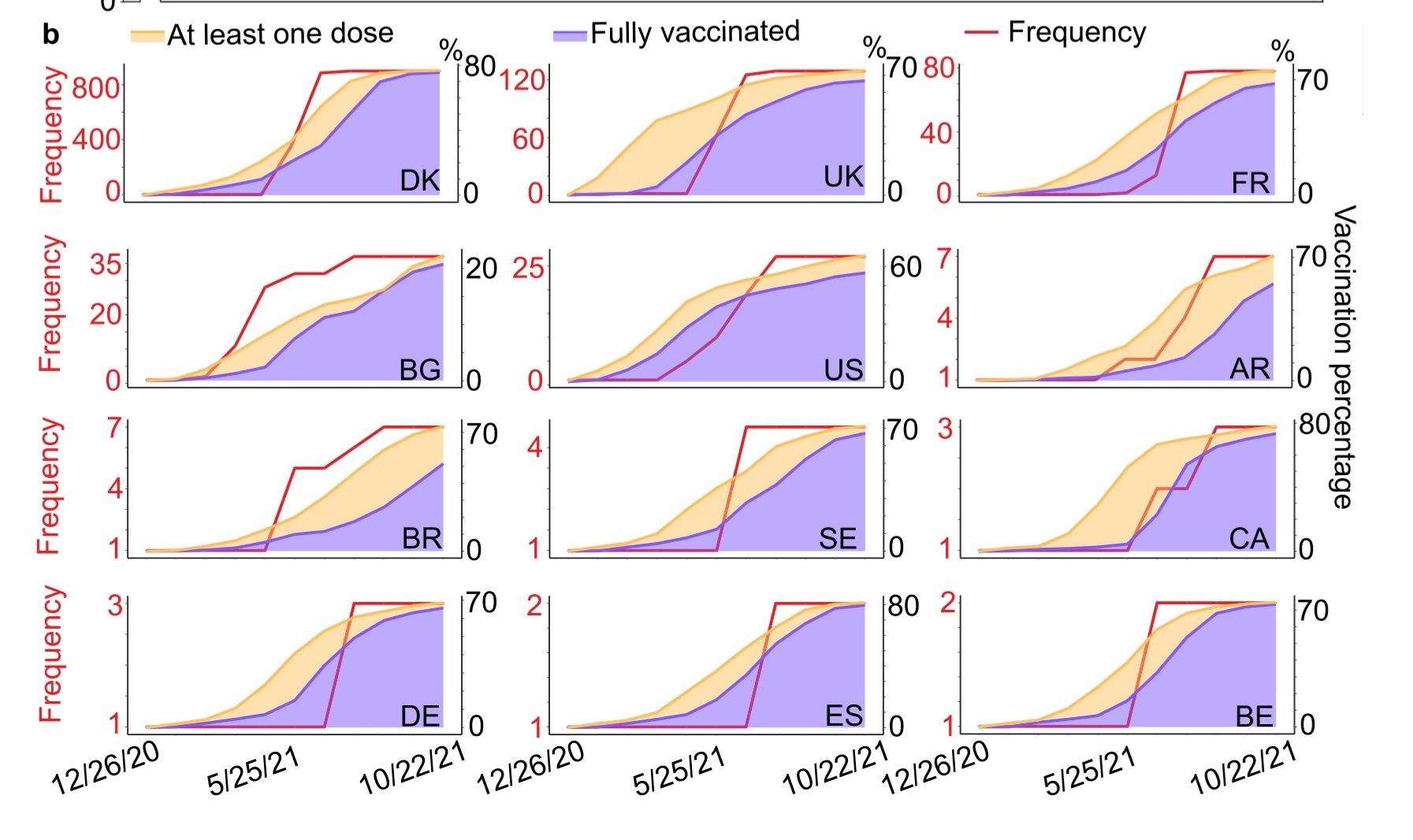
Reverse because as the enormous quantity of evidence demonstrates, over and over and over again for months, the vaccinated “chicken” (Spike-centric vaccinated individuals) would be the “chicken” spreading the disease, and fueling the evolution of the virus.
And for the record natural infection was always the superior method of “immunization”.
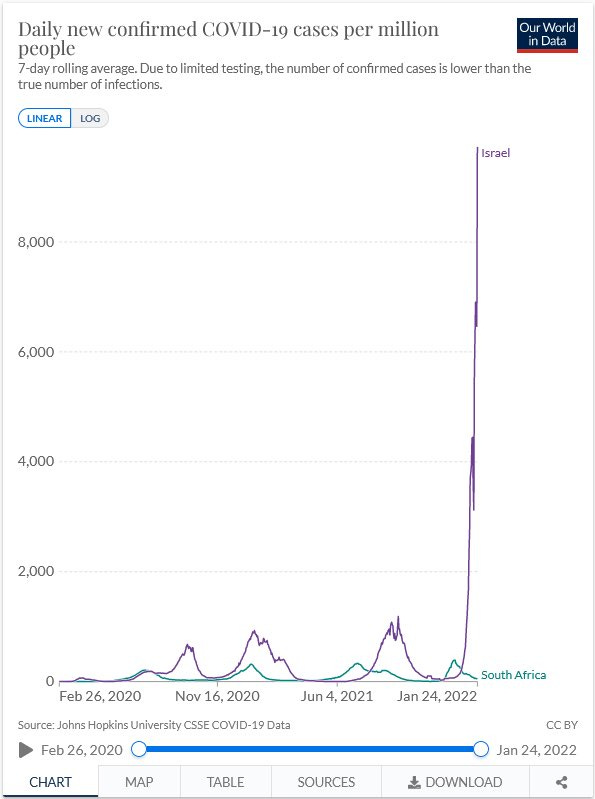
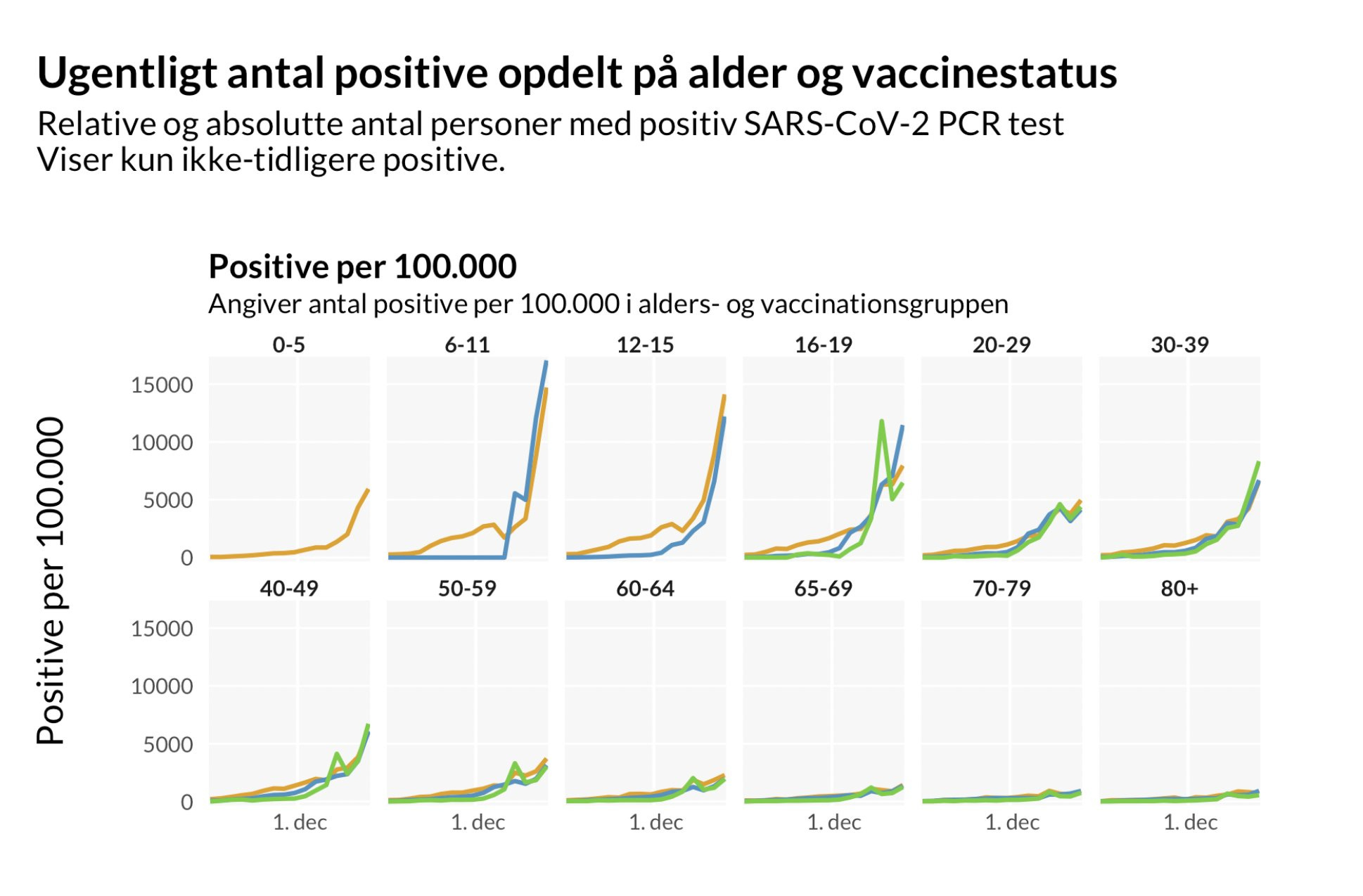
I could add graphs for days, recent ones, old ones, make a massive “dunking” Substack, but that isn’t the point, the point is to demonstrate that the trends were there since the start, but if there is one thing (and this will offend the scientists/doctors reading this), is that Science is too slow, too retroactive.
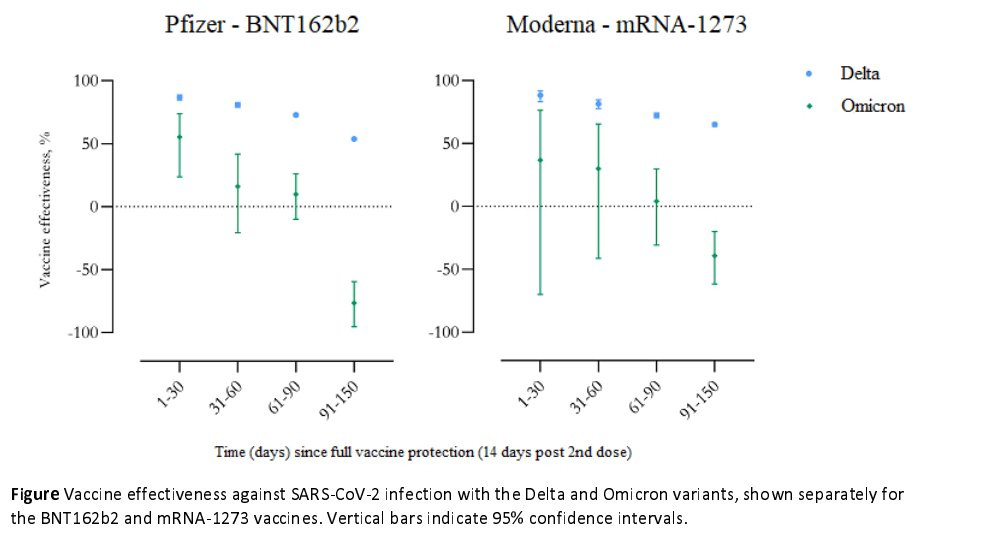
Very early on, all vaccines already showed signs of waning (papers about it here, here, here, and here, and didn’t elicit enough neutralizing antibodies. This all comes into play on both antigenic fixation and improper sterilizing immunity, a perfect mixture for a leaky vaccine.
Later after the vaccine’s mass rollout, there were enough safety signals for some doctors to write papers about the possible health risks of using the Spike Protein, the argument of some was the Spike Protein itself elicited cell signaling and that could lead to harmful effects, I have written about all of these to different extents but since I created this Substack, the quantity is rather substantial. Upon reading the paper above about non-neutralizing antibodies, I wrote:
You see, the problem is not merely that the vaccines Immuno suppress you, or turning you into a super-spreader, or even help the landscape of highly adapted viral mutation. The real issue is that now we have a Reverse Marek’s scenario, where the vaccinated create supercharged, highly transmissible viral swarms, which their compromised immune system can’t deal with, in turn infecting and creating a cascade in vaccinated individuals.
The soluble (meaning a free-floating protein part of something) spike protein will mimic the entire disease. Different parts of the spike will elicit different responses and activate different cell signalling, which cascades into inflammatory responses.
I still stand by my assertion, but now we know exactly how the Spike Protein is eliciting an immune response by itself, it isn’t merely the antigens or peptide sequences mimicking a wide array of proteins on the Spike Protein, but its ability to bind to endotoxins (LPS), this being the primary aggressor, consequentially the harmful amino acid sequences in the Spike being, the second.
Poor binding and poor neutralization lead to the persistence of viral fragments inside some of the infected, which may lead to persistent infections, Long Covid, and evolutionary pressure.
And more evidence to the contrary of what antibody salesmen spout out loud everywhere. Intra-host recombination isn’t new, especially for coronaviruses, one of the viruses more prone to recombination within a host, and here we have even more evidence of higher within-host diversity, meaning as anyone with even a cursory reading on basic biology and immunology known, the vaccinated were and are the ones generating immune evasive variants.
One point I made early on with Omicron, with the evidence available at the time was, there would never be an “effective” vaccine using Omicron-based Spike Protein, it wouldn’t work.
Unlike the test in rats for the “booster” approval, this paper did the test in humans, and the findings were not… pleasant for the antibody salesman. Paper here.
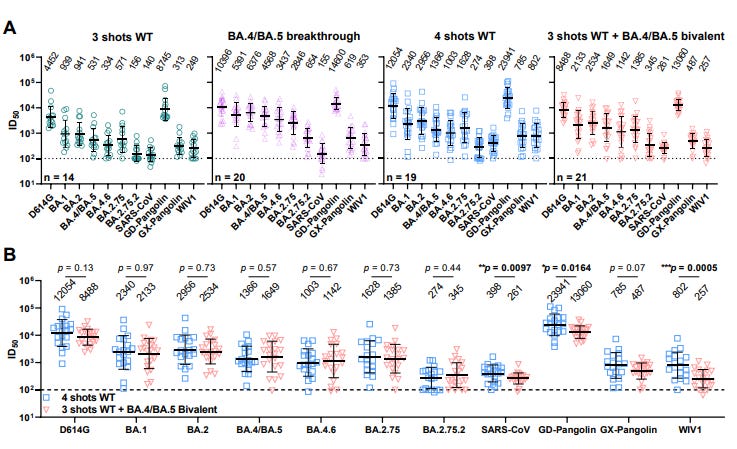
Clinical details are summarized for all groups in Table S1 and listed for each case in Table S2. Individuals who received four monovalent mRNA doses were older (mean age 55.3) than those who received a bivalent booster (mean age 36.4). Serum was collected from both cohorts at a similar time following the vaccine boost (mean 24.0 days in the monovalent group; mean 26.4 days in the bivalent group). All cohorts exhibited the highest serum virus-neutralization titers (ID50) against the ancestral D614G strain (Figure 1A). Geometric mean ID50 titers against SARS-CoV-2 variants were lowest for boosted sera and highest for BA.4/BA.5 breakthrough sera. There was no significant difference in neutralization of any SARS-CoV-2 variant tested between individuals who received a fourth monovalent vaccine and those who received a fourth dose of a bivalent vaccine (Figure 1B). ID50 titers against three related sarbecoviruses (SARS72 CoV, GD-Pangolin, and WIV1) were slightly but significantly higher in those who received a fourth monovalent vaccine dose compared to those who received a bivalent vaccine. Boosting with a new bivalent mRNA vaccine targeting both BA.4/BA.5 and an ancestral SARS76 CoV-2 strain did not elicit a discernibly superior virus-neutralizing antibody responses compared boosting with an original monovalent vaccine.
These findings may be indicative of immunological imprinting , although follow-up studies are needed to determine if the antibody 79 responses will deviate in time, including the impact of a second bivalent booster.
Testing into different age groups, and even different age brackets the authors found no difference in neutralization between any of the vaccines, be they using old Spike Protein, or Old Spike+New Spike (Omicron), but what got my eyes was the last, closing line.
“These findings may be indicative of immunological imprinting”. Also known in many circles as Original Antigenic Sin. Something many dozens of scientists, doctors, independent researchers, and average Joes with some time spent researching warned about since 2020. And merely 24 hours after the paper above was published, the one below went “online”.
Our data demonstrate that both monovalent and bivalent mRNA boosters markedly increased antibody responses but did not substantially augment T cell responses. BA.5 NAb titers were comparable following monovalent and bivalent mRNA boosters, with a modest and nonsignificant trend favoring the bivalent booster by a factor of 1.3. These findings are consistent with data recently reported for a BA.1-containing bivalent mRNA booster4 .
For future reference (and also past, because I covered all of these), your body needs a T cell response to properly fight and clear infections from your system, in regards to SARS-CoV-2, you need Nucleocapsid immunity, after the first SARS epidemic, they found that people with N immunity survived, while people without it, perished. You can read about it here, here, here in regards to SARS-CoV-2. Also, this paper titled “Nucleocapsid-specific antibody function is associated with therapeutic benefit from Covid-19 Convalescent plasma therapy”. A trend among “N immunity” is the fact that it gives you a strong CD8 response towards the virus, something the vaccines do not, never did.
Our findings suggest that immune imprinting by prior antigenic exposure5 may pose a greater challenge than currently appreciated for inducing robust immunity to SARS-CoV-2 variants.
For now, an understatement of the century, and most certainly the authors will get criticism for writing and publishing this paper, but the cat is out of the bag. Both papers lead me to believe why they insisted you need almost half a dozen of the original vaccines to take the new ones, because as I observed and deduced, it would simply not work properly without it, since this entire crime racket hinges on “antibodies”.
Repeated vaccination with the same nocive, highly inflammatory protein is inducing quite a few changes in the global immunological landscape, first, the B Cell responses in the vaccinated changed, and second, and most important of all. Their IgG class-switched from an inflammatory response to a less inflammatory one. This is still by far the most important piece of information in regard to what is to come, especially if there is a high expression of a certain chimeric Galectin…
Unless a massive breakthrough is published, a big epidemic explodes out of nowhere, even if takes me a few days, I will focus my efforts on the Galectin-3 substack, or maybe super shorter ones in between.
A big thank you to all supporters here and on KoFi, and also the people who share my substacks they find interesting.
Things Hidden in Complexity is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Your discussion about the N-protein reminded me, I paid for a full blood count a few weeks ago to 'mark' 12 months on from my decent lifestyle changes, and also check on certain levels of the supplements / vitamins I've been taking, and out of interest I selected the SARS-CoV-2 serology check also - Believe I had Omicron in April down here in Aus.




These things were never actually designed to prevent illness. Sometimes we must say things plainly.
Your discussion about the N-protein reminded me, I paid for a full blood count a few weeks ago to 'mark' 12 months on from my decent lifestyle changes, and also check on certain levels of the supplements / vitamins I've been taking, and out of interest I selected the SARS-CoV-2 serology check also - Believe I had Omicron in April down here in Aus.
Specimen: Serum
Anti-S protein IgG: Negative
Anti-N protein IgG: Positive
Anti-S protein IgM: Negative