

Depending on your perspective on life, your own mental health, and how/where you consume information, most of my Substack can be interpreted as either decent information or “bad” as in depressive information. To that effect, and for a couple of other reasons, both of these are “good” news, however you decide to look at it.
Also, as I often state, sometimes there is important information that doesn’t exactly fit in a single, short article, it is good for clicks and engagement, but to me, abhorrent and intellectually lazy, so I will use this opportunity to share it.
Many months ago I wrote, and repeated recently before deleting my Twitter account, that immune imprinting has been slowly, but surely being “overwritten”, given many complicated molecular and genetic mechanisms. In simple words, the virus changes so much, it is so different from the original strain, that the immune system is able to “update the software”.

Repeated Omicron infection dampens immune imprinting from vaccination and induces broad neutralizing profiles against other Omicron sub-variants
Protection from boosting with updated SARS-CoV-2 vaccines containing emerging Omicron sub-variants like BA.1 or BA.5 was not satisfying, especially the neutralizing ability against the newly emerged BQ and XBB related variants. Similar with influenza virus, antigenic drift is highly relevant to SARS-CoV-2 evolution, and immune imprinting may limit the performance of updated vaccines. In this study, we investigated whether repeated infection with Omicron variant could reduce the immune imprinting. A total of 194 participants with different status of vaccination (unvaccinated, regular vaccination and booster vaccination) confirmed for first infection and re-infection with BA.5, BF.7 and XBB variants were enrolled, and the neutralizing profiles against wild type (WT) SARS-CoV-2 and Omicron sub-variants were analyzed. The results showed that neutralizing potency against the corresponding infected variant is significantly hampered along with the doses of vaccination during first infection. However, for the participants with first infection of BA.5/BF.7 variants and re-infection of XBB variant, immune imprinting was obviously alleviated, indicated as significantly increased ratio of the corresponding infected variant/WT ID50 titers and higher percentage of samples with high neutralizing activities (ID50 > 500) against BA.5, BF.7 and XBB variants. Moreover, repeated Omicron infection could induce strong neutralizing potency with broad neutralizing profiles against a series of other Omicron sub-variants including the newly emerged EG.5.1 variant, both in the vaccine naïve and vaccine experienced individuals. In conclusion, our results provide useful information for the antigen selection and vaccination strategies, and indicated that repeated boosting vaccination with Omicron based vaccines especially the XBB sub-variant without the WT spike protein might achieve broad and efficient antibody responses against Omicron variant.
At multiple points last year, I wrote and broke down how and why Omicron vaccines would fail, it basically boils down to the Omicron Spike losing a lot of the “nasty” parts that made the other variants so aggressively damaging, or at the very least some of these parts were weakened. Changes proposed were insane, such as one of the latest vaccines adding 6 proline modifications instead of 2.
Here we are presented further evidence that breakthrough infections with different Omicron variants, in a crude way the more recent the better, attenuate the primary immune imprinting, in line with prior evidence. The mRNA imprinting is stronger than the other vaccine imprinting, but this also is getting “software updated”, it takes longer than usual, and the choice of not getting vaccinated again. Our bodies and immune systems are smarter than we are.
Knowing and having evidence of the attenuation of immune imprinting is a primary point to convince the remaining population to stop taking a genotoxic poison, and give them a fighting chance. To the effect of overcoming immune imprinting, a paper I covered 2 years ago already hinted towards this. This time, using convalescent plasma to expand N immunity and diminishing S immunity. Convalescent plasma (CCP) is a rather interesting and potential treatment.
The following paper is more complicated, but to me, “good news”, but truly is more along the lines of “how antibodies neutralize the virus”, the compelling finding is how. By proteolysis, by breaking down proteins into smaller pieces. Proteolysis is a very important aspect of biology, it can activate or inactivate proteins, it can generate bioactive peptides (the smaller protein, otherwise referred to as protein fragments), and degradation of misfolded proteins or damaged ones.
Spike-protein proteolytic antibodies in COVID-19 convalescent plasma contribute to SARS-CoV-2 neutralization
Before going into their experiments, the authors raise the pertinent point that CCP treatments are a very useful and attractive therapeutic option to reduce hospitalization and mortality, especially in hospitalized patients and those who are immunosuppressed. As a tangential personal note, proteolytic antibodies have been proposed as a biodefense target.
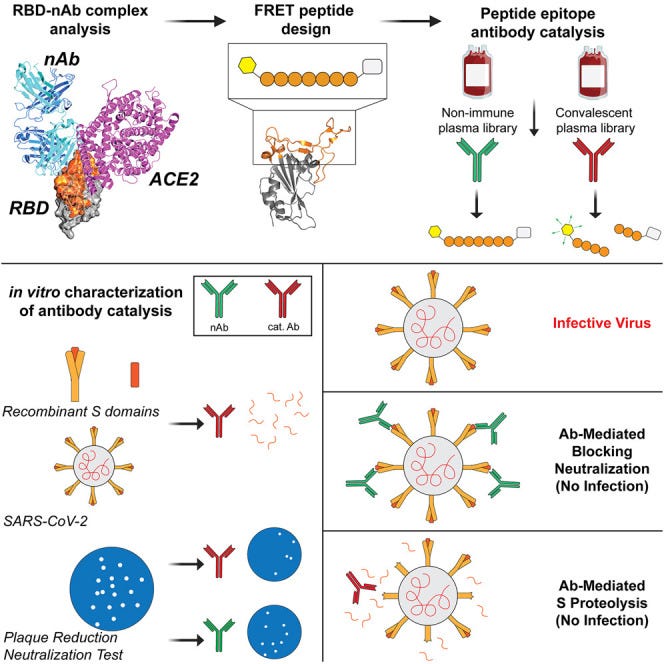
To test their hypothesis on if and how the authors decided to focus on two specific “parts” of the Receptor Binding Domain (RBD), the Receptor Binding Module (RBM) 1 and 2, since these are the specific regions that possess the most interaction with ACE2. Antibodies that bind (glue) themselves to these regions are thought to neutralize the virus because they out-compete the virus into binding ACE2. The sequence of RBM1 and 2.
RBM epitope peptide 1 (RBM1) consists of residues Lys444-Leu452 (KVGGNYNYL) and RBM2 consists of residues Val483-Ser494 (VEGFNCYFPLQS)

After conducting their experiments they observed that RBM cleavage occurred in all samples of convalescent plasma, but the cleavage rate (breakdown of the protein) varied, meaning the speed at which each person breaks down the protein is different. Interestingly, they found that higher concentrations of convalescent plasma did not lead to increased cleavage rates; instead, there was a decrease in activity, a phenomenon known as the hook or prozone effect. This suggested that there was competition among antibodies at high concentrations. This test was done under physiological conditions such as human body temperature.
To confirm that the observed cleavage was due to antibodies and not other components in the plasma, they heat-treated at high temperature the plasma to denature non-immunoglobulin components. They observed that a significant portion of the proteolytic activity was retained even after heat treatment indicating that antibodies in the plasma were responsible for the cleavage.
Further analysis revealed that some convalescent plasma samples had higher levels of RBD-specific antibodies, which correlated with faster cleavage rates. However, the proportion of RBD-specific antibodies did not solely determine catalytic activity, as samples with lower levels of these antibodies still exhibited cleavage activity.
To demonstrate the importance of RBD-specific antibodies, they depleted these antibodies from one sample of convalescent plasma. The cleavage of the RBM peptides was significantly attenuated in the depleted plasma compared to the untreated plasma, indicating that RBD-specific antibodies played a significant role in the cleavage process.
They also found a correlation between RBD-specific antibody titers and the RBM1 cleavage, supporting the notion that cleavage is associated with a specific antibody. To better understand how these catalytic antibodies function, the researchers used one of the samples (CCP3) and subjected these antibodies to protease inhibitors, these being AEBSF (which inhibits serine proteases), bestatin (targeting aminopeptidases), E-64 (which inhibits cysteine proteases), and pepstatin-A (effective against aspartic acid proteases).
The results showed that there was no significant inhibition of catalytic activity by E-64 or pepstatin-A, they observed a 42% inhibition of RBM2 cleavage by AEBSF and a 13% inhibition by bestatin. These findings indicated that a portion of the antibodies in the convalescent antibody population utilized mechanisms resembling serine proteases and aminopeptidases.
The most pertinent aspect of this paper to me was the cleavage of authentic S protein. The intensity of the intact rRBD decreased in a dose-dependent manner with increasing concentrations of CCP3 antibody, resulting in 20-78% degradation of rRBD. Similarly, rS1 protein was degraded by 21-59% under the same conditions. Specially the section “Although the degree of degradation was less than observed for recombinant S proteins in similar conditions (0–15% band reduction compared to no-antibody control), we also observed the concomitant accumulation of degradative S fragments.”
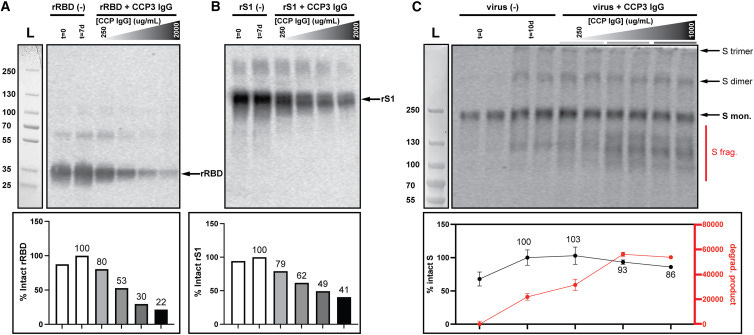
To further summarize and simplify, antibodies from infection can break down the Spike Protein, both being able to stop viral infection to a degree and most significant, break down Spike Protein itself, and they observed the accumulation of S fragment. This is significant for two reasons. First, the breakdown of Spike Protein by our bodies happens, this helps the body “clear” up the Spike Protein, and it affects the virus.
Second, and less “positive” is in relation to my 2 years long argument that a lot of the damage, both acute and long-term from the virus and especially proline-edited(vaccine) Spike Protein, and given the results here, and previous evidence, at a point after the initial infection, and breakdown of the Spike, there is a failure of the body to clear the Spike, and it gets “stuck” inside cells or tissue. Nonetheless, this serves as evidence that the body itself is capable of breaking down Spike. To what degree this happens in 4+ times vaccinated individuals has yet to be answered.
In line with the first paper covered in this article and the entire body of evidence from 2022. The title: Comparison of Omicron Breakthrough Infection Versus Monovalent SARS-CoV-2 Intramuscular Booster Reveals Differences in Mucosal and Systemic Humoral Immunity
Our understanding of the quality of cellular and humoral immunity conferred by COVID-19 vaccination alone versus vaccination plus SARS-CoV-2 breakthrough (BT) infection remains incomplete. While the current (2023) SARS-CoV-2 immune landscape of Canadians is complex, in late 2021 most Canadians had either just received a third dose of COVID-19 vaccine, or had received their two dose primary series and then experienced an Omicron BT. Herein we took advantage of this coincident timing to contrast cellular and humoral immunity conferred by three doses of vaccine versus two doses plus BT. Our results show that mild BT infection induces cell-mediated immune responses to variants comparable to an intramuscular vaccine booster dose. In contrast, BT subjects had higher salivary IgG and IgA levels against the Omicron Spike and enhanced reactivity to the ancestral Spike for the IgA isotype, which also reacted with SARS-CoV-1. Serum neutralizing antibody levels against the ancestral strain and the variants were also higher after BT infection. Our results support the need for mucosal vaccines to emulate the enhanced mucosal and humoral immunity induced by Omicron without exposing individuals to the risks associated with SARS-CoV-2 infection.
Notably, a BT infection enhanced T-cell responses even in individuals who were infected prior to their primary series and were therefore already hybrid immune.
I do not think injectable mRNA vaccines will ever be able to create mucosal immunity, and this is a point brought forth since early 2021 by dozens, if not hundreds of scientists looking into the pandemic. Lack of mucosal immunity is the main reason the mRNA vaccines failed to stop transmission, which should have been the main goal since the start, at least with that, the damage and the evolutionary pressure would’ve been contained to a satisfactory degree.
Breakthrough infections offer a superior and more complete level of immunity. It should be obvious by now, yet…here we are… I find this topic extremely boring and lazy now, so I will move on, I have written extensively and broken down its complexity for almost the entire year of 2022 if you are interested.
As the last topic of today’s substack. Among my many interests in regard to SARS-CoV-2, and health in general was, and still is liver function, especially the long-term impact this chimeric virus may exert on the whole population (meaning all age groups). The liver exerts systemic functions, beyond what most assume it does, so I have a major interest in the subject.
Liver abnormalities following SARS-CoV-2 infection in children under 10 years of age

Given that SARS-CoV-2 can directly infect hepatocytes, possessing many other effects, and how children’s immune system is fairly unique, and respond more “aggressively” to infection, this should not come as a surprise. As we often said in the last 2 years, SARS-CoV-2 is The Great Accelerator, and it is every other pathogen’s best friend. Sustained, or acute infection can prime individuals, kids in this paper, towards liver abnormalities, and “aid” into developing subsequent dysfunction and disease.
The authors find the direct infection of hepatocytes unlikely, and to this argument, they propose immune-mediated damage. This may be mediated by the other hyperinflammatory mechanism mediated by the S1 (I will need to further research it, but first the article I promised previously, about inflammaging).
SARS-CoV-2 may be the most sugar-hungry beast ever studied.
If you choose to support my work at any point, thank you !

Hey buddy, speaking of liver problems i was just diagnosed with acute porphyria. Misery during those attacks followed by purple/black urine and neurological cascade.
Hey, we were chatting a lot on twitter.
I was the guy with Long Covid and a bunch of auto antibodies. Maybe you remember me.
I recently caught corona - and surprise surprise. It looks like I completely recovered. All my symptoms have vanished. Could it be my body got rid of the spike? Including the vaccine spikes?