If I needed any sign to write this substack, this would be it, this was the piece I intended to write yesterday, with this freshly published paper being the opening salvo.
The following will come as no surprise for anyone reading this Substack for a while.
This non-randomized controlled study examined adverse reactions, PRN (pro re nata) medication intake and inability to work after a fourth vaccination (i.e. second booster) among HCWs (healthcare workers) of the prospective CoVacSer study. All enrolled individuals previously had been administered an EMA-approved COVID-19 basic immunization, and a subsequent third, mRNA-based COVID-19 vaccination, defined as first booster vaccination. The second booster was performed with the monovalent BNT162b2mRNA vaccine or the bivalent BNT162b2mRNA original/Omicron BA.4-5 vaccine. Study participants administered with a different COVID-19 vaccine as second booster were excluded. As coadministration of COVID-19 and influenza vaccination might influence immunogenicity and side effects,[4] individuals receiving a simultaneous influenza vaccination were also excluded.
Results
76 HCWs received a fourth dose of COVID-19 vaccination between the 13th of August 2021 and the 14 th of October 2022 with either the original, monovalent BNT162b2mRNA (48.7%,37/76) or the bivalent BNT162b2mRNA original/Omicron BA.4-5 vaccine (51.3%, 39/76).
Our study focused on a direct comparison between the monovalent BNT162b2mRNA and the corresponding bivalent vaccine. In the light of preprints reporting inconclusive results in neutralizing antibody levels between the compared vaccines,[5-7] our results and further studies on safety and reactogenicity of bivalent COVID-19 booster vaccines are highly important to aid clinical decision making in the choice between bivalent and monovalent vaccinations.
This isn’t a massive paper, with copious amounts of evidence, but it adds to the continuously growing pile of evidence on how useless the mRNA vaccination is at the very least. Here a sizable portion of the healthcare workers who took the bivalent jab had worse reactions and missed more workdays than the monovalent ones. I do not even want to entertain what type of physiological and molecular damage is going on, but it is the same deduction we will find out later on because thank God the new bivalent booster is having a poor uptake.
Incidentally, this one was published in Nature days ago.
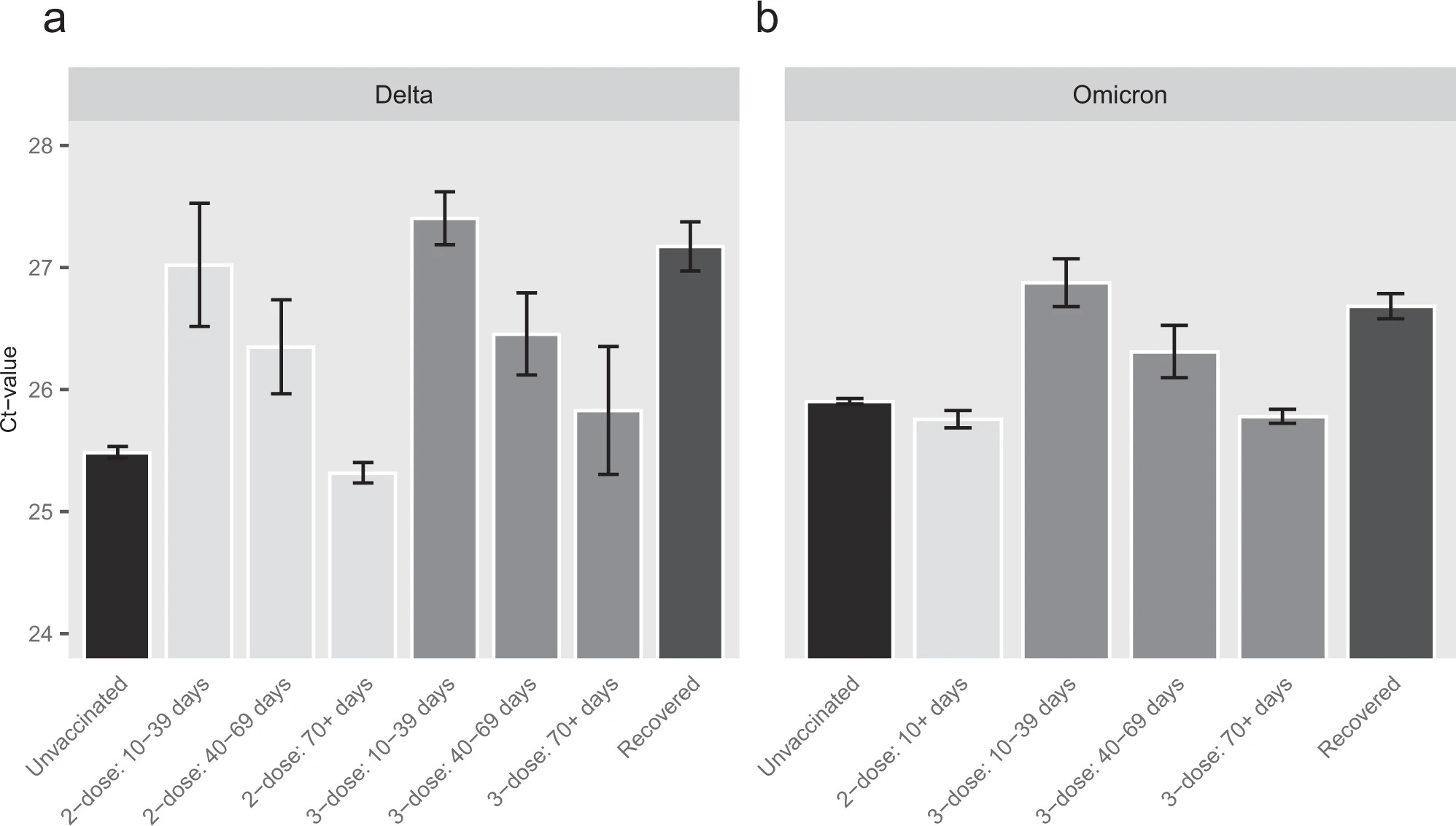
This study indicates that overall the presumed vaccination-related immunity to SARS-CoV-2 has only a negligible long term (>70-days) effect on Ct value, a common surrogate for VL and infectiousness. The combination of vaccine waning and vaccine evasion are most likely the drivers of this finding. In lieu of several prominent publications describing vaccine effectiveness in prevention morbidity and hospitalization for Omicron18,19,20, this study mandates reevaluating the role of current vaccination campaigns in harnessing the potential infectivity of COVID-19 at a time scale >2 months.
This is no small study, they analyzed the results of more than 460.00 individuals and measured viral load, and not antibodies, arguably a better overall metric for effectiveness than antibodies. When Delta was dominant the vaccinated had the advantage of lower viral loads for close to two months, decreasing almost weekly after that, and in many cases (not covered in this particular paper) reaching negative efficacy.
When faced with Omicron, there is particularly no difference because of both waning and immune evasion, between unvaccinated and up to 3 doses. 4 doses provided “some” protection and lower viral load for over 1 month, encountering the inescapable fate of waning after.
It is worth not that unvaccinated but infected with both variants (Delta+Omicron) had lower viral loads beyond 18 months, bringing the argument of early Omicron as a “natural booster”. A natural infection has minimal costs, and it is by far the best protection. I could argue that from any perspective we should have been out of the pandemic as a whole if not for the introduction of non-sterilizing vaccines. An argument made by everyone under the sun in 2021, and by me and others in mid-2020.
Further studies should assess the differential benefits of SARS-CoV-2 vaccines in alleviating disease vs. preventing pathogen spread. Should the lack of sterilizing immunity prove consistent, it may have major ramifications on global pandemic preparedness, vaccination rollout and medical inequity. The demonstrated short-lived immunity and rapid waning on one hand, combined with the limited impact on population on the other, may focus the need for boosters for high-risk groups only, with immediate impact on vaccination campaigns and public health measures upon disease resurgence.
The point of bringing both studies to light is not another “dunk” on the SARS-CoV-2, but awareness of how they fail, miserably, because…
Pfizer has a big pipeline of future mRNA vaccines, and one of the ones I most fear hitting the mark is the flu one. An mRNA flu vaccine will kill the broad immunity we have against influenza, and make it very narrow, locked down on certain epitopes, and the flu mutates like almost nothing else.
But the gravy train in the synthetic bio/biotech field shall not stop, and it will only increase, and we get this. As a personal note I would like to bring up the point that the Ebola vaccine below served to at least prove one of my points since the inception of the mRNA vaccine for SARS-CoV-2.
Poor CD8 stimulation or presence equals very poor neutralization and efficacy, exactly what the mRNA vaccine for SARS-CoV-2 did, basically negative CD8 for a good few months.
Emerging and re-emerging viruses, such as Zaire Ebola virus (EBOV), pose a global threat and require immediate countermeasures, including the rapid development of effective vaccines that are easy to manufacture. Synthetic self-amplifying RNAs (saRNAs) attend to these needs, being safe and strong immune stimulators that can be inexpensively produced in large quantities, using cell-free systems and good manufacturing practice. Here, the first goal was to develop and optimize an anti-EBOV saRNA-based vaccine in terms of its antigen composition and route of administration. Vaccinating mice with saRNAs expressing the EBOV glycoprotein (GP) alone or in combination with the nucleoprotein (NP) elicited antigen-specific immune responses. GP-specific antibodies showed neutralizing activity against EBOV. Strong CD4+ T cell response against NP and GP and CD8+ T cell response against NP were detected by ELISpot assays. Intramuscular vaccination with saRNAs conferred better immune response than intradermal. Finally, mice vaccinated in a prime-boost regimen with saRNAs encoding both GP and NP or with GP alone survived an EBOV infection. In addition, a single dose of GP and NP saRNAs was also protective against fatal EBOV infection. Overall, saRNAs expressing viral antigens represent a promising vaccine platform.
Mitochondrial diseases are one of the largest groups of neurological genetic disorders. Despite continuous efforts of the scientific community, no cure has been developed, and most treatment strategies rely on managing the symptoms. After the success of coronavirus disease 2019 (COVID-19) mRNA vaccines and accelerated US Food and Drug Administration (FDA) approval of four new RNAi drugs, we sought to investigate the potential of mitochondrion-targeting RNA-based therapeutic agents for treatment of mitochondrial diseases. Here we describe the causes and existing therapies for mitochondrial diseases. We then detail potential RNA-based therapeutic strategies for treatment of mitochondrial diseases, including use of antisense oligonucleotides (ASOs) and RNAi drugs, allotopic therapies, and RNA-based antigenomic therapies that aim to decrease the level of deleterious heteroplasmy in affected tissues. Finally, we review different mechanisms by which RNA-based therapeutic agents can be delivered to the mitochondrial matrix, including mitochondrion-targeted nanocarriers and endogenous mitochondrial RNA import pathways
Yang et al. established a novel type of circular mRNA called cmRNA. cmRNA contains an echovirus 29-derived internal ribosomal entry point element to promote ribosome binding and a newly designed spacer to enhance translation. Their findings suggest that this type of circular mRNA can mediate strong and persistent expression of various types of proteins. Furthermore, in addition to delivery via lipid nanoparticle (LNP), cmRNAs were discovered suitable for direct intratumoral administration. By giving mice cmRNAs encoding mixed cytokines directly intratumorally, they achieved successful modulation of intratumoral and systemic antitumor immune responses and enhanced anti-programmed cell death protein 1 (PD-1) antibody-induced tumor suppression.
These are a few examples of using synthetic forms of RNA for therapeutic goals, and as a “forecast” the mitochondrial one is rather prescient since the first ever mass-used mRNA product has the hallmark of causing mitochondrial dysfunction and mitochondrial-related diseases at alarming levels. And the cmRNA one for the “strong and persistent expression of various types of proteins.
To this day, nobody on the entire planet knows what the mRNA vaccines are producing, what type of proteins, translation fidelity, purity, and everything else. This is a very good video from a pharmacist I respect about the subject. And as a further reminder and a segway to our next subject, the following, in regards to mRNA. You can’t “fix” mRNA, because our bodies are genetically programmed to respond to it in the same way.
Proteomic surveys with top-down platforms are today revealing thousands of naturally occurring fragments of bigger proteins. Some of them have not functional meaning because they derive from pathways responsible for protein degradation, but many have specific functions, often completely different from that one of the parent proteins. These peptides encrypted in the protein sequence are nowadays called cryptides. They are frequent in the animal and plant kingdoms and represent a new interesting –omic field of investigation. To point out how much widespread is their presence, we describe here the most studied cryptides from very common sources such as serum albumin, immunoglobulins, hemoglobin, and from saliva and milk proteins. Given its vastness, it is unfeasible to cover the topic exhaustively, therefore only several selected examples of cryptides from other sources are thereafter reported. Demanding is the development of new –omic platforms for the functional screening of new cryptides, which could provide suggestion for peptides and peptido-mimetics with variegate fields of application
No person on the planet (except perhaps Leidos…) has any idea about the proteins and peptides being produced by the mRNA, nobody has any idea about the structure if there are added glycans, amyloid fibrils, or anything else, but above all else, nobody knows or is even testing the possibility and physiological function of the cryptic peptides (non-canonical peptides), and these sequences will have entirely different functions from the protein they originated from (especially if there are added molecules to the protein produced by mRNA).
You do not need a large amount of these peptides to have profound physiological effects. At this point, as a friend wrote to me, we are purely into experimental science without regard to anything else. There is no argument if this will backfire, the only honest argument is far this will backfire.
As I wrote for weeks, there are two sides of this that are completely ignored by almost everyone, regardless of expertise. First is glycobiology. The second is the non-canonical side of biology.
The mRNA technology was a good 10 years, perhaps 15 away from use in humans, and not only that, I heard from people responsible for scaling Pfizer’s own mRNA production, nowhere near even close to producing any meaningful quantities of the product.
I may write other things in between this piece, and the Cognitive Warfare piece, perhaps shorters or even longer ones, but do not be surprised if I go “silent” for a few days, even though I enjoy and like writing I must attend the funeral of a very dear friend of mine that recently passed away. And I want to make the Cog. War piece something fairly unique too.
I wish you all a good rest of the week. And as always a big thank you to subscribers who choose to support this Substack by paid subs or on Kofi, and everyone who shares these.
Things Hidden in Complexity is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
People reflexively get flu shots: Compellingly, you wrote:
"Pfizer has a big pipeline of future mRNA vaccines, and one of the ones I most fear hitting the mark is the flu one. An mRNA flu vaccine will kill the broad immunity we have against influenza, and make it very narrow, locked down on certain epitopes, and the flu mutates like almost nothing else."




Thank you JP and my condolences for your deceased friend. Too much grief.
Thank you and Doorless Carp!
People reflexively get flu shots: Compellingly, you wrote:
"Pfizer has a big pipeline of future mRNA vaccines, and one of the ones I most fear hitting the mark is the flu one. An mRNA flu vaccine will kill the broad immunity we have against influenza, and make it very narrow, locked down on certain epitopes, and the flu mutates like almost nothing else."