
Even more antigenic sin, T-Cell escape
And bivalent vaccine failure

Well, sometimes life has a funny way of sending a message, and the message is pretty clear and in line with much of the evidence for the last 18 months, and I said I would briefly cover these papers in a less sciency manner, they are all rather significant. I won’t bother referring to the very recent substack within this theme, they are all recent and easily accessible.
Antigenic sin of wild-type SARS-CoV-2 vaccine shapes poor cross-neutralization of BA.4/5/2.75 subvariants in BA.2 breakthrough infections

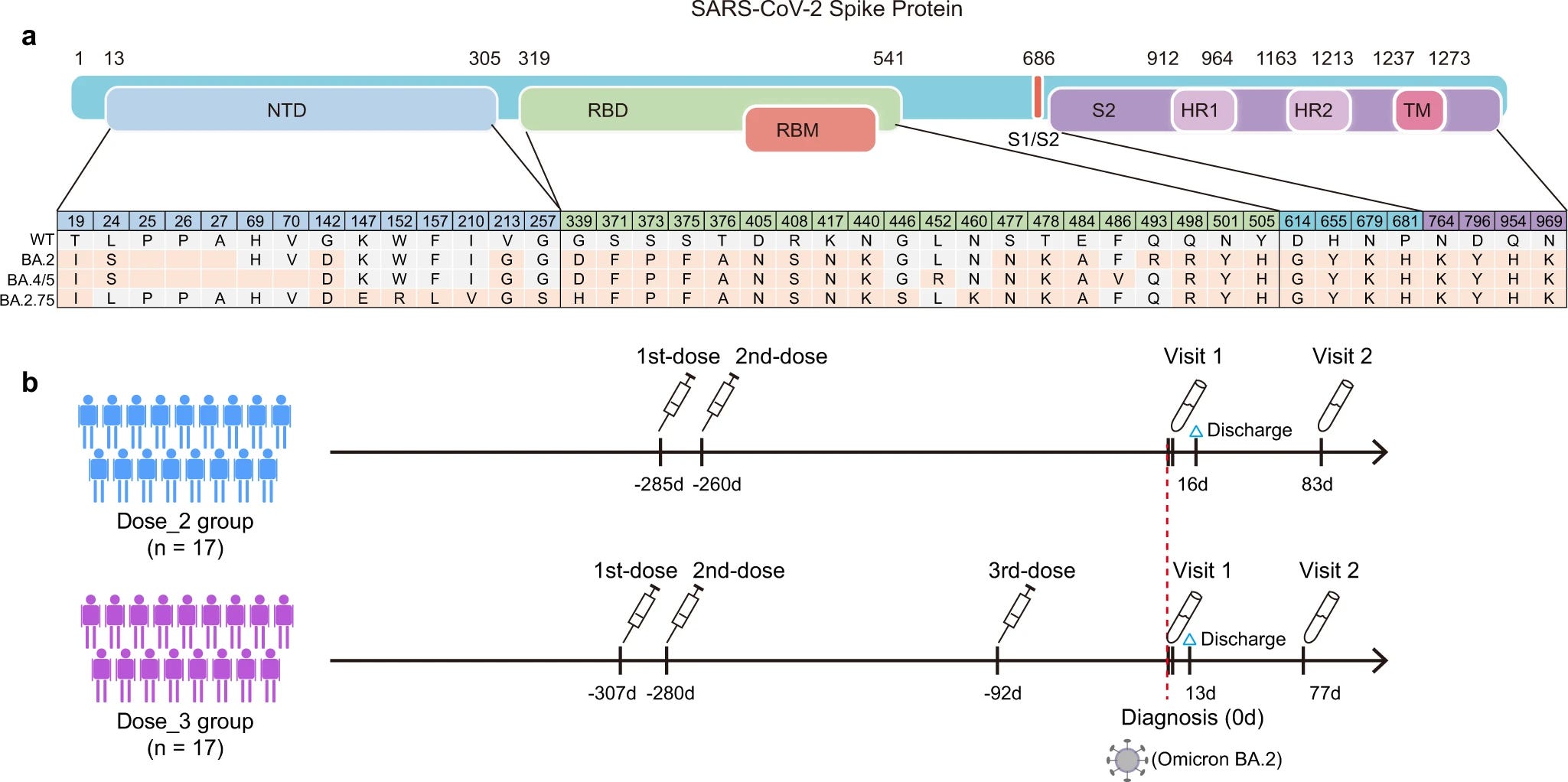
The sampling here is good, but your focus is and should be the mutations, save the image or mark them down, even if you don’t understand molecular biology, it will serve you well as the years go by.
Trying to clarify what exactly goes on at a neutralization level and find if the antibodies the immune system produces which are aimed, or “fixated” in the Wuhan virus/spike protein the authors found that after a long enough period, the majority of the group in the study were not able to neutralize the virus, and none against Omicron. 2 doses vaccinated maintained a decent neutralization rate against Wuhan, but fall by 30% against BA. 2 and further falls against BA. 4/5 and 2.75 (average of 23% against these last ones), neutralization capacity was rescued and enhanced after a BA. 2 infection. What has been referred to months ago as a “natural booster” from an\ Omicron infection.
Together, these results demonstrated that the current immune barrier established by vaccination or vaccination plus the BA.2 breakthrough infection would be severely challenged by recently emerging Omicron subvariants.
These findings indicated that the BA.2 breakthrough infection mainly induced cross nAbs against the WT virus and poorly elicited Omicron-specific nAbs in prototype vaccine recipients.
While not exactly the correct scientific term, this is what one could refer to as antibody saturation, and another “lie” or misconception being proven wrong again, the body can’t “update” its antibodies and effectively fight the viral infection even when someone goes through a breakthrough infection, which is precisely the argument the author’s raise in the discussion section.

The now self-evident truth presents itself yet again, and building more evidence of OAS is necessary judging by the continuous “discussion” among the experts and both sides of this overly political conversation now. Given that antibodies were the basis of this entire debacle even vaccine pushers such as Bill Gates are now changing their tune, from pushing vaccines or drugs (antivirals) to inhalable inhibitors…
Months ago other researchers pointed out that there was already a need to change vaccine design precisely by what is discussed in this substack for the most part of this month and in the closing paragraph, there is a degree of “hopium” written. Many experts argue a change in design and using different epitopes or other immunogenic-specific parts of the virus will be enough to deal with the next variants. (Spoiler alert: it won’t, only early treatment will).
Antibodies can’t be endlessly produced and their quantity and neutralization capacity increased with this class of virus, so a few would argue “T cells got our back, bro”. Do they though ?
SARS-CoV-2 Omicron BA.4/BA.5 Mutations in Spike Leading to T Cell Escape in Recently Vaccinated Individuals
SARS-CoV-2 Omicron (B.1.1.529) lineages rapidly became dominant in various countries reflecting its enhanced transmissibility and ability to escape neutralizing antibodies. Although T cells induced by ancestral SARS-CoV-2-based vaccines also recognize Omicron variants, we showed in our previous study that there was a marked loss of T cell cross-reactivity to spike epitopes harboring Omicron BA.1 mutations. The emerging BA.4/BA.5 subvariants carry other spike mutations than the BA.1 variant. The present study aims to investigate the impact of BA.4/BA.5 spike mutations on T cell cross-reactivity at the epitope level. Here, we focused on universal T-helper epitopes predicted to be presented by multiple common HLA class II molecules for broad population coverage. Fifteen universal T-helper epitopes of ancestral spike, which contain mutations in the Omicron BA.4/BA.5 variants, were identified utilizing a bioinformatic tool. T cells isolated from 10 subjects, who were recently vaccinated with mRNA-based BNT162b2, were tested for functional cross-reactivity between epitopes of ancestral SARS-CoV-2 spike and the Omicron BA.4/BA.5 spike counterparts. Reduced T cell cross-reactivity in one or more vaccinees was observed against 87% of the tested 15 non-conserved CD4+ T cell epitopes. These results should be considered for vaccine boosting strategies to protect against Omicron BA.4/BA.5 and future SARS-CoV-2 variants.

Many of the mutations present in BA. 4, BA. 5, and the new ones such as 2.75 and XBB (the current dominant variant) effectively negatively impact T cell responses towards the virus, and if you read the piece Repeated RBD boosting, you will understand why this is such a big deal.
Both from antibodies (B cell) and T cell perspective, multiple vaccinated individuals are having a continuously harder time dealing with and clearing Covid infections, leading to persistent symptoms, and persistent low-level inflammatory responses and damage, which taxes both their bodies and their capacity to keep any opportunistic pathogen at bay. The antibodies aimed at SARS-CoV-2 also lose their polyfunctionality, meaning they lose their efficacy and how well they can deal with the Spike and virus.
As I wrote earlier this week, we are out of in-for-a-penny, and getting into the in-for-a-pound stage, a bet the world made unwillingly, yet all pay the price. While there is a substantial difference between “natural” immunity and “vaccine” derived immunity, the virus is converging and becoming a long-term problem. Which, by all evidence so far, and ever since 2020 SARS-CoV-2 itself doesn’t kill, but whatever comes next does, especially without proper treatment.
What I mean by the long-term problems are the low-grade immunological, microbiome shift, and other subclinical changes, dozens of the pathways I wrote about and others come into play. Such changes create the following problem for millions of people.
Waning Immunity Against XBB.1.5 Following Bivalent mRNA Boosters
The SARS-CoV-2 Omicron variant has continued to evolve. XBB is a recombinant between two BA.2 sublineages, XBB.1 includes the G252V mutation, and XBB.1.5 includes the G252V and F486P mutations. XBB.1.5 has rapidly increased in frequency and has become the dominant virus in New England. The bivalent mRNA vaccine boosters have been shown to increase neutralizing antibody (NAb) titers to multiple variants, but the durability of these responses remains to be determined. We assessed humoral and cellular immune responses in 30 participants who received the bivalent mRNA boosters and performed assays at baseline prior to boosting, at week 3 after boosting, and at month 3 after boosting. Our data demonstrate that XBB.1.5 substantially escapes NAb responses but not T cell responses after bivalent mRNA boosting. NAb titers to XBB.1 and XBB.1.5 were similar, suggesting that the F486P mutation confers greater transmissibility but not increased immune escape. By month 3, NAb titers to XBB.1 and XBB.1.5 declined essentially to baseline levels prior to boosting, while NAb titers to other variants declined less strikingly.
The combination of low magnitude and rapidly waning NAb titers to XBB.1.5 will likely reduce the efficacy of the bivalent mRNA boosters5 , but cross-reactive T cell responses, which were present prior to boosting, may continue to provide protection against severe disease.
As I warned very early, before XBB was even “a thing”, with all the evidence and an in-depth analysis of the immunological response of the Omicron Spike, especially significant changes when used as a “vaccine target”, the bivalent booster would fail fast, and this was merely by these dynamics, not taking into account the shift in mRNA elicited immunity, the deep changes in B cells, T cells dynamics and others.
A bundler from the start, and as we just covered, while some of the T-Cell response is maintained, the continuous usage of poorly functional drugs and vaccines driving mutations in the virus is leading to a certain level of T-Cell escape.
If you are, or know someone vaccinated, you or that person should take a lot of care of their health, the unvaccinated too, but the vaccinated need double or triple the care, of this moment your problem won’t be pneumonia, but invasive, aggressive fungal and bacterial infections, but above all else for certain genetic types, autoimmunity. The coming explosion of autoimmunity, which a certain subset of “influencer” will attempt to pindown solely on the mRNA or Spike, will actually not be caused by both, they are merely the first hit (and run).
Clearing your body of the virus, and keeping the immune system as functional as possible, making the time your body takes to recover from the infection shorter will definitely help and avoid any of the more daring outcomes.
But I digress, these are both subjects (sepsis, autoimmunity) for other substacks, way longer, and more complex, which I am postponing until I feel like writing about them.
I won’t explain why, how, the mechanism, the pathway, or even allude to it, but if you are vaccinated, you should 100% get into Berberine or Metformin as soon as you are able. Not optional. Take it or leave it, any comment about this section of this substack will be summarily deleted. Advise the unvaccinated to add these too.
I appreciate the support of those who choose a paid subscription, or who decide to buy me a coffee whenever they feel like it, and everyone who shares my Substack. This work wouldn’t be possible.
This one took longer even though it is not sciencey because I have been going through a massive headache for the last 48 hours 😆 😭 lol.
Thanks for the great posts, I have added Berberine to my list (also NAC) to my list just a few weeks ago, expecting to be confronted with the new escape variants very soon.