

Disease acceleration, nuclear receptor and a common denominator
Disease acceleration, nuclear receptor and a common denominator
"The Nuclear Option"

Highlights of this article:
We have more evidence the Spike Protein contributes to the acceleration of certain diseases via Th17 immune response
Doesn’t matter the type of vaccination, a breakthrough infection may induce Th2 (allergic) and Th17 responses
Natural infection does both of the same described above
A nuclear receptor downregulated by the virus, downregulated in Long Covid is responsible for keeping Th17 in check
All roads lead to Rome
The vast majority of the time I follow a schedule. An absurd amount of hours spent on research, then hours poured into writing. In rare moments we have articles like the last one, sudden because of the nature of the news, and others, articles like this one. Based on gut instinct, waking up “inspired”, or touched by God. Choose whatever makes you feel more comfortable with my work, but all 3 play a significant part.
Here we are going to touch on some complex topics. We start from the big one and go tracing the pathway…somewhere. It is no mystery that one of my biggest scientific interests, especially after the start of the pandemic has been the subset of T Helper cells called Th17.
T Helper cells (Th cells) are one of the most important aspects of our immune system, they orchestrate a large portion of your immune response against anything. Th17 cells are an essential part of your immune response too, but they are the perfect example of “too much of anything” being bad and the delicate balance of the immune system. When the balance is broken or for a paradoxical reason your body produces too much of these, you get highly inflammatory conditions, autoimmunity, the “usual”.
While Th17 cell biology is very complex, the best way to explain would be “Necessary, but sometimes a last-ditch effort of the body to deal with an infection, which can cause problems if persistent.” If you use my Index article you can find most of my Th17-centric articles, or click here for the search query finding all articles mentioning Th17.
SARS-CoV-2 spike protein accelerates systemic sclerosis by increasing inflammatory cytokines, Th17 cells, and fibrosis
Systemic Sclerosis is mostly commonly known as “Scleroderma”, an autoimmune condition when your body attacks your tissues, from the skin to your blood vessels, and induces fibrosis on all organs (your skin is your biggest organ). It causes vascular permeability and this makes your cells enter places they shouldn’t, causing damage that induces scars (which in turn becomes fibrosis).
Similar to the last study, this study has some “caveats”. Their first test was over-expressing (making the cells produce a lot more than normal) the Spike Protein in HEK293 cells, and measured the impact it had on ACE2, and per all the evidence we have, lots of Spike = fewer ACE2, in turn, proteins related to fibrosis such as alpha-SMA and Col1a1 were upregulated.
Next, they used mice lacking ACE2 and induced skin fibrosis by injecting bleomycin, an antibiotic so absurdly toxic it is used to kill cancer cells (and in mice, it can induce fibrosis). After injecting the mice with plasmid DNA encoding human ACE2 and Spike protein, they observed an increase in anti-phospholipid antibodies, this type of autoantibodies can cause clots. And here is the actually important section.
Furthermore, we detected an increase in the levels of total IgG in the serum of the group immunized with the protein (Fig. 2D). After 5 weeks, we analyzed the proportions of Th2 and Th17 cells in the peripheral blood via flow cytometry (Fig. 2E). We observed an increase in Th2 and Th17 cells in the group injected with the spike protein, indicating heightened immune system activation and autoimmune symptoms.
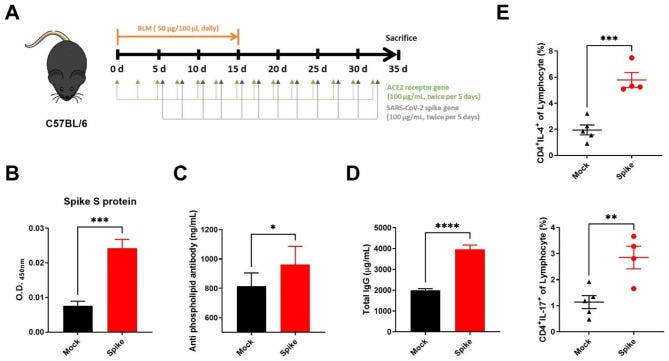
Timing is everything, and one can (and many pro-mRNA vaccine researchers did knowingly or not) game cells expressed in any type of sample, cell line, or test. Th17 cells always come late to the party in a lab, and here they found that after weeks, there was a shift towards Th2 and Th17 responses, measured by IL-4 for the first, and IL-17 for the latter.
Next, they used microscopy to see if there was lymphocyte infiltration in skin and lung tissue, and the group of mice injected with Spike Protein had greater infiltration of Th2 and Th2 cells in the lungs and skin.
Similar to some adverse events where skin conditions deteriorated at an accelerated pace as an adverse reaction to the mRNA or the adenovirus vaccine, the Spike Protein accelerated fibrosis. It does so by increasing inflammatory proteins such as IL-6, IL-4, IL-17, TNF-Alpha, and IL-1Beta. This also happens with the natural infection.
As further evidence, here is another study measuring inflammation and vascular damage markers after the mRNA vaccine in patients with thymic epithelial tumors.
This evidence supports the hypothesis that COVID-19 inflammation and cytokine release are related to activated T-lymphocytes, particularly Th1 and Th17, as we observed either in acute COVID-19 [18] and in multisystem inflammatory syndrome in children [19, 20], and later in patients with TET following the vaccine [11].
This is not merely repeating myself, just more evidence of what has been obvious for a few years, but I am also going somewhere here. For the past 2 to 3 months I kept referring to Omicron’s immune response, something I was sorely lacking on examing like the other subjects I do.
It is arguable by many perspectives that the IL-17 and Th17 response present in the mRNA vaccines are a byproduct of Endotoxin exposure and contamination, given the Spike itself can interact with those too, as you can see here where Omicron infected mice only increased their IL-17A, IL-22, and IFN-γ by exposure to LPS. But…
At this point, my perspective is that the virus and Spike Protein have an intrinsic Th17 response in regards to vaccination, regardless of the type of vaccine, mRNA, Adenovirus, inactivated, it always ends up converging into a similar response. This a perspective the authors share, because here they tested different formulations in regards to different types of vaccine, and while during vaccination the immune response is what “you expect it” after the breakthrough infection you get a Th2-biased response followed by systemic Th17.
Immune responses are insanely complex, the genes involved, the regulation of genes even more so. Sometimes signals present themselves, and you will only make sense of something months down the line, even after spending a considerable amount of time researching that “single thing”.
The friend I often refer to as being the person I collaborated with had a major criticism while still present online, including towards me, and he was correct. “Nobody is looking at what is happening at the nucleus (of the cell).” Nuclear Receptors (NR) are found inside the cell, around the nucleus and they are incredibly important because they can regulate gene expression, which cascades into significant changes inside and outside the cell.
I spent a considerable amount of time researching one of these NRs, even though there was little published evidence in regards to the role of one specific receptor concerning SARS-CoV-2, although I was aware Pfizer was pumping millions of dollars into solving this specific research avenue. But as I said at the start of this article, sometimes everything just clicks.
What started connecting the dots and made me look in retrospect at the paper cited above is this paper on Long Covid, “Persistent complement dysregulation with signs of thromboinflammation in active Long Covid”, here is an article that is very friendly to most readers. Among the many important findings, the one I paid the most attention to was the researchers finding low-expression levels of NR4A1 in the monocytes of Long Covid patients.
The receptor in question is called NR4A1 (also referred to as Nurr77). Going back to 2022, a group of researchers did a comprehensive analysis of how SARS-CoV-2 escaped our immunity and found it did so by destroying mitochondrial quality, and the body itself contributed to the inflammatory response by “eating” infection alveolar epithelial cells thus starting an inflammatory reaction via the ROS-HIF1A (hypoxia and excessive oxidative stress), inducing cytokine storm by affecting T-Regulatory cells. Among the genes downregulated was NR4A1.
If Nuclear Receptors are highly complex, NR4A1 goes further into fully paradoxical function. It can possess distinct effects in the same type of cells depending on what is around the cell, and where inside the cell it finds itself. It is incredibly important for T-cell function. Ironically, they are very important when it comes to T-Reg cells, the regulatory cells of the immune system, and absurdly important to keep Th17 in check…
Another paper.
Here using an NR4A1 agonist called cytosporene B the researchers were able to decrease the production of Interferon-Gamma and Interleukin-17 by Th1 and Th17 in the central nervous system.
Clearly, NR4A1 is incredibly important for immune homeostasis, keeping the immune system in harmony, and equilibrium. I am reminded of what the same friend said “This thing must be flipping a very important switch that can cause all of this”, while I don’t think I found the switch, I do have the instinct this one is among the most important ones.
Unregulated, systemic Th17 responses are implicated in many autoimmune diseases, neurodegeneration, depression, psychological conditions, bone-related diseases, and organ diseases, so mitigating this response was, and still is my primary goal. In case you forgot, my suggested supplements take care of this but the most effective ones are Vitamin D and Thiamine (Vitamin B1). Simple, beneficial, no fuss no muss.
Long-term implications rather than short-term effects are what you should take from here.
This is me when you are or become a paid subscriber or the article helps you.

I wish everyone a great weekend. Hope it is a chill or a productive one.
My energy and cognitive tanks are empty so no snark comments this time =P. How are you spending your weekend ?
Love you bro, there isn’t a day I don’t thank Jesus and the blessed mother for you. Keep up the good work and God bless you homie.