

Vaccine induced Th17 response - Further evidence for paradoxical immune response
Vaccine induced Th17 response - Further evidence for paradoxical immune response
And the superiority of Live Attenuated Vaccines.

Good evening, hope you all had a very nice day this Sunday. I was surprised to find this recently publish pre-print yesterday, and have to cover it. It is incredibly meaningful.
To understand why this has importance, you should read at least both of the pieces below, but most likely all of the ones linked, since this is one singular (big) theory. This piece obviously will touch on many subjects I covered both now, and before.

To be clear to the reader (and arrogant to annoy certain…people), I was among the first to point out and find parts of the mechanisms of how SARS-CoV-2 could be chronic and I was the one who first equated AIDS with the vaccine, and this has nothing to do with AIDS, it was for the “stickiness” of the meme.
It is immune DYSFUNCTION, not a deficiency. (I make this clear in these pieces)
It has nothing to do with AIDS, period.
The paper below was done on cancer patients, but it applies broadly to a huge percentage of the vaccinated population.
Profiling of immune responses to COVID-19 and vaccination uncovers potent adjuvant capacities of SARS CoV-2 infection to vaccination leading to memory T cell responses with a Th17 signature in cancer patients

The abstract is rather simple to understand, and something other researchers found too. Even a vaccine solely fixed on using the S protein generates a poor T cell response against the S itself compared to a natural infection, and only after being infected (before the vaccination or breakthrough infection) does the response becomes sufficiently broad and potent enough.
Also interesting that your body will focus on M and S protein, and not on the N when you are naturally infected, but as I wrote before, the response against the N protein is necessary to clear the virus, especially after your body “kills it”.
That is why some people have persistent low-grade inflammation, and can keep testing positive.
And here we have, the vaccines elicit an elevated IL-17 CD4-based response with plenty of neutrophils, these neutrophils can be used, under certain circumstances and conditions to “infiltrate” tissue and set off the different types of diseases and damage you see around sometimes.
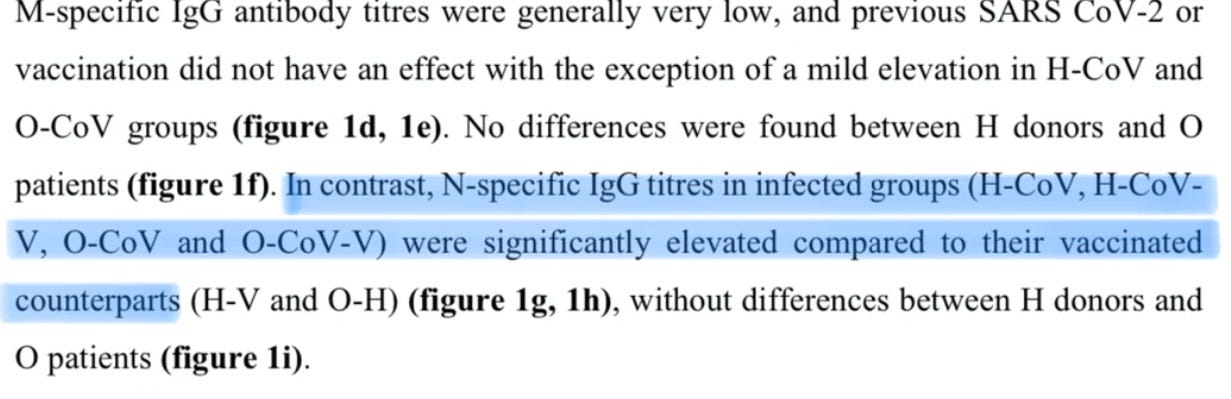
Same as I wrote above. N-specific IgG (a type of antibody) was substantially higher in infected people than the vaccinated ones.

The previous infection elicited an Interferon-gamma CD4 response which is complete to be expected since your body needs IFN-y to fight and clear infections and fight pathogens, the problem is always “excess” of it, not solely having a response.
The highlighted part is the most important one, again, more proof that Spike Protein is what is driving this abnormally strong Th17 shifting and highly inflammatory response. Authors note that cancer patients had stronger inflammatory responses than healthy people, which depending on cancer, is “normal”, and this right here is why I called it “disease acceleration” and not “THE SPIKE CREATES ALL DISEASES IN THE HARRISON’S INTERNAL MEDICINE BOOK”.
Under certain conditions, the virus, and absolutely the vaccine will accelerate a lot of diseases, autoimmunity, and cancers. It might turn some of the dormant genes on and set diseases off too.
The good news, this inflammatory response diminishes progressively after 6 months of vaccination. Did you get now why your body is trying to get rid of vaccine-elicited antibodies so fast, the more times go by, the more you boost and new variants pop up ?
The human body is the most amazing, complex self-regulating machine in nature.
One of the main arguments used by the vaccine zealots very early in the pandemic and the push towards Spike-centric vaccines (both the adenovirus and mRNA ones) was the body does not need a CD8 response to fight the infection and long-term immunity. Which was always a lie, and a clearer lie by the day. Only a natural infection (vaccinated or not) will give you that memory, long-term CD8 response. Vaccines will only give you an effector (short-term) immune response.
Vaccines also fail to elicit an M response, which to the author’s findings, is a potent part of the immune response and cross-reactive (this specific part of the virus doesn’t mutate much among all the coronavirus family). Well, I know it might sound obvious, alas they need to test it.\

To my surprise, vaccination alone was not a potent inductor of S-specific CD4 T cell response, only if you were previously infected, so now we have even more of a bullshit thread to pull from Pfizer's long list of trial manipulation.
The N protein was also a poor inductor of T Cell response in both healthy and cancer patients, and the authors argue that it requires natural infection and vaccination to expand it… I know what you are thinking, but the authors NEED to push the vaccines otherwise they will never get published anywhere, nor get grants to actually research.
Won’t blame them, but that is why you need to interpret, cross reference, and be careful with all papers.
As some of us said for over 2 years, they should have used other parts of the virus even using novel technology. Here they find that the M protein has a substantially stronger CD8 response than the Spike, which mostly produces CD4. This has been my argument for a year and very few could accept it.
And here we have more proof that the vaccines heavily shift your immune response towards Th2, and induce an IFNy response with high levels of IL-17, both markers for a dominant Th17 response. They can both coexist in an “allergic” scenario (what is autoimmunity again?). Infection, as I wrote quite a number of pieces on, also induces a Th17 response, and my argument was always this was driven by the Spike protein, and its abnormally capacity to bind to all receptors known to man.
The last highlighted part speaks for itself, and clearly shows how some people get accelerated (sometimes at alarming speeds) cancers. Following is a paper I would cover alone but will cover here in a short format.
A live attenuated vaccine confers superior mucosal and systemic immunity to SARS-CoV-2 variants
Vaccination alleviates clinical symptoms and reduces virus load
All vaccines used here protected animals from the considerable body weight loss that is typical for SARS-CoV-2 infection of Syrian hamsters. At the same time, vaccine regimens involving sCPD9 displayed a trend towards improved protection compared to other vaccines based on body weight loss.
Following a single vaccination, none of the vaccines completely prevented infection by SARS-CoV-2 Delta as evidenced by the detection of viral RNA in both the upper and lower respiratory tract of all animals. However, on day 2 post challenge, sCPD9 vaccination diminished replicating virus to undetectable levels in the lungs; a feature none of the other groups exhibited
In this model, a single dose of any vaccines (they tested mRNA, Adenovirus, and their LAV one) didn’t prevent the infection with Delta, however on Day 2 after infecting the hamsters, their LAV lowered the amount of replicating virus in the lungs to levels that could not be detected, something no vaccines to this day does, in any form.
LAV is superior in preventing inflammatory damage to the lung
We found that after single vaccination, sCPD9 prevented inflammation and pneumonia more efficiently than other vaccines
Notably, for the mRNA+mRNA regime, most detectable viral RNA appeared in macrophages. Since virus uptake in macrophages causes their transcriptional activation, this can explain more abundant expression of pro-inflammatory genes in macrophages of mRNA+mRNA animals compared to those of sCPD9+sCPD9 vaccinated animals. Consistently, all effects were most pronounced after double sCPD9 vaccination, which could indicate that this strategy is also very successful in reducing the strong inflammatory responses that are responsible for both acute and long-term damage caused by SARS-CoV-2 infection.
This was a finding that was particularly interesting to me. One of the remarkable effects SARS-CoV-2 (the virus) and the Spike-centric vaccines have is the strong inflammatory response they elicit, especially in regards to macrophages. It is one of the driving forces of long-term low-grade inflammation. Which this live attenuated vaccine didn’t have as a feature.
LAV induces superior mucosal immunity against SARS-CoV-2
In addition to potent T cell memory and humoral immunity, induction of protective mucosal immunity is a distinguishing property of LAVs that are administered locally at the natural site of virus replication. However, in case of SARS-CoV-2, induction of limited mucosal antibody responses following mRNA vaccination is reported.
We found that sCPD9 vaccinated animals harbored considerably larger quantities of IgA in nasal washes prior challenge and at all tested time points post challenge . Notably, challenge infection further boosted levels of SARS-CoV-2 spike-specific IgA antibodies in sCPD9-vaccinated animals and induced detectable quantities in mRNA- and Ad2-vaccinated animals, albeit with clear differences in favour of sCPD9 vaccinees at all time points.
Taken together, we provide evidence that sCPD9, the live-attenuated vaccine employed here, provides superior protection against SARS-CoV-2 in both the lower and upper airways, making it a promising candidate for further investigation in clinical trials.
As I covered in a recent post (Reasons for vaccine failure against Omicron), this is one of the main reasons the vaccines do not protect against infection and transmission, because they can’t elicit a proper IgA in your mucosa, the first barrier against any respiratory viruses.
Why am I posting this one here ? Two reasons, with another post I want to make and fits my following argument.
This is exactly what Omicron does to the unvaccinated, and to a minor degree to the vaccinated, and this is what the new variants, even though they “escape immunity” will do to many people.
A live virus is the best way to acquire immunity, and as long as you take certain precautions (supplements, everything I covered so far), it should be completely fine.
(Everything I covered so far…mostly)
Thanks for this continuing thread on the mechanisms of vaccine side effects. 👍🏼👏 I'm getting what's your saying, how this immune system dysregulation leads to problems in so many areas of the body. Versus the amyloid and prion theory that would affect so many areas of the body.
I know you chose the name reverse AIDS because of stickiness. Every time I hear it though I get a little confused, and feel like I need to understand it all over again. This is play because I don't have enough of an understanding of the immune system, and I've watched a few videos today to understand a little more. It's my understanding simplistically, AIDS depletes CD4 cells so the immune system is severely hampered in fighting any infection (generally CD4 cells are helper T cells and activate other parts of the immune system).
So the vaccine reduces CD8 + t cells (which has many effects that you've pointed out), which are the cells that kill pathogens and cells infected with pathogens (and have formed memory T cells). I just can't get it in my brain how in any way "reverse AIDS" applies to this process. I guess the only way I can think of it is that CD8 cells are reduced rather than CD4 cells. Was that your thinking and calling it reverse aids? Or is there something else I can understand that won't throw me off?
Thank you for this John Paul. Is it possible that a low level inflammation state leads to weight gain?