
The misguided hope of updated vaccines
And the myo/pericarditis mRNA thingy...

The problem with doing things how I do, the system I built over the years is, that sometimes you keep stumbling on certain words, biochemicals and pathways, and out of nowhere, it will click. And you are deep into a rabbit hole.
I am also not happy with the quality of all the other current virus-related posts I am working on, so this will make do this weekend. Consider it homework…
This will be a mixed bag of some sort. A few days ago, the video below went viral on all social media, and here in Substack too, you are probably aware of it and have watched it multiple times. In case you didn’t.
Dr. Birx Says She Knew of Natural COVID-19 Reinfections as Early as December 2020
The quote that jumps to the eyes and ears is the same. The vaccine zealots HOPED the vaccines would work as they purport to. Most people with some intact common sense were aware of such a thing. Watch the video, but not the focus of this one.
A tweet from yesterday, my superficial opinions on the matter of this video.
Earlier today, in the morning, Pfizer from its benevolent intent release this.
Pfizer and BioNTech Announce Omicron-Adapted COVID-19 Vaccine Candidates Demonstrate High Immune Response Against Omicron
“As we’ve said since the early days of the pandemic, we will follow the science and adapt our own approaches as needed to help address COVID-19 as the virus evolves,” said Albert Bourla, Chairman and Chief Executive Officer, Pfizer. “Based on these data, we believe we have two very strong Omicron-adapted candidates that elicit a substantially higher immune response against Omicron than we’ve seen to date. We look forward to discussing these data with the scientific community and health authorities so we may rapidly introduce an Omicron-adapted booster as soon as possible if authorized by regulators.”
Moderna did the same 3 days ago.
MODERNA ANNOUNCES BIVALENT BOOSTER MRNA-1273.214 DEMONSTRATES POTENT NEUTRALIZING ANTIBODY RESPONSE AGAINST OMICRON SUBVARIANTS BA.4 AND BA.5
In today's data, mRNA-1273.214 boosted neutralizing titers against BA.4/BA.5 by 5.4-fold (95% CI: 5.0, 5.9) above baseline in all participants regardless of prior infection, and by 6.3-fold (95% CI: 5.7, 6.9) in the subset of seronegative participants. Neutralizing titers against BA.4/BA.5 were approximately 3-fold lower than previously reported neutralizing titers against BA.1. One month after an mRNA-1273.214 booster, neutralizing geometric mean titers (GMT) against BA.4/BA.5 were 941 (95% CI: 826, 1071) in all participants, and 727 (95% CI: 633, 836) in seronegative participants. For context, prior studies of a third dose of the prototype booster induced neutralizing GMT against BA.1 of 629 (95% CI: 526, 751) and against Delta of 828 (95% CI: 738, 928)[1]. A third dose of the prototype booster was shown to be effective against Delta and BA.1 infection and hospitalization in observational studies [2],[3].
Of course, both companies are still using the, forgive my french, bullshiting antibody levels as a measurement of “efficacy”, and titer levels. The following article has all the necessary information for you to understand this.

In specific, this paper in which Omicron Spike fails to elicit a proper immune response. The following comes from my Twitter.
Pfizer now has "tweaked" the jab for Omicron, the question is what the fuck did they change or add since Omicron doesn't work as a vaccine candidate. Also a reminder Omicron is dead, you need BA. 4 and 5 updated jabs. That will drive the evolution further.
The cycle repeats itself until this thing gets out of hand, and uses non-neutralizing antibodies to opsonize cells and create a cascade of inflammation and cytotoxicity.
The original spike had SEB and 15 other pathogens "parts" as an adjuvant, that is why "it worked". What the hell did they substitute the SEB for ? Since the SEB got attenuated in Omicron.
So many questions. They will pull some bullshit I am absolutely sure

From the get-go, the vaccine is already somewhat useless because it is using Omicron (BA. 1) Spike protein, which by all the evidence, is very antigenically different from BA. 4 and 5. The question that online time, molecular investigation, and clinical evidence will tell will be what did they change in the Spike Protein structure to “work” ?
Safe bet (from my perspective) they further messed with Toll-Like Receptor, and they change the Lipid NanoParticles recipe (chemical structure, chemicals used, among other things) to fake once again their “high level of antibodies” upon infection.
I will not divulge how I know, but I bet everything I have they either went full in Th17 territory or completely reversed the response of their previous vaccination. This isn’t a gut feeling or insight. It is from my own experience.
Before going further, a few clues from my Twitter page, months ago.



You should read both of the following posts (and the papers analyzed inside) even if you need to read them 3 times. They will be worth the time investment in the coming months. If you read them, and my Omicron pieces, you will understand where I am coming from, and going to.
Now to a fresh of the press paper.
Age and sex-specific risks of myocarditis and pericarditis following Covid-19 messenger RNA vaccines
Cases of myocarditis and pericarditis have been reported following the receipt of Covid-19 mRNA vaccines. As vaccination campaigns are still to be extended, we aimed to provide a comprehensive assessment of the association, by vaccine and across sex and age groups. Using nationwide hospital discharge and vaccine data, we analysed all 1612 cases of myocarditis and 1613 cases of pericarditis that occurred in France in the period from May 12, 2021 to October 31, 2021. We perform matched case-control studies and find increased risks of myocarditis and pericarditis during the first week following vaccination, and particularly after the second dose, with adjusted odds ratios of myocarditis of 8.1 (95% confidence interval [CI], 6.7 to 9.9) for the BNT162b2 and 30 (95% CI, 21 to 43) for the mRNA-1273 vaccine. The largest associations are observed for myocarditis following mRNA-1273 vaccination in persons aged 18 to 24 years. Estimates of excess cases attributable to vaccination also reveal a substantial burden of both myocarditis and pericarditis across other age groups and in both males and females.
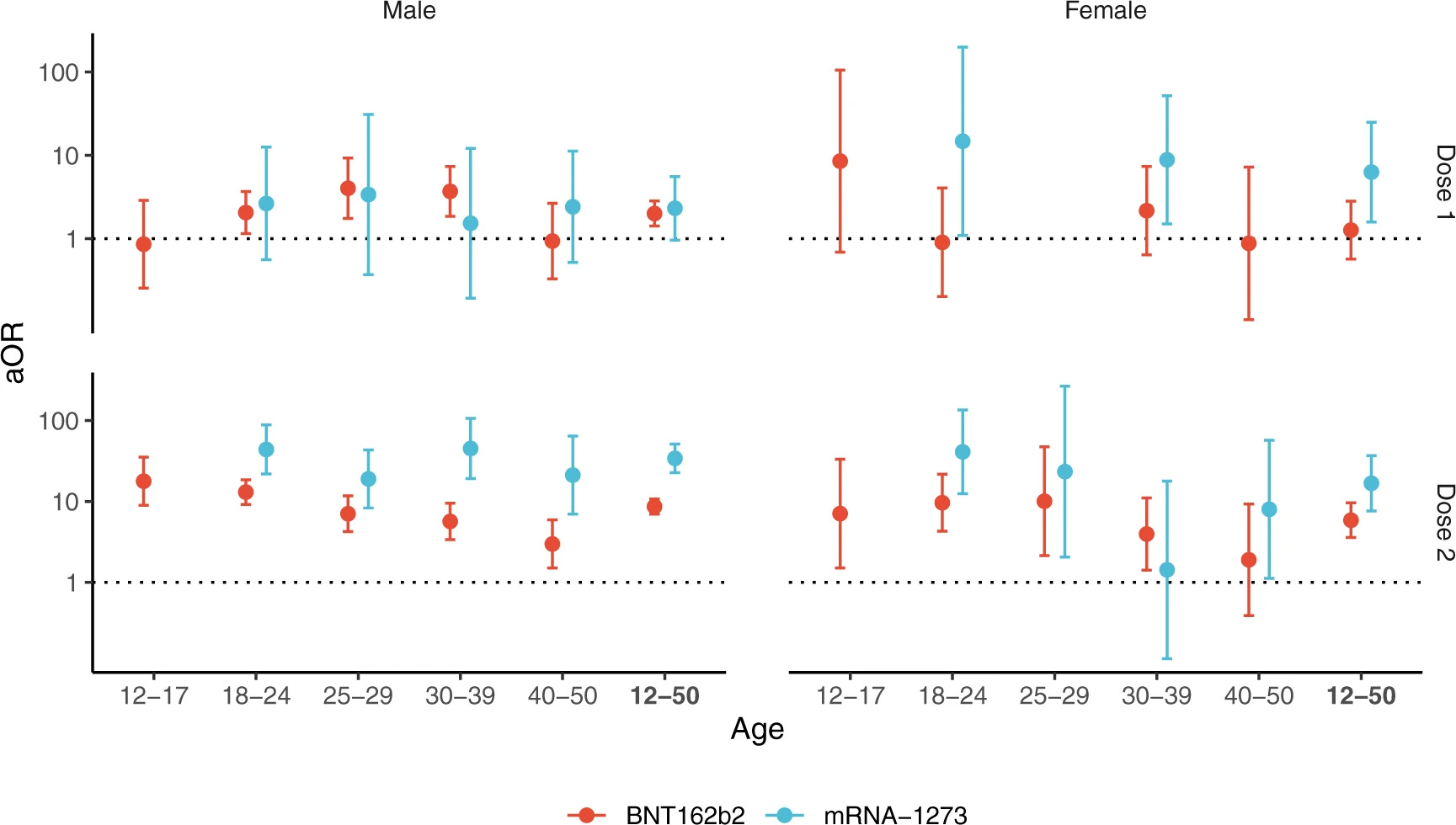
In this nationwide study involving a population of 32 million people aged 12 to 50 years having received 46 million doses of mRNA vaccines, we provide detailed estimates of the risk of myocarditis and pericarditis by sex, age categories and vaccine type. We find that vaccination with both mRNA vaccines was associated with an increased risk of myocarditis and pericarditis within the first week after vaccination. The associations were particularly pronounced after the second dose, and were evident in both males and females. We found a trend of increased risks towards younger age groups but a significant risk was also found in males over 30 years to develop myocarditis and in females over 30 years to develop a pericarditis after vaccination. Reassuringly, these cases of myocarditis and pericarditis, although requiring hospitalization, did not result in more severe outcomes than those unrelated to vaccination.
In conclusion, this study provides strong evidence of an increased risk of myocarditis and of pericarditis in the week following vaccination against Covid-19 with mRNA vaccines in both males and females, in particular after the second dose of the mRNA-1273 vaccine.
Using a massive sample size and a good methodology, the findings while not a surprise to anyone paying attention, should definitely open the eyes of the ones that don’t, and the vaccine pushers.
Self-evidency aside, the paper is clear, the younger you are, the higher your risk of developing heart inflammation, and damage from the vaccination alone. I would very much like to remind the layperson that, unless taken a very precise and (almost unique) approach, heart damage is forever. While evidence for healing heart damage is available, it is a very disputed territory among the most arrogant field of medicine, cardiology.
Now add everything we covered in this Substack so far, and everything other writers covered, there is no reason, anywhere, any person young than 40 should take the mRNA vaccines (and the Adeno ones for that matters) even IF they did stop infection, or severity, or whatever other lies they want to peddle.
If some people still want to take the vaccines after so many safety signals are publicly available for anyone to read, and many public sources interpreting and demonstrating to the layperson the damages of the magic potion, I am sad to say these people can’t be saved, even from themselves.
Another breadcrumb from 2020. And since they will, once again, experiment with a genetic, untested, therapy upon untold billions of people. A meme. My favorite meme.


I would like to get funding to conduct limited in vitro and ideally clinical trials for therapeutic antivirals as options are fast diminishing, but you need to set the frame of reference correctly or you will get nowhere.
This study shows some of the TLR range characteristics, I understand that possibly 2, 7 & 8 are being inhibited ie further variant infections & influenza especially:
Properties of toll-like receptors
TLRs Localization Ligands
TLR1/2 [33–35] Cell surface Triacylated lipopeptides
TLR2/6 [36–41] Cell surface Diacylated lipopeptides (Mycoplasma), Lipoteichoic acid (Streptococcus), Zymosan (Saccharomyces cerevisiae)
TLR2 [38, 42–48] Cell surface Peptidoglycan (Gram-positive bacteria), Lipoarabinomannan (Mycobacteria), Hemagglutinin (measles virus), phosphatidylinositol mannoside 6 (Mycobacteria), Glycosylphosphatidylinositol (Trypanosoma)
TLR3 [49–52] Endosome ssRNA virus (West Nile virus), dsRNA virus (Respiratory syncytial virus, murine cytomegalovirus)
TLR4 [43, 53–59] Cell surface Lipopolysaccharide (Gram-negative bacteria), Mannan-binding lectin (Candida albicans), glycoinositol- phospholipids (Trypanosoma cruzi), Envelope proteins (respiratory syncytial virus, mouse mammary tumor)
TLR5 [60, 61] Cell surface Flagellin (flagellated bacteria)
TLR7 [62, 63] Endosome ssRNA viruses (vesicular stomatitis virus, influenza virus)
TLR8 [64–66] Endosome ssRNA from RNA viruses
TLR9 [67–71] Endosome dsRNA viruses (herpes simplex virus, murine cytomegalovirus), CpG motifs from bacteria and viruses, Hemozoin (Plasmodium)
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7726878/
Great read. I still need to read the past posts 3 times. Not looking good is my position. And purely from an economic standpoint how on earth do the vaccine companies try & sell these new vaccines when the last ones went from doses 2 to 4 & still didn’t work like sold? In any other situation you’d want a refund, not another billion dollar bill, for the newest shitty product that comes with no guarantees or definite amount. If we yet again get mandated into these vaccines surely their will be an uproar?