


SARS-CoV2 - First signs of recombination
And the mitochondrial saga continues

This will be a post about aspects of this virus I am deeply interested, in the first one, and I hinted about it quite a few times. Recombination.
Finally, some real-world evidence of something a lot of “experts” didn’t think was possible. Except for Ralph Baric…
Evidence for SARS-CoV-2 Delta and Omicron co-infections and recombination
Between November 2021 and February 2022, SARS-CoV-2 Delta and Omicron variants co-circulated in the United States, allowing for co-infections and possible recombination events. We sequenced 29,719 positive samples during this period and analyzed the presence and fraction of reads supporting mutations specific to either the Delta or Omicron variant. Our sequencing protocol uses hybridization capture and is thus less subject to artifacts observed in amplicon-based approaches that may lead to spurious signals for recombinants. We identified 20 co-infections, one of which displayed evidence of a low recombinant viral population. We also identified two independent cases of infection by a Delta-Omicron recombinant virus, where 100% of the viral RNA came from one clonal recombinant. In both cases, the 5’-end of the viral genome was from the Delta genome, and the 3’-end from Omicron, though the breakpoints were different. Delta-Omicron recombinant viruses were rare, and there is currently no evidence that the two Delta-Omicron recombinant viruses identified are more transmissible between hosts compared to the circulating Omicron lineages.
Our study demonstrates the existence of co-infections, the presence of a recombinant population in at least one of these co-infections, and the existence of two infections consisting almost entirely of multiple copies of a recombinant virus. However, the mechanism by which a recombinant virus comes to dominate an infection remains somewhat of a puzzle. One possibility is that the two infections that contain only recombinant virus were themselves seeded by a recombinant virus. This implies that in their respective ancestral co-infections, the two recombinant viruses each rose to a high enough fraction to be transmitted during an exposure and were able to establish an infection in a new host. Yet, despite transmitting to a new host at least once, the transmission chain was not sustained; we have not observed any more of these recombinants in our sequencing data. The other possibility is that these two infections began as co-infections and that the recombinant viral population then completely outcompeted the Delta and Omicron populations within the host. Yet, it seems unlikely that Delta and Omicron can be completely cleared from a host, while leaving the recombinant virus population intact. Either way, in both scenarios, the recombinant did not appear to have an increased ability to transmit between hosts compared to co-circulating Omicron variants. There are parallels here with HIV-1, where chronic infection and host immune response leads to extensive within-host diversity of the virus, but the genotypes of the virus that ultimately seed new infections are from a much narrower set of viral types
This paper is rather complex unless you have a good understanding of molecular biology, and genetics, so I will skip the boring part. Unlike some previous statements of recombination, which were merely artifacts, the authors went to quite a great length to prove that recombination within infected individuals does happen.
So far the rate of recombination is fairly low, but still, it did happen and can lead to new variants. One of the arguments is that the recombinant viruses might arise from a coinfection (getting infected with both Delta and Omicron in this particular case), and give rise to a recombinant variant. Recombinants don’t transmit as normal lineage, but, just read the bold part.
We are back again at my argument. Insane back then, most likely by the day now, of chronic infections, which also leads to an argument by a brilliant scientist I know. Immuno-compromised hosts are genetic dead ends for transmission, but not for recombination, the virus will adapt to stay alive either way. The problem is the immune roller coaster in said patients, at some point they might transmit the recombinant variant.
Is this a concern right now ? Clearly not, but it will be within 12 months, not systemic, not globally I expect, but it will. And maybe next year, maybe in 5 years, I will be proved right. Covid, under specific conditions, is like EBV and other chronic pathogens.

Tracking SARS-CoV-2 Omicron diverse spike gene mutations identifies multiple inter-variant recombination events
The current pandemic of COVID-19 is fueled by more infectious emergent Omicron variants. Ongoing concerns of emergent variants include possible recombinants, as genome recombination is an important evolutionary mechanism for the emergence and re-emergence of human viral pathogens. Although recombination events among SARS-CoV-1 and MERS-CoV were well-documented, it has been difficult to detect the recombination signatures in SARS-CoV-2 variants due to their high degree of sequence similarity. In this study, we identified diverse recombination events between two Omicron major subvariants (BA.1 and BA.2) and other variants of concern (VOCs) and variants of interest (VOIs), suggesting that co-infection and subsequent genome recombination play important roles in the ongoing evolution of SARS-CoV-2. Through scanning high-quality completed Omicron spike gene sequences, eighteen core mutations of BA.1 variants (frequency >99%) were identified (eight in NTD, five near the S1/S2 cleavage site, and five in S2). BA.2 variants share three additional amino acid deletions with the Alpha variants. BA.1 subvariants share nine common amino acid mutations (three more than BA.2) in the spike protein with most VOCs, suggesting a possible recombination origin of Omicron from these VOCs. There are three more Alpha-related mutations (del69-70, del144) in BA.1 than BA.2, and therefore BA.1 may be phylogenetically closer to the Alpha variant. Revertant mutations are found in some dominant mutations (frequency >95%) in the BA.1 subvariant. Most notably, multiple additional amino acid mutations in the Delta spike protein were also identified in the recently emerged Omicron isolates, which implied possible recombination events occurred between the Omicron and Delta variants during the on-going pandemic. Monitoring the evolving SARS-CoV-2 genomes especially for recombination is critically important for recognition of abrupt changes to viral attributes including its epitopes which may call for vaccine modifications.
I don’t agree with many of the assumptions and propositions of this paper, but it has some good insights, especially above. As the pandemic slowly grows, and new Omicron-derived lineages come to dominate, we will see new, actual, recombinant viruses.
Given the poor level of neutralization and the insistence of governments to use useless treatments, one could deduce a pathogenic variant is a matter of time, not a matter of if, and it will most likely affect the vaccinated because all variants are immune evasive, antibody resistant, and I firmly believe are causing some level of atypical ADE. Lacking the N protein protection is a problem, injecting a vaccine-derived N problem is bigger. Nowhere to go, nowhere to hide.
I shared this paper, merely to put recombination on your radar, for you to be aware, and I already superficially covered it before, this will be an emerging trend this year. I personally suspect maybe Hong Kong is experiencing the growth of an under traced recombinant variant.
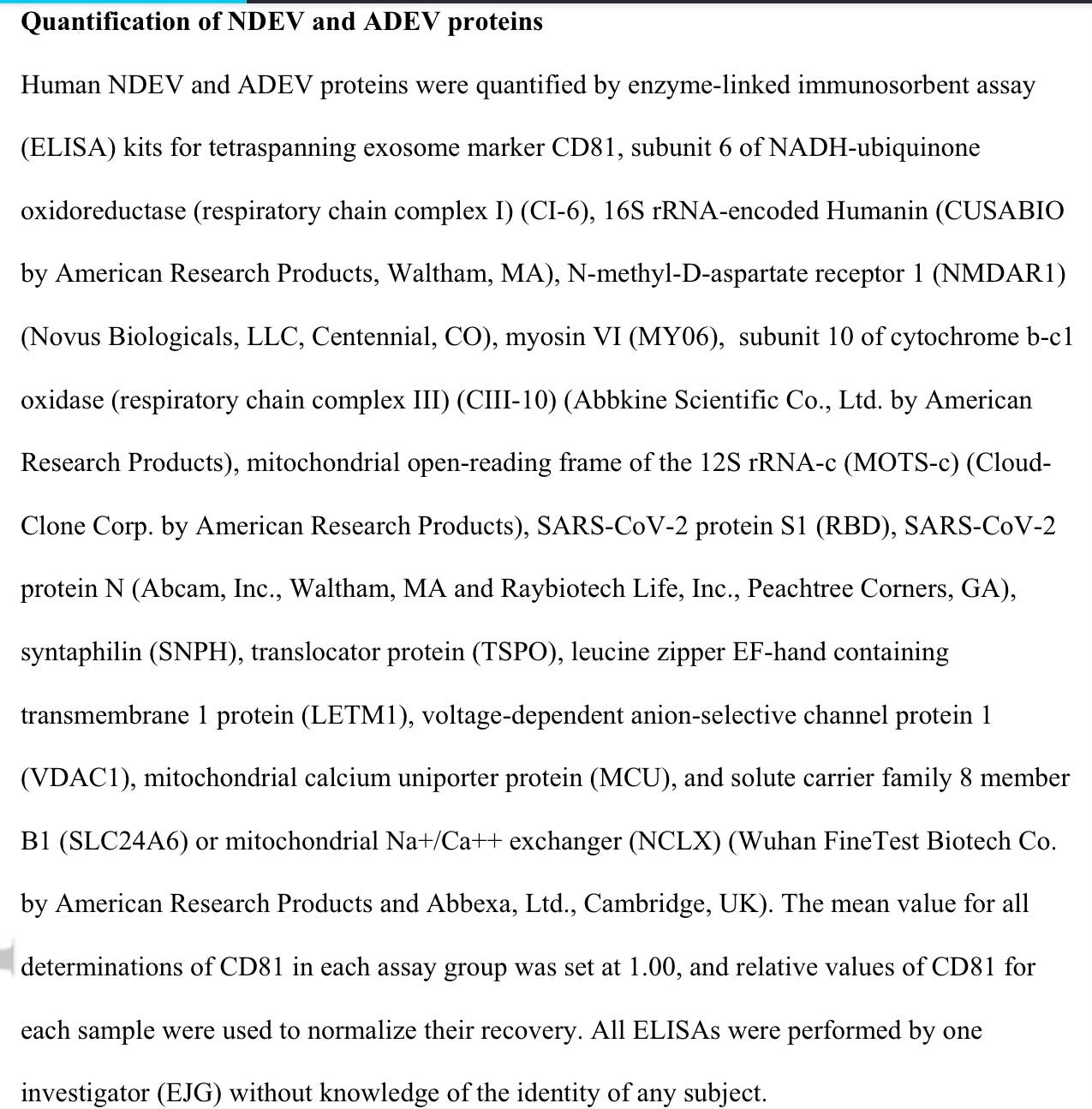
SARS-CoV-2 and mitochondrial proteins in neural-derived exosomes of COVID-19
For example, SARS-CoV-2 ORF9c and Nsp7 interact, respectively, with mitochondrial NDUFAF1 and NDUFAF2, which both are involved in the assembly of complex I of the mitochondrial electron transport chain. It thus tentatively appears that both SARS-CoV-2 RNA- and protein-dependent This article is protected by copyright. All rights reserved.
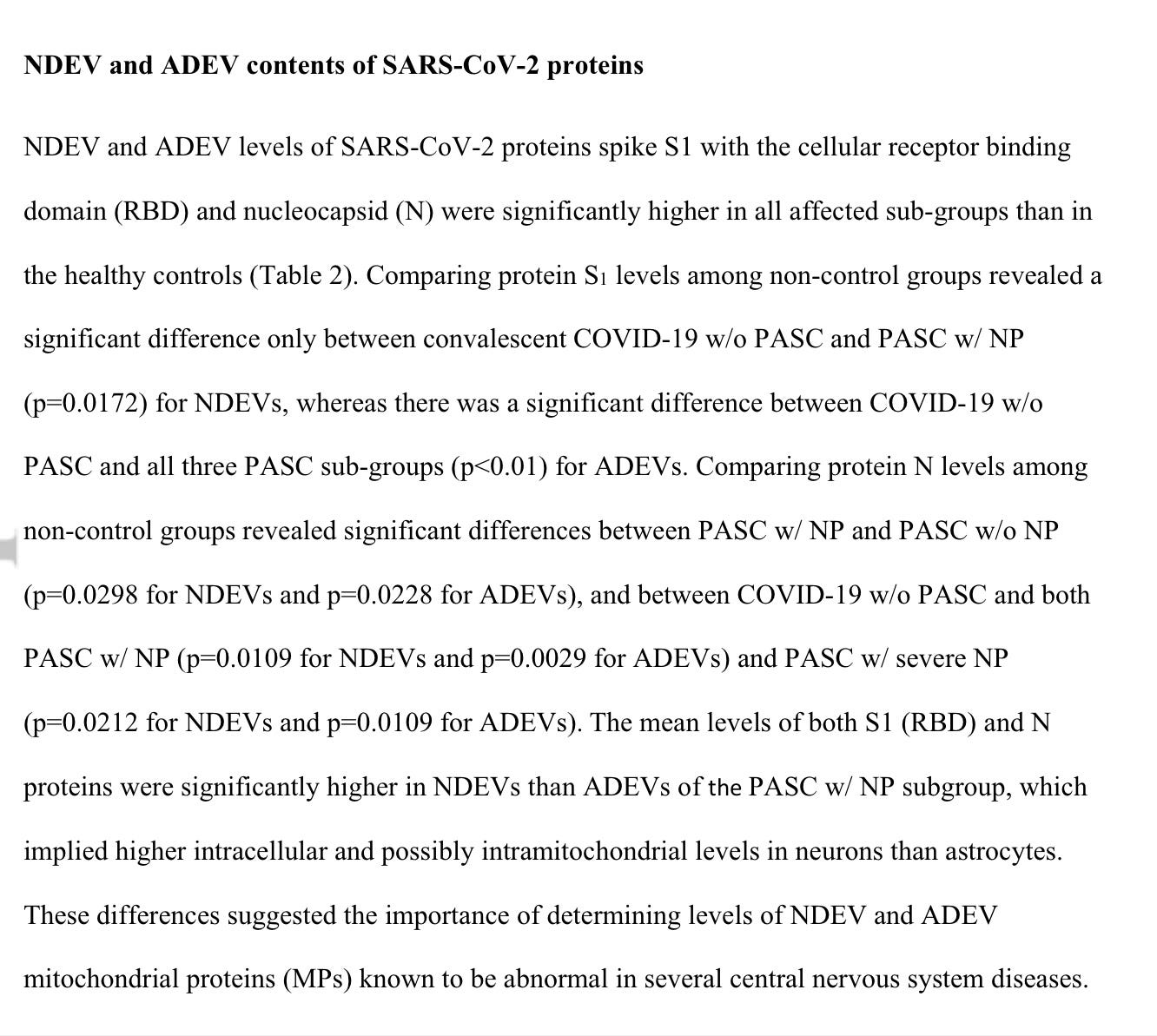
NDEV and ADEV levels of SARS-CoV-2 proteins spike S1 with the cellular receptor binding domain (RBD) and nucleocapsid (N) were significantly higher in all affected sub-groups than in the healthy controls
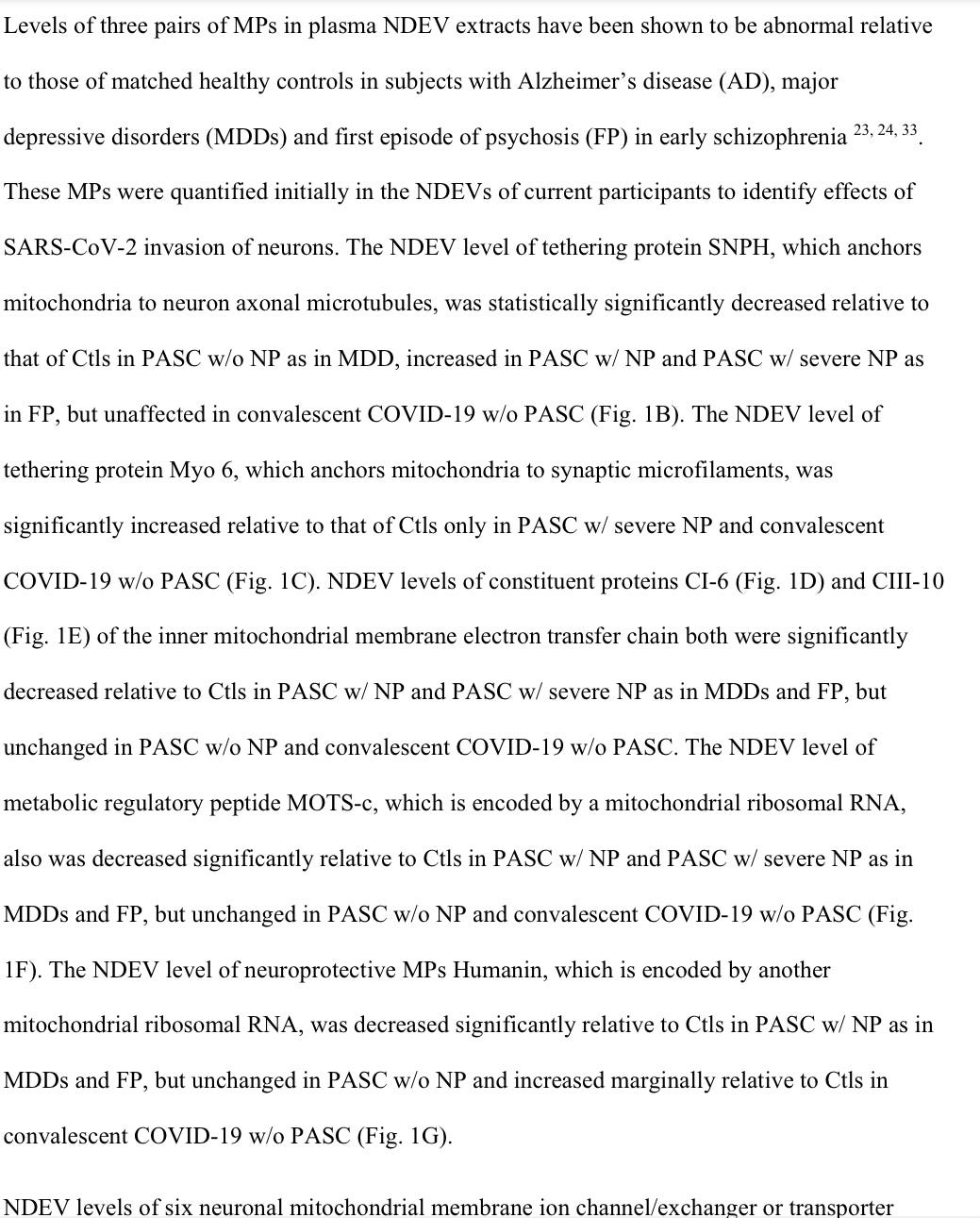

Again, another difficult paper has to do with finding new, viable markers, for Long Covid (referred to in most recent papers as PASC) patients, especially the ones with neuropsychiatric symptoms (NP).
It uses (my dreaded) Extracellular vesicles from specific neural cells as measurement markers, and they do find, abnormal levels between patients with or without NP, compared to the control. The paper is valid and interesting, but this isn’t the main reason I am sharing it.
The main reason is the same as I shared this one, and this, and in my first Biological Briefing. The fact that a good portion of the initial, and long-term damage is mitochondrial dysfunction, which can and will cascade into other types of inflammatory and neurological diseases.
Metabolic, energy/mitochondrial pathways are one of the most important aspects of this disease, and there is extensive evidence that the infection (before Omicron) affected and changed them entirely. A good overall place to start, this is a fairly complex topic before you delve in.
Addressing these changes, dysfunction, excessive inflammation, and its cellular byproducts is the easiest way to start to fix people with any form of sequelae from this disease.
Relationship between changes in symptoms and antibody titers after a single vaccination in patients with Long COVID
Coronavirus disease 2019 (COVID-19) is spreading worldwide; there is a need to address its sequelae known as Long COVID. This study evaluated postvaccination changes in symptoms and antibody titers in patients with Long COVID. Patients visiting the outpatient department specializing in Long COVID at our hospital were enrolled. Changes in symptoms were evaluated before and 14–21 days after first vaccination. Antibody titers were measured using ARCHITECT SARS-CoV-2 IgG II Quant at the same time. This study included 42 patients (median age: 45 years; 17 [40.5%] men). Median pre- and postvaccination antibody titers were 456 and 28,963 AU/ml, respectively. Postvaccination symptoms (fatigue, joint pain, and taste and olfactory abnormalities) were relieved, worsened, and unchanged in 7 (16.7%), 9 (21.4%), and 26 (61.9%) patients, respectively. Ratios of pre- and postvaccination antibody titers were 53, 40, and 174 in the unchanged, relief, and worsened groups, respectively. The worsened group had the significantly highest antibody titer ratio (p = 0.02). The higher increased rate of the antibody titer in the worsened group than in the nonworsened group suggests an excessive immune response to vaccination associated with worsening of sequelae. Although patients with Long COVID should be vaccinated, additional concerns should be addressed.
And for last, something I have been hammering on for months, from actual clinical evidence. Vaccination will often worsen the symptoms of Long Covid, and sometimes for a weird reason, will bring relief. In my opinion, the relief comes from, by mere accident, correcting the dominant immune response, and given how most of the vaccines work, kick-starting the immune system in dealing with whatever subclinical secondary infection Covid set off.
The higher the antibodies, the worse the symptoms in almost a third of this small study, bear the question I raised, that the non-neutralizing antibodies are driving atypical ADE, and worsening specific markers of inflammation, and I would bet shifting the immune response, among many other variables (micro clots, sCD40L, etc).
If you enjoy or take value from my independent, interdisciplinary analysis, consider becoming a free or paying subscriber, my work is fully supported by you. Sharing also helps me tremendously. I truly appreciate all supporters.
Very interesting, even for a layman.
The higher the antibodies, the worse the symptoms in almost a third of this small study, bear the question I raised, that the non-neutralizing antibodies are driving atypical ADE.
Right: COV-2 AB's-work-Reverse is becoming most CIA-Mossad-did-911, CIA-killed-JFK, like stuff? Stupid conspiracy negationists.
https://albertosilva.substack.com/p/reverse-immunogenic-evolutionary?s=w