
SARS-CoV-2, thymic atrophy and impaired T cell development
And the case of a persistent infection !

First, let us find out what is the thymus, for the readers who don’t know this small, yet very important part of you.
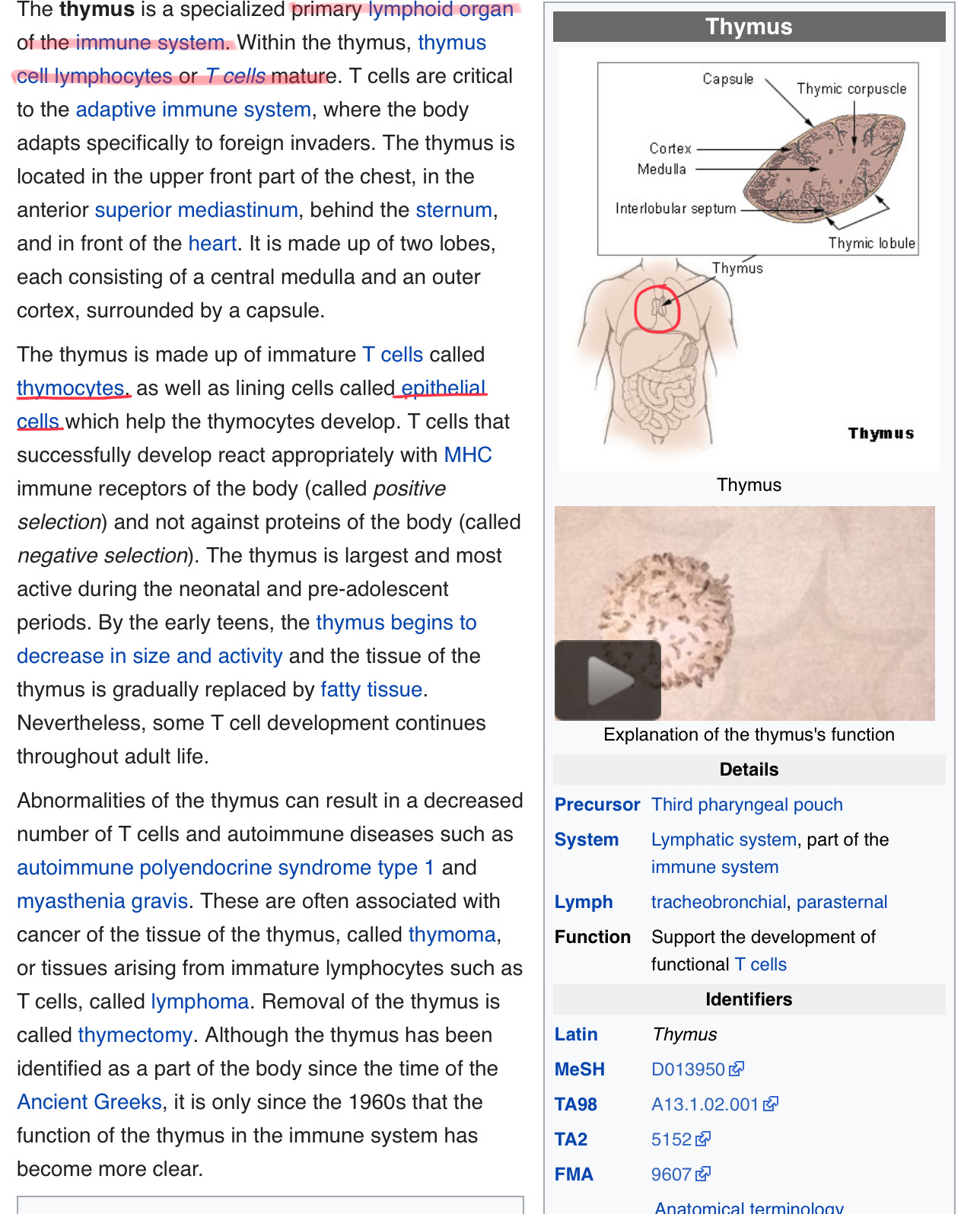
Clearly, a very important part of your immune system.
SARS-CoV-2 and its variants, but not Omicron, induces thymic atrophy and impaired T cell development
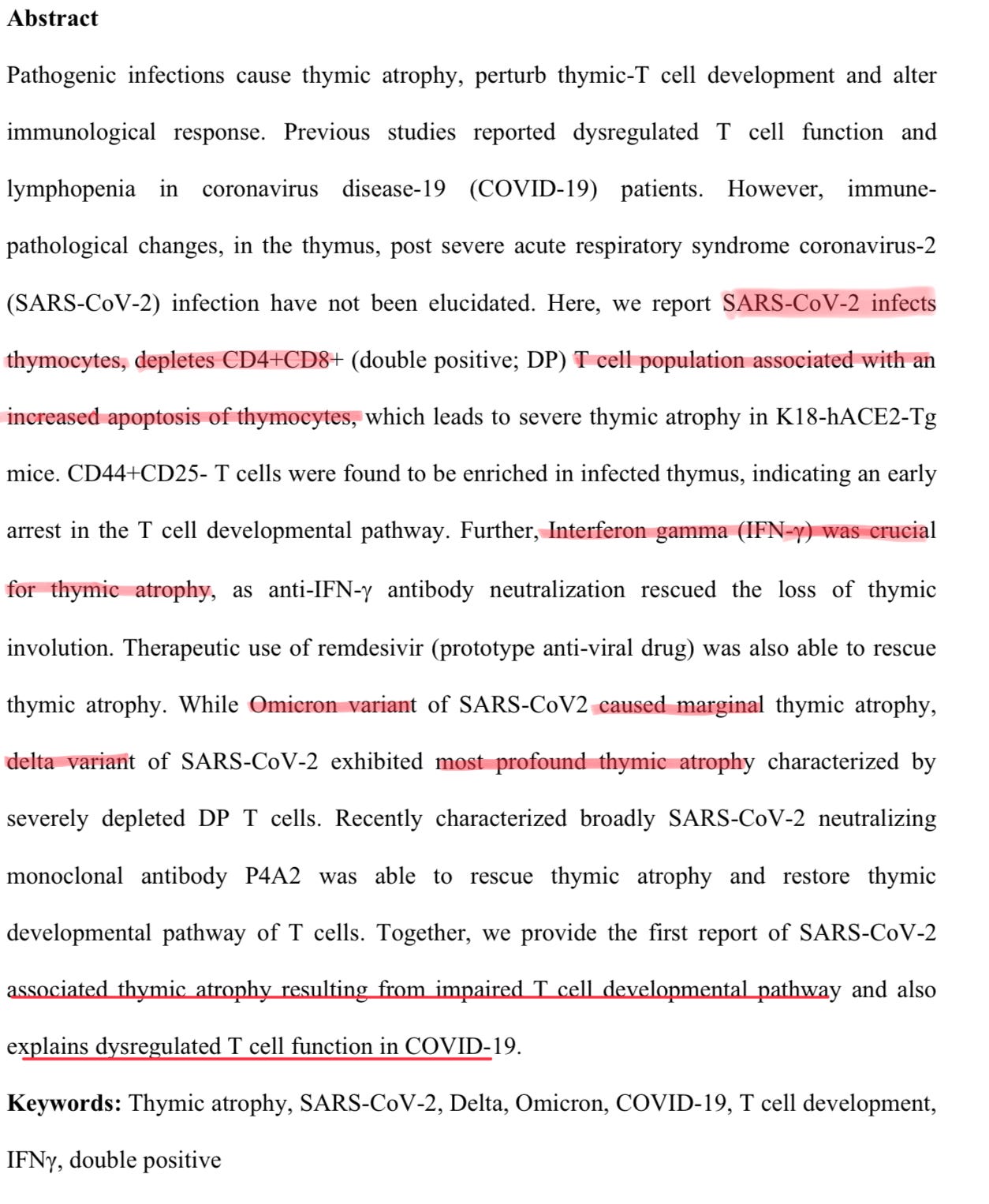
The abstract is relatively clear, also it is a research done in rats, but I expect this to translate pretty well to humans, everything fits well with all the available evidence. Authors found that SARS-CoV-2 infect thymocytes, followed by a increase of Interferon Gamma, which was the fuel to cause thymic atrophy.
The Omicron variant, while “mild”, caused a marginal thymic atrophy, and the Delta cause the most profound, severely depleting the immune cells. This explain the dysregulated T cell function in COVID-19 patients.
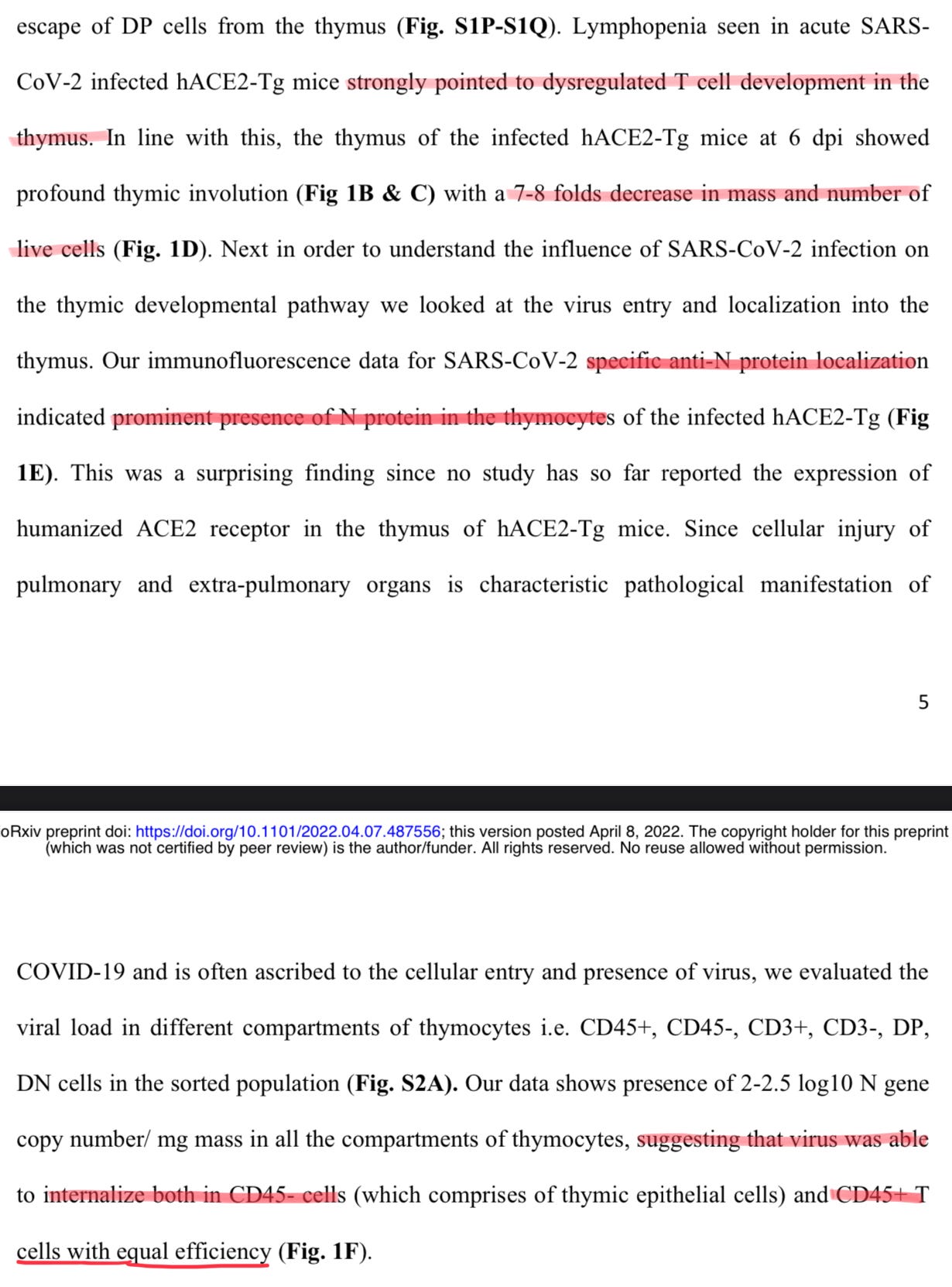
Lymphopenia is strongly correlated to dysregulated T Cells in the thymus, with the decrease of 8 times the living cells. To find if the virus got inside the cells, they tested for the N protein, and they found a decent amount of Nucleocapsid protein in the thymocytes, and the virus got inside body CD45 negative and positive cells. CD45 is one receptor in many of these cells, specially hematopoietic cells, which I covered a paper that I consider really important.

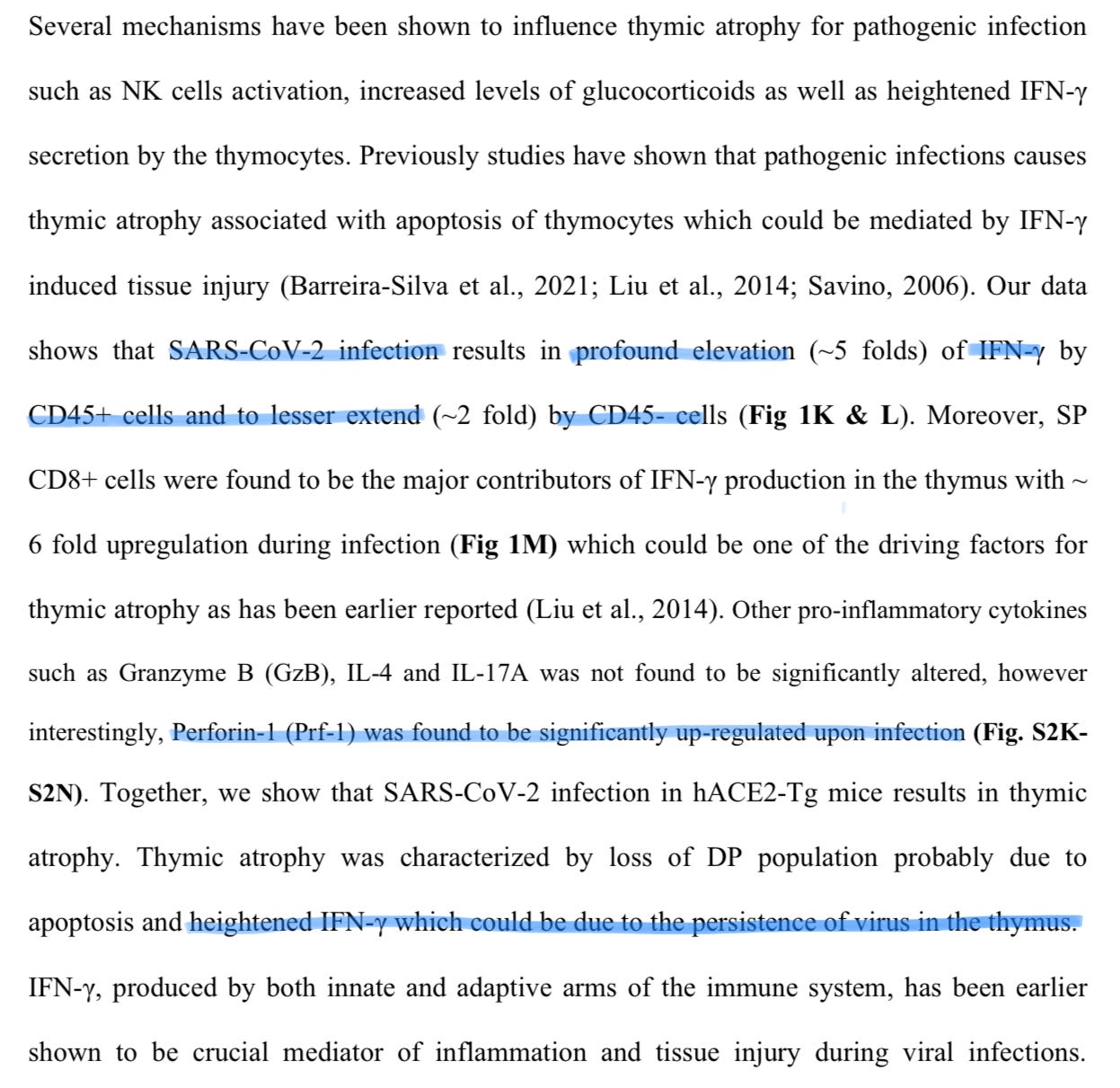
Upon infection, the paper shows a profound elevation of 5 fold of Interferon gamma by CD45 positive cells, and CD8 single positive cells (meaning they are only CD8 cells) were found to be the major contributors of Interferon Gamma in the thymus. Other cytokines were not found to be significantly more expressed (my favorite being IL-17A), but Perforin-1 was.
Perforin is a protein used by CD8 cells to, well…perforate, meaning poking holes in the cell membranes of invaders, or infected cells. They propose that the thymic atrophy and loss of cells was due to apoptosis, and that that increase 5 fold presence of Interferon gamma could be cause by persistence of the virus in the thymus. The post below has information on Interferon Gamma, and the axis with Interleukin 12.
Presence of virus or viral factors have been shown to activate TLR3, TLR7 and TLR8 and RLR which leads to induction of anti-viral genes and cytokines characterized by heightened IFN-γ response (Bonifacius et al., 2021; Moore and June, 2020). This would mean that the use of anti-viral drugs which could reduce the viral burden and reduce viral antigens would also effectively reduce the inflammatory IFN-γ production and hence thymic atrophy.
Paper go into details, which I don’t find as pertinent to discuss here, they propose using anti-IFN gamma therapy to arrest thymic atrophy, and tissue damage, and the dysregulation of immune function, but there is a major problem. Too much of IFN gamma is a problem, but too little, specially at the wrong time too. It can (and will) lead to viral persistence in some tissues, dependent on the person. Nothing I ever describe is population wide, just enough to cause problems, perhaps bigger ones down the road.
At least treatments to rescue thymic function exist, specially in the case of SARS-CoV-2, as the authors discuss.
This paragraph is interesting and the paper itself too. How many people got breakthrough infections from Delta ? Hundreds of millions, at the very least, it was when breakthroughs kicked off in reality, when I started seeing the pattern. How much of the immune dysfunction we see is caused by this exact mechanism, and not just the vaccines (as I often argument). Even though they state Omicron causes marginal atrophy, how much breakthrough infection one can experience, until the marginal becomes enough to cause dysfunction, and set off a cascade ?
Testing the N protein was necessary for the authors to demonstrate their hypothesis, and I appreciate this paper, but, I would love for them, or any other team to test other parts of the virus, and what they might set off in thymocytes, and in the thymus. Yes, the reader might know where I am going with this one. I, once again, believe this is cause by parts of the Spike Protein itself, and not solely any of the other proteins.
I never did edit one of my posts, but here is the first time. It is know that SARS-CoV-2 has the SEB on its sequence, and also the antigenic sites of different pathogens. So here, another reason for the thymic atrophy, and why Omicron inflicts less of it, because the SEB sequence got attenuated.
As a final side note to this paper. Source.
If you want a rabbit hole to dig, CXCR4-GP120 bystander effect.
And persistent infection lead us to the next, very interesting paper.
Evolution of a globally unique SARS-CoV-2 Spike E484T monoclonal antibody escape mutation in a persistently infected, immunocompromised individual
The entire paper is quite interesting, but this is just to exemplify the fact that persistent (chronic) infections exist, and they will grow in number, if researcher know how to test, and where to look. Reading what you read so far, knowing what you know to this point.
How many of the vaccinated, with poor immune function for various reasons, are breeding ground for highly evasive, glycan creating (more on this in another post), immune resistant variants, that will create the perfect state for persistent infections ? How we will define what is a breakthrough infection, and what is a persistent one, given the testing design being obviously flawed ?
Got a feeling this post will be fairly pertinent in the future, changing BA. 2 to something else.
And I stick to my previous statement. The type of receptor SARS-CoV- uses dictates the fate of the cell (which type of cell death it suffers).
Buy me a coffee whenever you feel like it.
Deep appreciation for all the supporters !
Take out your thymus and, amongst other things, that's your immune tolerance broken, aka a trigger for multiple autoimmune disorders like lupus after a build up of usually 3+ years.
The role of thymic tolerance in CNS autoimmune disease
Adam E Handel et al. Nat Rev Neurol. 2018 Dec.
https://pubmed.ncbi.nlm.nih.gov/30451970/
Another great piece in the puzzle thanks.
I've been looking into GP 120 & IL6 in some detail. You don't need GP 120 for the induced pathology but it helps.
I really hope spike protein is not as oncogenic as HIV. We will find out in the next 1-3 years.
This Substack explores the oncogenic potential of GP120, of how it upregulates cytokines including oncogenic interleukin 6, how both upregulate a multidrug resistant protein, the pathology of MRP1 and finally some potential therapeutics are explored.
Spike protein (inc vax) induced immunodeficiency & carcinogenesis megathread #27: Further investigations into GP120, IL-6 & multidrug resistance
https://doorlesscarp953.substack.com/p/spike-protein-inc-vax-induced-immunodeficiency-298?s=w