
SARS-CoV-2 Reinfection, hospitalization and death
And Omicron BA. 5

This will be a two-for-one. The number of papers getting out talking about vaccination, waning efficacy, and natural immunity is large, and I have covered these so much I thought most of my subscribers are bored by now, they also often go viral on social media. These two were enough to push me to write this piece.
Risk of infection, hospitalisation, and death up to 9 months after a second dose of COVID-19 vaccine: a retrospective, total population cohort study in Sweden
The study design is quite good (design matters), from the paper “each individual who was vaccinated with two doses, with no documented SARS-CoV-2 infection and alive within 14 days of vaccination, was matched (1:1) to one randomly sampled individual from the rest of the cohort on birth year and sex. Baseline for both individuals in each matched pair was set to the date of the second dose of vaccine in the vaccinated individual. Matched individuals were excluded if they received the first dose of vaccine, had a documented previous SARS-CoV-2 infection, or died within 14 days of baseline, whereby a new individual was searched from the remaining total cohort. This procedure was repeated five times.”
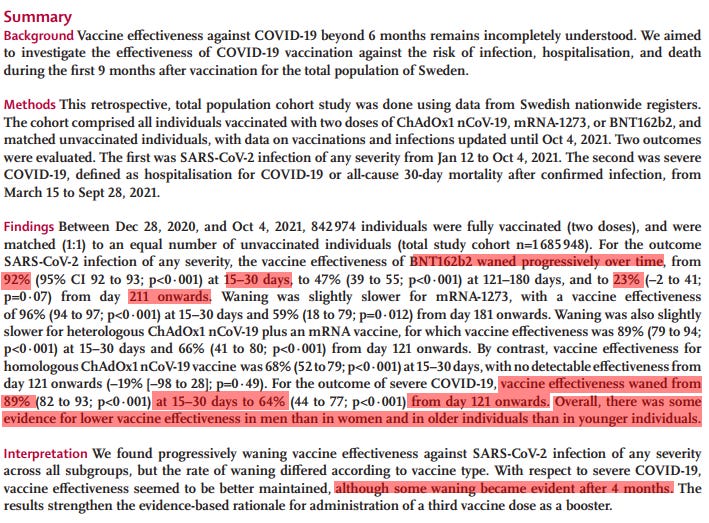
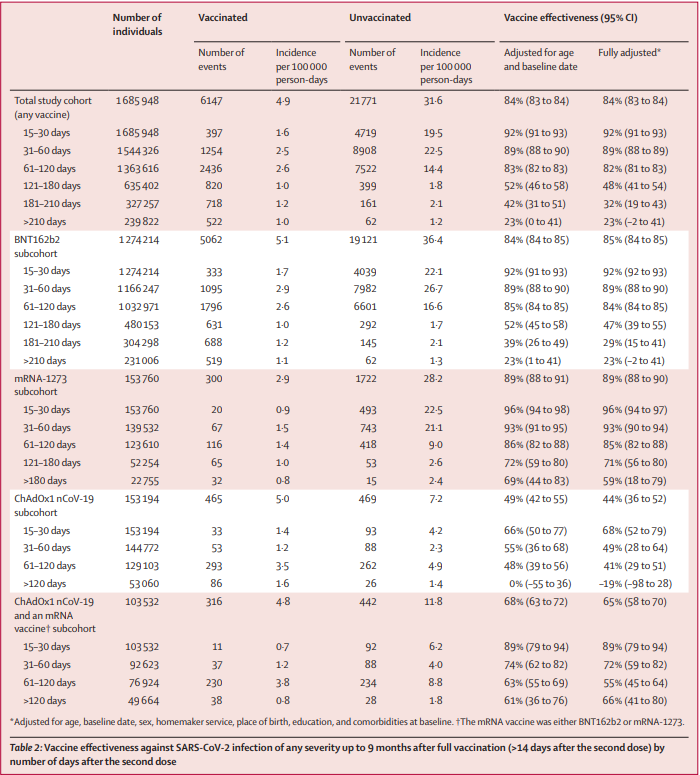
This research has a massive cohort (group of people participating in something), and as you can see from the first image, the obvious and already covered here, elsewhere, almost anywhere, the waning efficacy of the vaccines against infection. If you pay attention to the ChAd0x subcohort, using only that vaccine, when adjusted, after 120 days the efficacy goes negative.
As often I write myself, this isn’t exactly news, not only have I covered the possible mechanisms and all the signals since early 2021, but since the start of Omicron, there was no way to hide the waning. In fact here are some of the numerous aspects of this I covered.

Your overall metabolic health will also impact your immune response and breakthrough infection rate.
And let us not forget.
If you are a layperson and often get lost in the science stuff, I will make it simple. There are, quite literally, a dozen different dynamics on why the vaccines wane so fast, why the antibodies don’t last that long, and why the immunity they elicit varies so greatly among people in the same age group, and these are the most meaningful ones, a “blanket approach” if you will.
The reason I used the paper above, which has many many similar ones being published right now, is the following.
Increasing SARS-CoV2 cases, hospitalizations and deaths among the vaccinated elderly populations during the Omicron (B.1.1.529) variant surge in UK.
There were increased SARS-CoV2 hospitalizations and deaths noted during Omicron (B.1.1.529) variant surge in UK despite decreased cases, and the reasons are unclear.
Of the total cases (n= 22,072,550), hospitalizations (n=848,911) and deaths (n=175,070) due to COVID-19 in UK; 51.3% of cases (n=11,315,793), 28.8% of hospitalizations (n=244,708) and 16.4% of deaths (n=28,659) occurred during Omicron variant surge. When comparing the period of February 28-May 1, 2022 with the prior 12-weeks, we observed a significant increase in the case fatality rate (0.19% vs 0.41%; RR 2.11[ 2.06-2.16], p<0.001) and odds of hospitalization (1.58% vs 3.72%; RR 2.36[2.34-2.38]; p<0.001). During the same period a significant increase in cases (23.7% vs 40.3%; RR1.70 [1.70-1.71]; p<0.001) among ≥50 years of age and hospitalizations (39.3% vs 50.3%;RR1.28 [1.27-1.30]; p<0.001) and deaths (67.89% vs 80.07%;RR1.18 [1.16-1.20]; p<0.001) among ≥75 years of age was observed. The vaccine effectiveness (VE) for the third dose was in negative since December 20, 2021, with a significantly increased proportion of SARS-CoV2 cases hospitalizations and deaths among the vaccinated; and a decreased proportion of cases, hospitalizations, and deaths among the unvaccinated. The pre-existing conditions were present in 95.6% of all COVID-19 deaths, various ethnic, deprivation score and vaccination rate disparities noted that can adversely affect hospitalization and deaths among compared groups.
CONCLUSIONS
There is no discernable vaccine effectiveness among ≥18 years of age, vaccinated third dose population since the beginning of the Omicron variant surge. Pre-existing conditions, ethnicity, deprivation score, and vaccination rate disparities data need to be adjusted for evaluating VE for hospitalizations and deaths. The increased cases with significantly increased hospitalizations and deaths among the elderly population during the Omicron variant surge underscores the need to prevent infections in the elderly irrespective of vaccination status with uniform screening protocols and protective measures.
Recent papers and graph analysis (statistic analysis using graphs for easier understanding and data visualization) have been somewhat positive in the outcomes of recent infections, but a little over the place, they all point to a decline in death and severity. It takes too much time to deconstruct data manipulation going on on all sides, so I think to “science”.
In line with everything covered so far, there was a measurable increase in deaths in the first Omicron wave, after crunching the numbers, there was no vaccine effectiveness among the vaccinated, and as the authors themselves state, there are many reasons for this, one being Omicron just blast through the previous immunity acquired from either infection or the diminishing immunity from the vaccines. Also worth note 95% of the deaths were in people with some underlying issues.
We also noted increased cases among ≥50 years age groups associated with significantly increased hospitalizations and deaths particularly in ≥75 years age group (80.1% of total deaths) after February 27, 2022
Additionally, the vaccinated with third dose had significantly higher infection rates than vaccinated with two doses and unvaccinated during the Omicron variant surge (since February 2022). This was associated with a significantly higher proportion of hospitalizations in vaccinated with two doses than unvaccinated during the Omicron variant surge (since January 2022), higher proportion of deaths in vaccinated two doses than unvaccinated (since October 2021) and higher proportion of hospitalizations and deaths in vaccinated with third dose than vaccinated with two doses and unvaccinated during Omicron variant surge (since February 2022).
Most of the deaths were in old people, as this was the case since March 2020, and the reason for loss of vaccine effectiveness among these is also documented and I linked a few here. Diabetes will affect your immune response, Vitamin D levels (old people have poor Vitamin D level), among many many other measurable markers, old age itself will hinder your B cell and T cell response.
Now to the crux of this matter. Why would having more vaccine-elicited antibodies be detrimental to your ability to avoid infection, and why it would lead to more deaths, even if this is mostly among old people. Was it what I described in the paragraph above ? No, boosting would boost your antibody levels regardless, even if marginal by a poor immune response. In my opinion, it is exactly as the paper I covered recently hypothesized. Competition between your cells to create new B cells and antibody response.
For honesty's sake, I will like to voice my observation, given real-world data so far, that natural infection, or “hybrid immunity” (which I find a dishonest way to describe what is happening) is holding the line. Both of these lowered both severity and deaths. Before anyone asks, hybrid immunity is in my opinion scientific manipulation of the data and building-specific designs and tests to avoid describing what is happening. At some level, the vaccinated immune system is attempting to overwrite the antigenic imprinting that is going on. In fact, all early BAs had decreased severity regardless of vaccination status or a previous infection in California, even the country you analyze will affect the data.
And the reason I decided to cover both of these papers is the following.
Enhanced innate immune suppression by SARS-CoV-2 Omicron subvariants BA.4 and BA.5
We find Omicron BA.4 and BA.5 replication is associated with reduced activation of epithelial innate immune responses versus earlier BA.1 and BA.2 subvariants. We also find enhanced expression of innate immune antagonist proteins Orf6 and N, similar to Alpha, suggesting common pathways of human adaptation and linking VOC dominance to improved innate immune evasion. We conclude that Omicron BA.4 and BA.5 have combined evolution of antibody escape with enhanced antagonism of human innate immunity to improve transmission and possibly reduce immune protection from severe disease.
To be fairly clear, especially for the layperson, a lot of these studies are done in cell lines, while they are important and give us really good insights, cell lines lack proper metabolism, nutrients that we have, and an actual dynamic immune response, and many other things. Don’t interpret what you are about to read as the end of the world for anyone.
Strikingly, this revealed reduced induction of Interferon-β (IFNB) and ISGs including inflammatory chemokine CXCL10 and RSAD2, DDX58, IFIT1 and IFIT2 by BA.4 and BA.5, as compared to BA.1/BA.2
The diminished innate immune activation byBA.4 is likely explained by slower replication in Calu-3, but BA.5 replication was similar to BA.1 and BA.2 and yet induced significantly less innate response in infected cells. The greater levels of IFNβ induced by BA.1 and BA.2 restricted their replication, because inhibition of IFN-mediated JAK/STAT signaling with Ruxolitinib rescued BA.1 and BA.2 infection in Calu-3 to a greater degree than Delta or BA.5
Unlike BA. 1 and 2 which didn’t immune suppressed your Interferon responses much, BA. 4 and 5 do, they lower and delay the immune response of your body. To simplify it, the immune response you got after getting infected by the first subvariants from Omicron is what made it “like a vaccine”, in which BA. 4 and 5 are delayed and this might become a problem because this is one of the main mechanism for the massive inflammatory response we saw with both Alpha and Delta.
Delaying a molecular response will lead to overcompensation, your body will produce too much of that thing, and it will lead to exacerbated inflammation. A lot of variables come into play, this isn’t a problem itself for now, and dare I say this is one of the consequences of the hyperglycolitc mutation (L452). The problem is the following.
…detecting viral proteins at this time point suggested that BA.5 expressed higher levels of Orf6 and N. ). Indeed, quantitation of two immunoblots from independent experiments supported higher levels of Orf6 for BA.4 and BA.5 and higher N levels for BA.5…and enhanced expression of all viral proteins but 87 enhancement of BA.4 and BA.5 Orf6 and N expression was still apparent…
We hypothesise that increased Orf6 translation or enhanced protein stability, perhaps through increasing a viral Orf6 binding partner, explains enhanced Orf6 expression.
Together these data confirm Orf6 as a viral innate immune antagonist, and are consistent with a model in which, like Alpha, BA.5 enhancement of Orf6 expression contributes to the reduced innate immune response as compared to its parental BA.2 isolate
The problem lies not only in the immune suppression but in the higher expression of ORF6 and N protein. ORF (Open Reading Frame) are accessory genes, meaning they are not essential for viral replication, but they play roles in either that or in creating disease, the others are NSP (non-structural proteins).
ORF6 is one of the nasty ones because besides what is described here, is one of the parts of the virus that has actual amyloid-creating sequences (I will cover this…one day) unlike what certain people covered so far, this amyloid sequence is known to cause amyloid crystalization and it has a lower metabolic rate (meaning these are formed over a longer period of time, and are harder to degrade, among other functions). Viral replication left unchecked could lead to amyloid formation via different pathways, to what extent no one can tell.
And a higher expression of N is a double edge sword. You need N immunity to properly clear the viral infection and to elicit a broader response, yet under an antigenic imprinted scenario, not clearing the N protein is in my opinion one of the causes of Long Covid. The persistence of viral fragments.
It is safe to say with some degree of certainty that BA. 5 has the hallmarks of being somewhat problematic, it is behaving much like Alpha/Delta, but now we have different levels of immunity going on, so in regards to severity, we will see, fatality we might see a minor spike. My biggest concern is post-viral infection damage. Long Covid. Given what I covered so far in this Substack, it is easy to deduce the chances of Long Covid or what I call “after effects” (post-viral infection damage) will grow in a statistically significant way.
Innate immune suppression, higher expression and stability of the nastier proteins (In my opinion), and the hyperglycolitc mutation, alongside other clinical observations lead me to ask my reader to not let your “guard down”. Yes, most of us are immune, but this isn’t over, and for sake of simplification I didn’t cover everything I believe the newer variants might be able to do AFTER infection.
The infection is actually the least of my worries for most people. This is after all, still SARS. I will try to cover an aspect of Long Covid that ties with a lot of what believe is driving a lot of these outcomes. Yes, it is the Kynurenine Pathway if you want to dig into that labyrinth.
Oldie but goodie on why the original vaxxes weren't going to work. You only need to watch the 1st minute to get the point, but the whole things is well explained in laymens terms, without being overstated.
https://www.bitchute.com/video/7XXmStI8VINb/
BA.5 should be called ADE.