

SARS-CoV-2 - Recombination, Omicron immunity, ADE ?
SARS-CoV-2 - Recombination, Omicron immunity, ADE ?
High viral loads !

Other authors are already covering the number of cases, deaths, and everything in between in some countries experiencing massive surges of cases, and death. I will refrain from it for now.
As the technology, and computer models/tracking gets better, you will see more, and more papers talking about, and correctly tracking recombinant, and they might become a real problem, mainly for the vaccinated, but perhaps for both, who knows where evolution might shift. I have been following the recombination trend for a while, because I was expecting it. The post below is of really importance overall, but here are the posts directly talking about recombination. First signs of recombination, and Delta Omicron recombination.


A recombinant variant between BA. 1, and BA. 2, which could be expected. I know some readers might ask how, if they are the same “variant”. They are, but they are very distinct, I also covered this. Worth to note, the XE variant seems to be outcompeting its forefathers, and some expect it to completely take over in the coming weeks, no official news about how “bad” it can be.
Unofficially, seems it hits the gut for a few weeks (diarrhea mainly), cough, and Omicron symptoms. I find curious in the hitting the gut for longer…
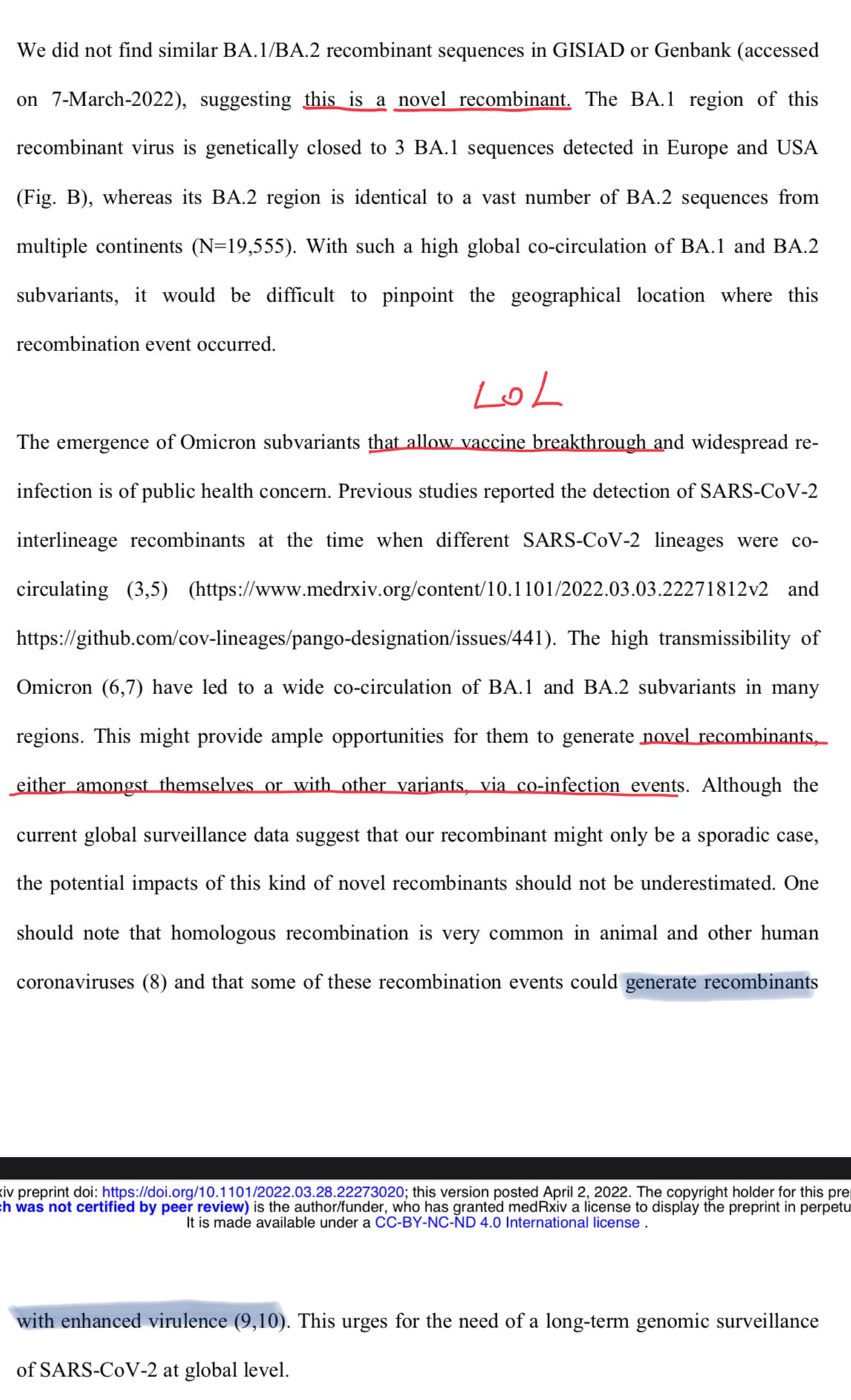
Detection of a BA.1/BA.2 recombinant in travelers arriving in Hong Kong, February 2022
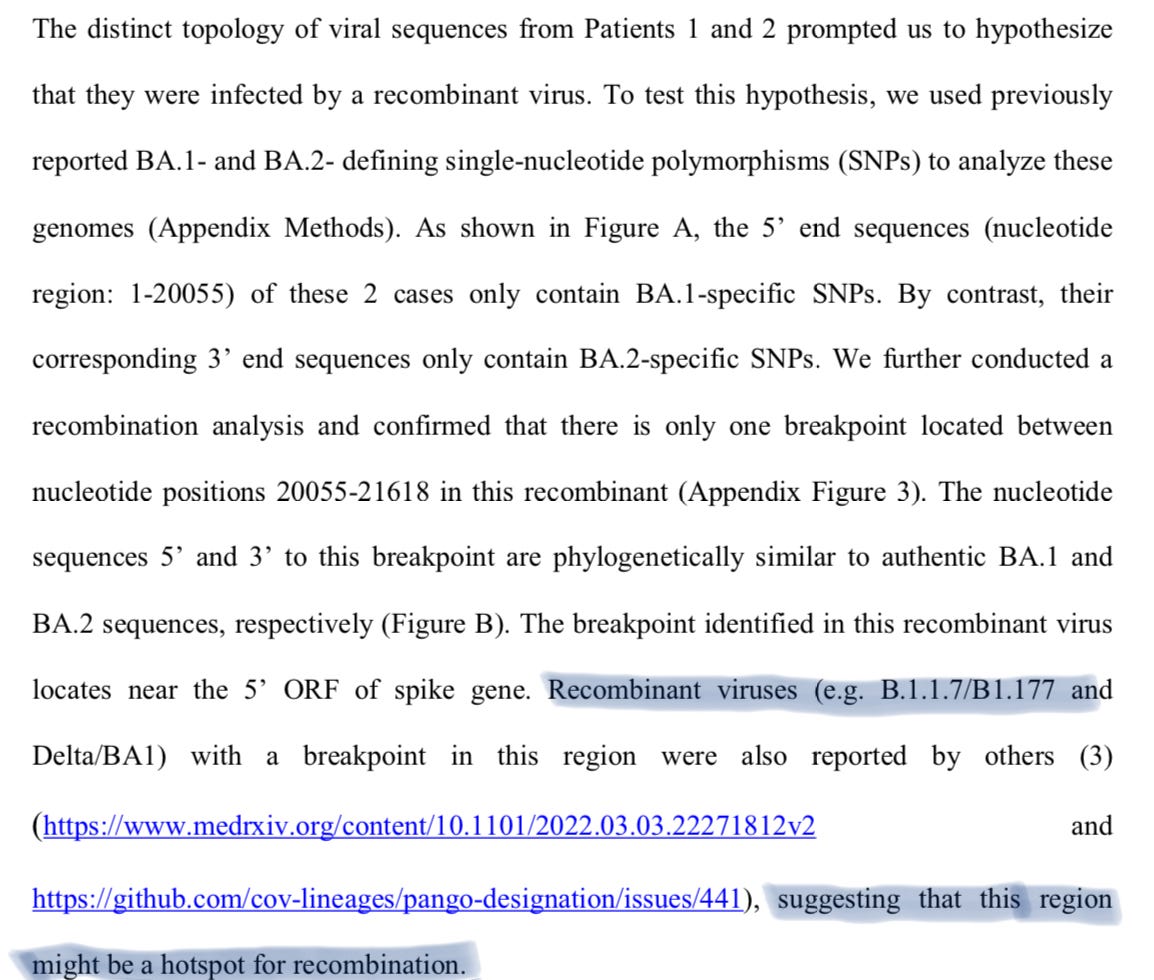
Per other posts I have been keeping an eye on Honk Kong, among some other places for being hit in a very odd way, with slightly higher number of deaths. Neither the doctors, or scientists, or even myself would jump to conclusions, but one thing is for certain. Either we are seeing a form of still to be categorized ADE, or a stealth variant. Meaning, a variant that can coinfect, and pass mostly undetected (a stretch I know lol, but hell, most of my insane ideas became true, so who knows).
The LOL is about the authors ignoring the mountain of evidence about the vaccines, and everything else… I am being harsh, because if they went that route, this paper would never be accepted, even as a pre-print. Now, to the fun part.
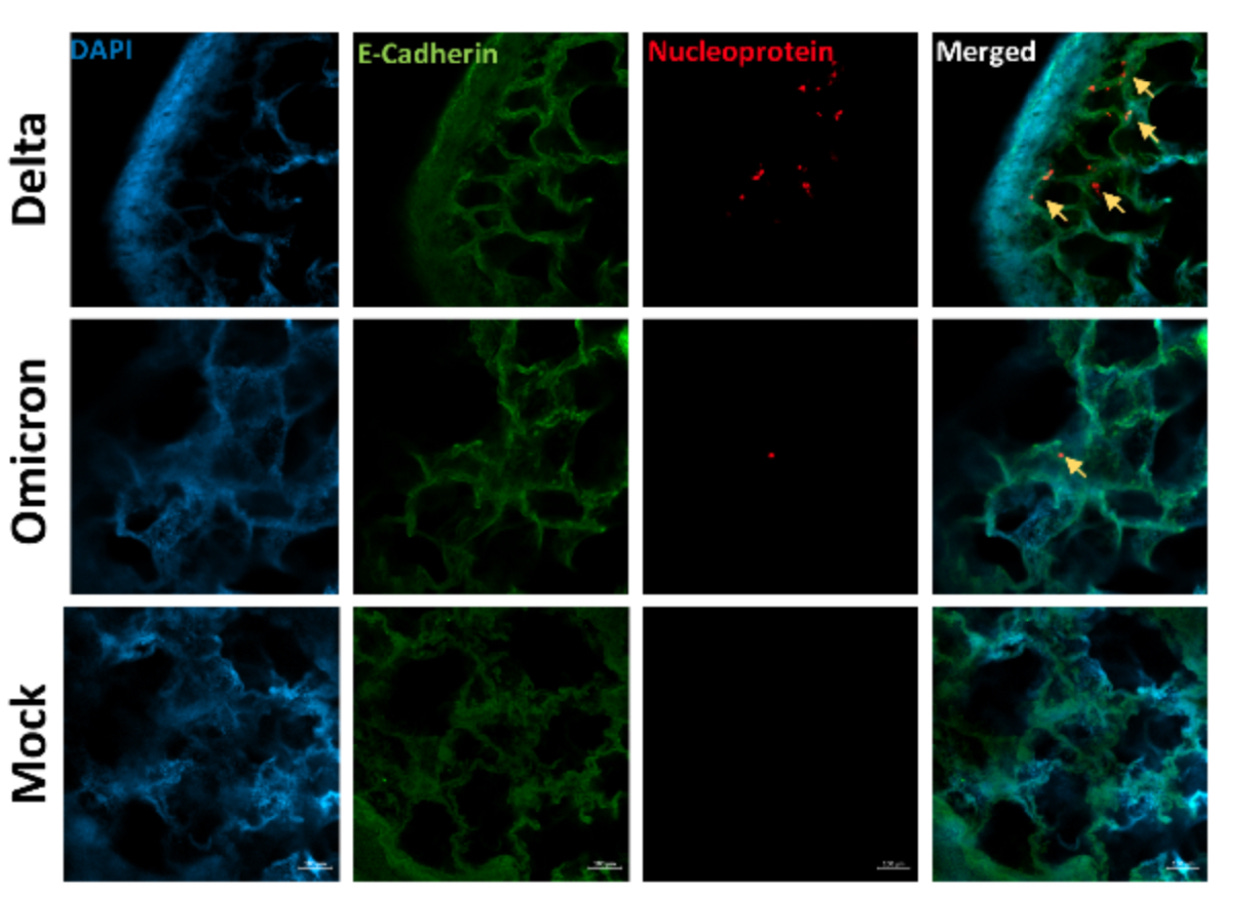
SARS-CoV-2 Omicron is specifically restricted in its replication in human lung tissue, compared to other variants of concern
SARS-CoV-2 Omicron variant has been characterized by decreased clinical severity, raising the question of whether early variant-specific interactions within the mucosal surfaces of the respiratory tract could mediate its attenuated pathogenicity. Here, we employed ex vivo infection of native human nasal and lung tissues to investigate the local-mucosal susceptibility and innate immune response to Omicron, compared to Delta and earlier SARS-CoV-2 variants of concern (VOC). We show that the replication of Omicron in lung tissues is highly restricted compared to other VOC, whereas it remains relatively unchanged in nasal tissues. Mechanistically, Omicron induced a much stronger antiviral interferon response in infected tissues compared to Delta and earlier VOC - a difference which was most striking in the lung tissues, where the innate immune response to all other SARS-CoV-2 VOC was blunted. Our data provide new insights to the reduced lung involvement and clinical severity of Omicron
We are finally having access (or they finally decide to publish it) to the specific immune responses Omicron elicits in most infected.
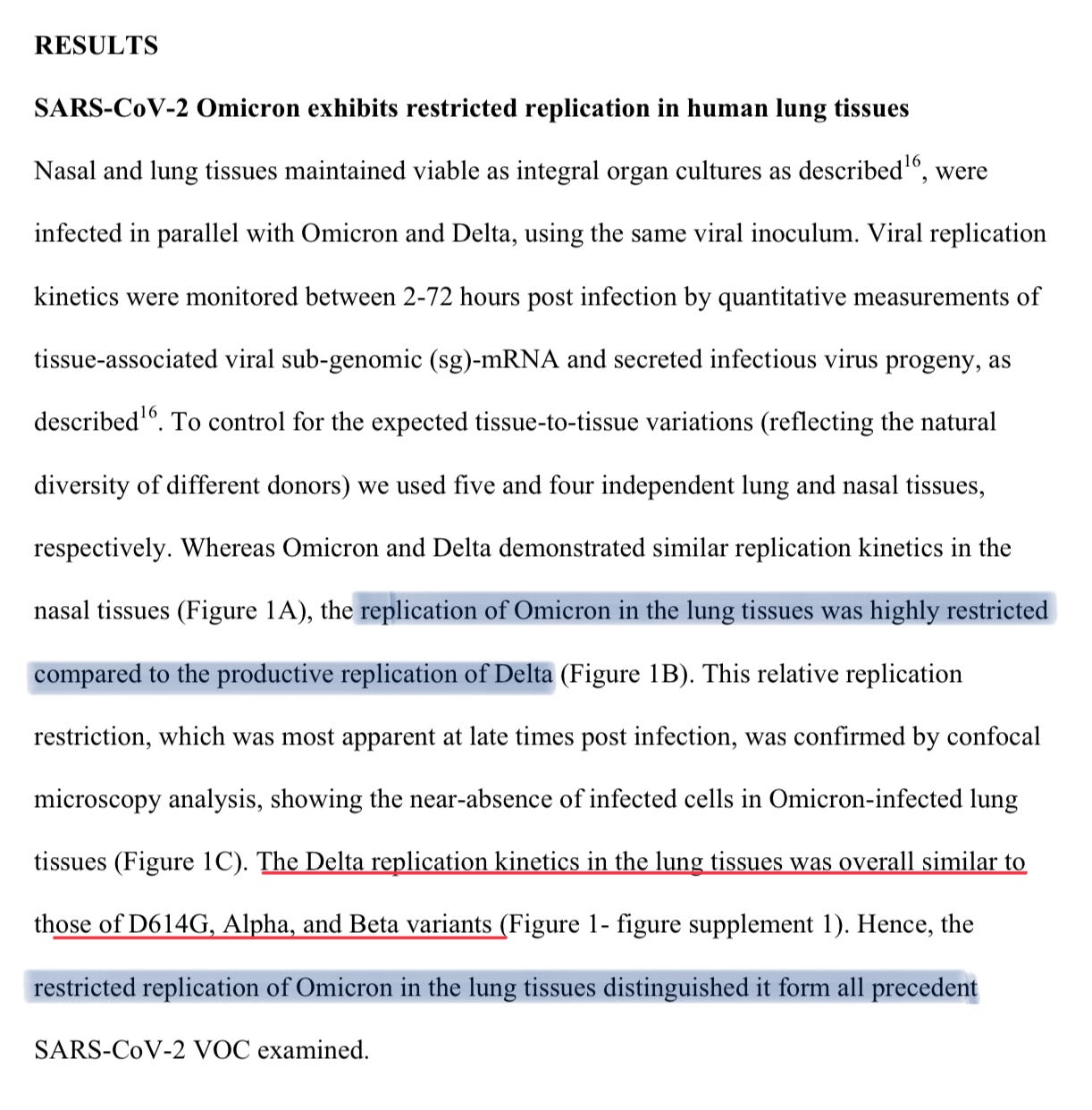
As I mentioned on Twitter many times, and DMs, Omicron was mild as in “it didn’t , kill your lungs fast” and here we have some of the evidence for that assertion. Omicron doesn’t replicate in the lungs compared to Delta. And all variants replicate similarly to Delta in the lungs, which makes Omicron fairly unique.
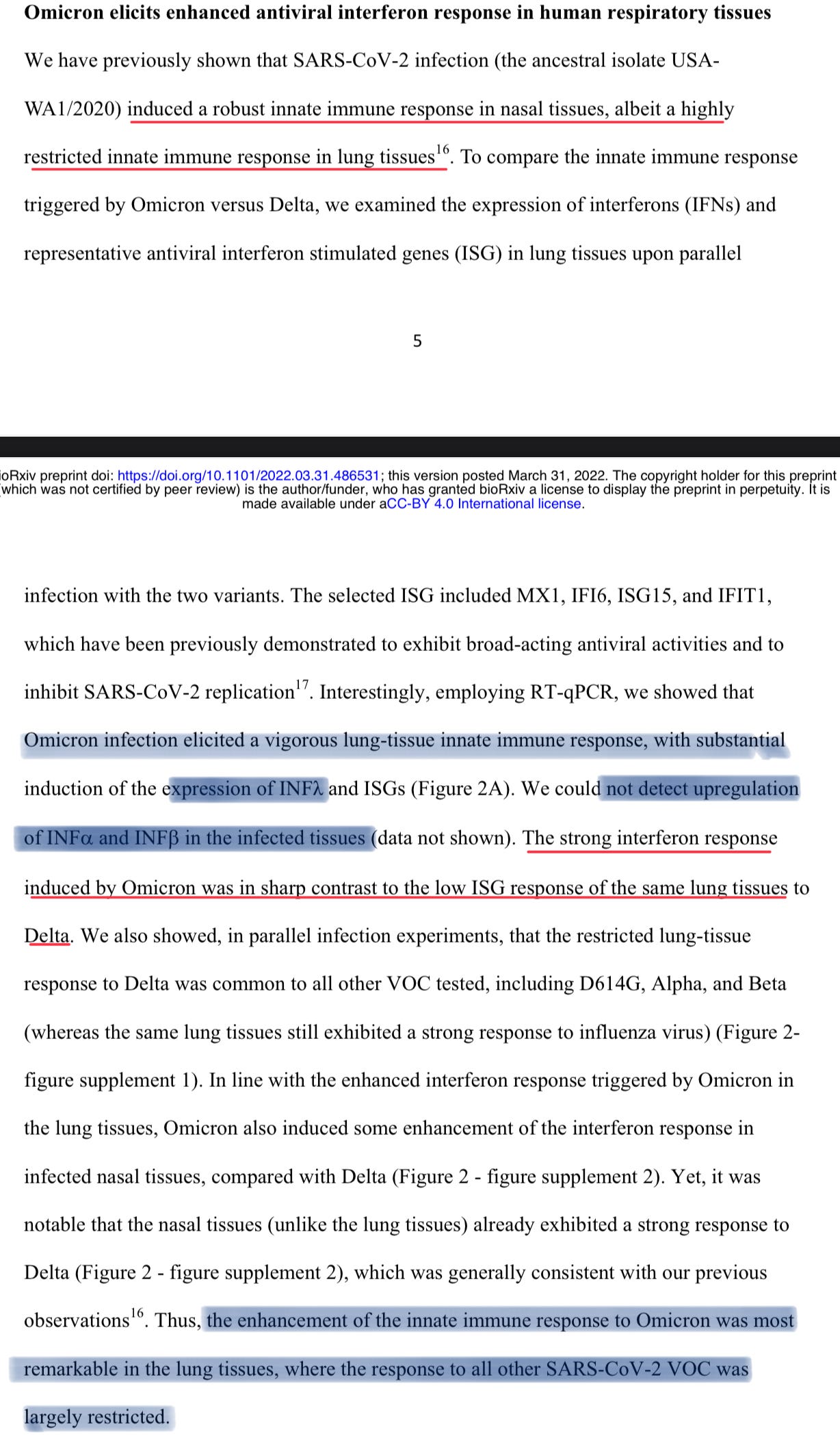
Previous SARS-CoV-2 variants (I do rather call them strains, I think its cooler…just venting), induced robust immune response in the nose (upper airways in a simplified way), but not in the lungs, which gave all the weird, systemic effects, and the coinfections often severe with different types of pneumonia. Again, and I said this multiple times, SARS-CoV-2 is a disease accelerator.
Omicron on the other hand elicited a very strong lung immune response, producing Interferon Lamba, which you want at the first stages (as Interferon Gamma, and Interleukin 12, you don’t want them at the wrong time, or too much for long), and they found no up regulation (producing more of) both Interferon Alpha, and Beta, two of the culprits at different stages of the infections of other variants, that drove the damage, and all the dysfunction I have been writing about. In a ironic way, it is somewhat the literal of the other SARS-CoV-2 variants… heh.
There are only trade-offs in nature, and I maintain my position, Omicron is not as mild, it just doesn’t inflict massive amounts of damage too fast. As long, you are healthy, and take supplements, it shouldn’t be a problem, neither the variants born from it too, for now. It will, however, be a concern among the vaccinated, as we all know.
At the end of the paper they say research is still needed, because no team has figured out how Omicron works, why it does what it does, and I agree, and am eager to see results from this line of inquiry.
Talking about vaccinated. Source.
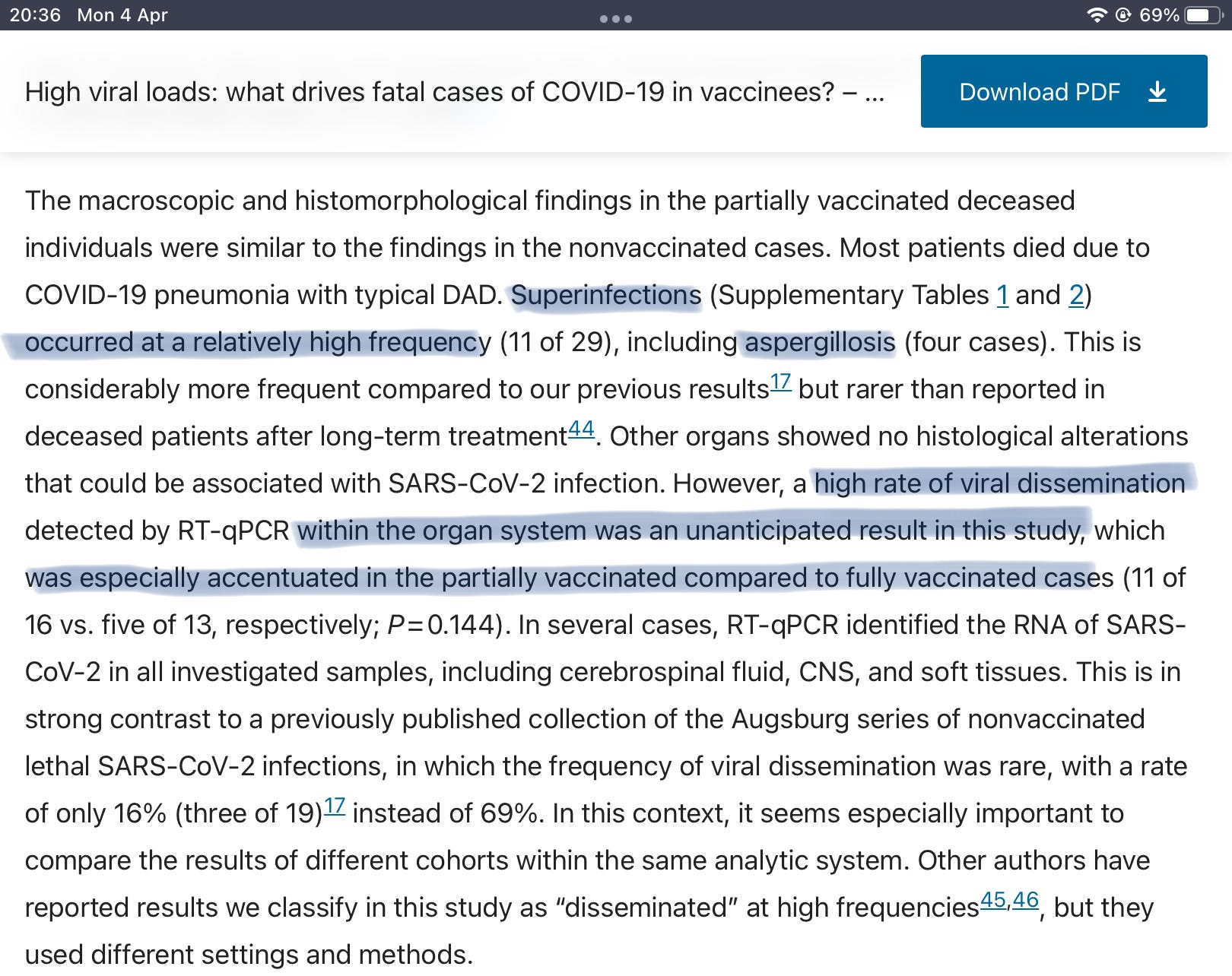
High viral loads in vaccinated individuals, something that I have been warning for. *check notes
Almost 2 years. When vaccinated individuals die, they find viral dissemination (that means there is virus elsewhere, not just the lungs, or airways, but in other organs too), which authors found more present in “partially vaccinated” individuals compared to fully. Which is bullshit.
I have written extensively about this, and “full vaccination” is merely a timing problem, because the antibodies wane incredibly fast. So, the effects being discussed here could be applied to any vaccinated person.
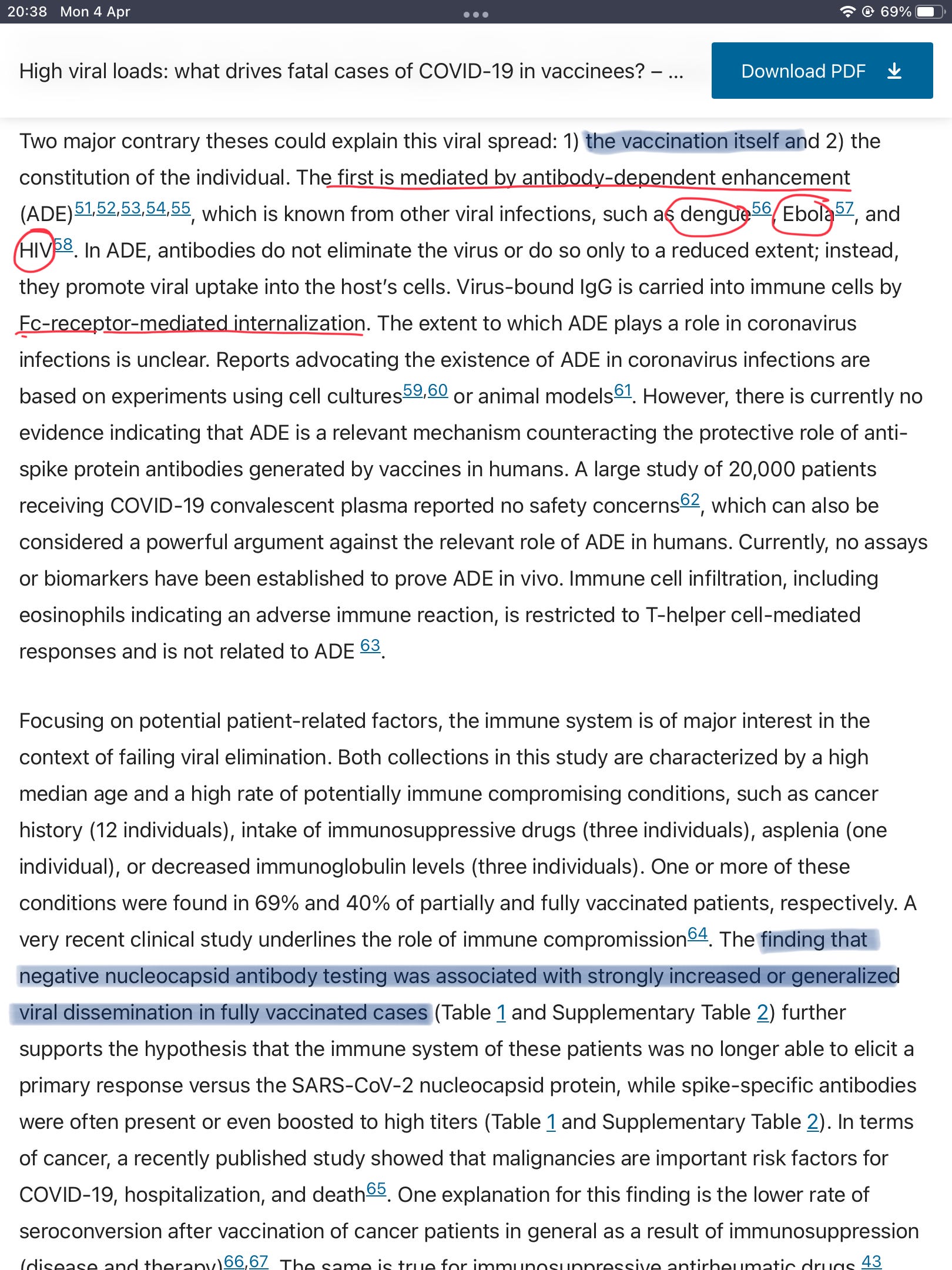
Another point I have brought up many times, we are seeing a uncategorized form of ADE in vaccinated individuals, and the vaccines are creating super-spreaders of supercharged variants. What I called Reverse Marek (will link the posts below, and given the current way this is headed, highly recommend you to read it). There are many possible mechanisms as to how viral load is being enhanced, and I believe pathology will soon follow in certain demographics.
In this post I comment on a paper about N protein. The post below, and the post referred inside it, will help you understand the broader picture. I might just try to make it into one big post, and add newer evidence later this month. In this post, you can find a screenshot from the UK government stating, vaccinated individuals can’t build an N protein response, nor “learn it”.
You can use Ko-Fi to buy me a coffee.
If you enjoy independent, complex, interdisciplinary analysis, and forecasting consider becoming a free or paying subscriber, support is very much appreciated. Sharing also helps me tremendously. Deep appreciation for all the supporters.
Hey man, thanks for the content. Your work is helping me see through the bullshit. Regarding the vaccine, me and my family got 2 doses because we thought that would help our older family members, none of us did the 3rd because everyone was being so pushy about it, thank god. I'm pretty sure we all had covid before the vaccines. Are we screwed? Or is it only the boosted people that are screwed? Or it depends on the person? Thanks for you time.