


SARS-CoV-2 - Impaired DNA repair, viral evolution, and secondary infections
"it's just mild heart inflammation bro"

I had a family emergency and a personal one, so sorry for taking a little longer on this one. There isn’t a lack of good, interesting papers on SARS-CoV-2 FYI.
For weeks, I have been saying that Omicron BA. 1 might be immune-suppressing people, and by now most subscribers are aware of the Reverse AIDS hypothesis, basically how the (main mRNA) vaccines cause a transient immune dysfunction. I will stick to both until evidence to the contrary is presented. A friend sent me this.
Hong Kong mortuaries hit capacity as Covid-19 deaths climb
“The storage space in hospital mortuaries has reached full capacity,” the authority told Reuters in an email.
Dozens of bodies are waiting in hospital accident and emergency rooms to be transported to mortuaries, said Tony Ling, head of the city’s Public Doctors Association.
South Korea has deadliest day of COVID-19 pandemic amid Omicron surge
Health workers diagnosed 166,209 new cases, which came close to Wednesday’s one-day record of 171,451 and represented more than a 37-fold increase from daily levels in mid-January, when Omicron first emerged as the country’s dominant strain.
I will maintain all my previous comments, inside all my virus posts, especially the Reverse Marek case, which clearly is real. Omicron isn’t that mild, it just doesn’t destroy your lungs and causes severe respiratory failure, especially at scale, BA. 2 blasts through all vaccine-elicited immunity, and even natural immunity in certain circumstances.
Everything will fall upon where the “wind” shifts (viral evolution). Of course, if you read all my other posts, you will most people have many other problems at hand.
Myocarditis and Pericarditis following COVID-19 Vaccination: Evidence Syntheses on Incidence, Risk Factors, Natural History, and Hypothesized Mechanisms
Adolescent and young adult males are at the highest risk of myocarditis after mRNA vaccination. Pfizer over Moderna and waiting more than 30 days between doses may be preferred for this population. Incidence of myocarditis in children aged 5-11 may be very rare but certainty was low. Data on clinical risk factors was very limited. Clinical course of mRNA related myocarditis appears to be benign although longer term follow-up data is limited. Prospective studies with appropriate testing (e.g., biopsy, tissue morphology) will enhance understanding of mechanism(s).
I personally do not understand many of these authors, I guess it should be expected not to go against the wave, otherwise, your funding gets pulled out, your university or research center starts pressuring you and your career grinds to a halt. Some researchers clearly prefer a clear conscious over research money, but not these.
There is extensive clinical evidence, and literature on how and the possible pathways the mRNA vaccines cause heart inflammation and damage, and the signals are all there, and if you wanted to be scientific about it and fast, you could either use a simplified Bayes approach or a Fermi approximation, among other analytical frameworks.
Also, given the current world evidence, and scientific literature on how the vaccines are useless against Omicron and young people don’t die, I see no point in telling anyone younger than 40 to get the jab, the younger, the pointless. Unless you want to damage them for life. But wait, it will get worse, pretty fast.
Time-Dependent Increase in Susceptibility and Severity of Secondary Bacterial Infection during SARS-CoV-2 Infection
Secondary bacterial infections can exacerbate SARS-CoV-2 infection, but their prevalence and impact remain poorly understood. Here, we established that a mild to moderate SARS-CoV-2 infection increased the risk of pneumococcal coinfection in a time-dependent, but sexindependent, manner in the transgenic K18-hACE mouse model of COVID-19. Bacterial coinfection was not established at 3 d post-virus, but increased lethality was observed when the bacteria was initiated at 5 or 7 d post-virus infection (pvi). Bacterial outgrowth was accompanied by neutrophilia in the groups coinfected at 7 d pvi and reductions in B cells, T cells, IL-6, IL-15, IL-18, and LIF were present in groups coinfected at 5 d pvi. However, viral burden, lung pathology, cytokines, chemokines, and immune cell activation were largely unchanged after bacterial coinfection. Examining surviving animals more than a week after infection resolution suggested that immune cell activation remained high and was exacerbated in the lungs of coinfected animals compared with SARS-CoV-2 infection alone. These data suggest that SARS-CoV-2 increases susceptibility and pathogenicity to bacterial coinfection, and further studies are needed to understand and combat disease associated with bacterial pneumonia in COVID-19 patients.
The role of secondary infections in SARS-CoV-2 has been clinically known for a long time, almost since Q3 2020, but it was swept under the rug after a while, but there is extensive evidence out there.
Here, in a rat model, the authors demonstrate that after a very short time post-infection, patients with the mild or moderate disease have a higher chance to acquire a secondary bacterial infection.
The bacterial infection was subclinical until 5 days post-viral infection (PVI in the paper), higher lethality after 5 and 7 days was found.
Reduction of reductions in B cells, T cells, IL-6, IL-15, IL-18, and LIF were present after 5 days, which literally means a co-infection will literally immune suppress you.
In general, viral-bacterial coinfections are not uncommon, where S. aureus and pneumococcus are widely documented as complicating pathogens during infection with other viruses, most notably influenza A virus (IAV)Reviewed in 35–46. During influenza pandemics, 45-95% of the mortality has been attributed to bacterial coinfections47–50.
Some host responses also differ in timing and magnitude, including the delayed type I interferon (IFN-α,β), increased proinflammatory cytokines like TNF-a and IL-6, and reduced immune regulation that have been detected in COVID-19 patients62–66. Further, neutrophils and macrophages, which are important for efficient bacterial clearance during viral-bacterial coinfection67–72, are dysregulated during COVID-1973–75. Thus, the potential for bacterial invasion during SARS-CoV-2 infection may also differ from that observed in influenza infection with respect to timing and host-pathogen mechanisms.
The first paragraph is pretty self-explanatory, and I would like the reader to keep in mind (and preferably go read Reverse AIDS Part II - The Toll of TLR). The second paragraph explains the higher inflammatory responses that the reader should be used to seeing by now and immune suppression.
Do you know what makes a SARS-CoV-2 co-infection similar to the influenza-bacteria one historically seen ? Messing with Toll-Like Receptors. And of course, I wouldn’t be me if…

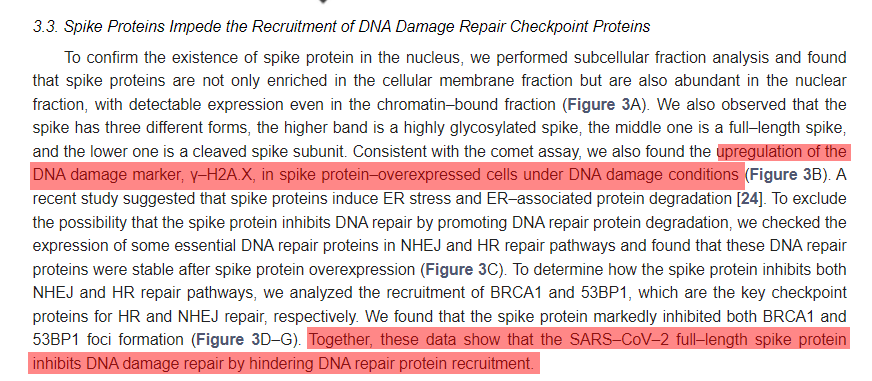
SARS–CoV–2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro
Severe acute respiratory syndrome coronavirus 2 (SARS–CoV–2) has led to the coronavirus disease 2019 (COVID–19) pandemic, severely affecting public health and the global economy. Adaptive immunity plays a crucial role in fighting against SARS–CoV–2 infection and directly influences the clinical outcomes of patients. Clinical studies have indicated that patients with severe COVID–19 exhibit delayed and weak adaptive immune responses; however, the mechanism by which SARS–CoV–2 impedes adaptive immunity remains unclear. Here, by using an in vitro cell line, we report that the SARS–CoV–2 spike protein significantly inhibits DNA damage repair, which is required for effective V(D)J recombination in adaptive immunity. Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site. Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.
This is a very good and important paper that I barely saw around either Substack or Twitter (granted I didn’t look too much in Twitter lol).
Using an in-vitro (cell line, not living beings) this paper shows that SARS-CoV-2 spike protein inhibits DNA repair damage, which is required for V(D)J in adaptive immunity.
V(D)J is a fairly complex part of immunity. From Wikepedia.
V(D)J recombination in mammals occurs in the primary lymphoid organs (bone marrow for B cells and thymus for T cells) and in a nearly random fashion rearranges variable (V), joining (J), and in some cases, diversity (D) gene segments. The process ultimately results in novel amino acid sequences in the antigen-binding regions of immunoglobulins and TCRs that allow for the recognition of antigens from nearly all pathogens including bacteria, viruses, parasites, and worms as well as "altered self cells" as seen in cancer.
In a crude way, this is a process to create antigen-binding sites, the little Y things that grab parts of any foreign invader and start an immune response. So by directly impacting this, it impacts your entire adaptive immune response.
They found Spike protein inside the nucleus of the cells they used to test and it impaired the recruitment (calling in basically) of two very significant proteins for DNA repair.
Therefore, the inhibitory effect of Nsp1, Nsp5, Nsp13, and Nsp14 on DNA damage repair may be due to secondary effects, such as growth arrest and cell death. Interestingly, overexpressed spike protein did not affect cell morphology or proliferation but significantly suppressed both HR and NHEJ repair (Figure 1B–E, Figures S2A,B and S3A,B).
Here they tested specific parts of the virus, called Non-Structural Proteins, and deduce it might be due to secondary effects, such as slower growth and cell death. In my opinion, one of the main reasons might be the few papers I shared previously, the mitochondria ones. Mitochondrial function is essential for life itself, and normal physiological function. The spike itself affects mitochondrial function.
In contrast, our data provide valuable details on the involvement of spike protein subunits in DNA damage repair, indicating that full–length spike–based vaccines may inhibit the recombination of V(D)J in B cells, which is also consistent with a recent study that a full–length spike–based vaccine induced lower antibody titers compared to the RBD–based vaccine [28]. This suggests that the use of antigenic epitopes of the spike as a SARS–CoV–2 vaccine might be safer and more efficacious than the full–length spike. Taken together, we identified one of the potentially important mechanisms of SARS–CoV–2 suppression of the host adaptive immune machinery. Furthermore, our findings also imply a potential side effect of the full–length spike–based vaccine. This work will improve the understanding of COVID–19 pathogenesis and provide new strategies for designing more efficient and safer vaccines.
This paragraph speaks for itself. If proven right, tested in vivo (and I believe it is right at some level, given all the evidence you could gather, even here in my Substack), and it doesn’t bode well for any of the vaccines using the spike protein.
Waning of SARS-CoV-2 booster viral-load reduction effectiveness
The BNT162b2 COVID-19 vaccine has been shown to reduce viral load of breakthrough infections (BTIs), an important factor affecting infectiousness. This viral-load protective effect has been waning with time post the second vaccine and later restored with a booster shot. It is currently unclear though for how long this regained effectiveness lasts. Analyzing Ct values of SARS-CoV-2 qRT-PCR tests of over 22,000 infections during a Delta-variant-dominant period in Israel, we find that this viral-load reduction effectiveness significantly declines within months post the booster dose. Adjusting for age, sex and calendric date, Ct values of RdRp gene initially increases by 2.7 [CI: 2.3-3.0] relative to unvaccinated in the first month post the booster dose, yet then decays to a difference of 1.3 [CI: 0.7-1.9] in the second month and becomes small and insignificant in the third to fourth months. The rate and magnitude of this post-booster decline in viral-load reduction effectiveness mirror those observed post the second vaccine. These results suggest rapid waning of the booster’s effectiveness in reducing infectiousness, possibly affecting community-level spread of the virus.
Another myth down the drain, which anyone with a functional brain already knew. The vaccine does NOT stop viral replication, and even post-booster it wanes really fast, within two months, you basically produce the same amount of virus as before the vaccine and spreads to your community. Otherwise, nothing worth in this paper besides this.
Now we just need to wait for one researcher or team to prove that the vaccine, after 50 days, actually enhances viral replication, creating the Reverse Mareks scenario I proposed. This leads us to one of my oldest points about the useless vaccines.
Emergence of Progressive Mutations in SARS-CoV-2 From a Hematologic Patient With Prolonged Viral Replication
We documented a hematologic patient with prolonged SARS-CoV-2 viral replication in whom emergence of viral mutations was documented after the consecutive use of antivirals and convalescent plasma. The virus detected in the last of 12 clinical samples (day 237) had accumulated 22 changes in amino acids and 29 in nucleotides. Some of these changes, such as the E484Q, were mutations of concern as defined by WHO. This finding represents an enormous epidemiological threat and poses a major clinical challenge. Combined antiviral strategies, as well as specific strategies related to the diagnostic approach of prolonged infections for this specific population, may be needed.
Prolonged, persistent, dare I say chronic, viral infection with SARS-CoV-2 in an immunocompromised patient led to a change in the virus, even acquiring one of the “concerning” mutations accord to the WHO.
There is an argument to be made that immuno-compromised patients are evolutionary dead-ends for viral infections since the virus will evolve to survive, but not transmit, among other observations by a molecular biologist 10x smarter than me, but that is beside the point I want to raise here.
What happens when your vaccine immuno suppress your population, while not slowing the spread, and putting a selective pressure via non-neutralizing antibodies and poor/impaired immune response ?
Among the first to warn about this, and I will be proven right on every single point, regardless of how insane it may sound.
Vaccines drove the viral evolution of every other variant besides Alpha and Omicron, that is my personal opinion.
Appreciate all the supporters and the new subscribers. Sharing this post helps me tremendously. I wish you all a great Sunday.
Another great post, thanks. The last part reminded me of a modeling study.. although they won't have factored in the more recent immunosuppression ideas. Even back then, high transmission plus a highly vaccinated population was the recipe for variant emergence. As I'm sure has happened everywhere, we've had the media and public health officials, and subsequently the public, constantly accuse the unvaccinated of being the variant factories and spreaders of disease..how ironic that the opposite is emerging. Won't hold my breath for an apology, though.
https://www.nature.com/articles/s41598-021-95025-3
Thanks for all your hard work. My daughter has gotten vaxxed at the behest of employers/college and of course, I found out after the fact. Her mother is a healthcare worker and she's beyond complacent about medication harms. In the bountiful world of vax-induced health disaster, one thing that's worrying me most is cancer.
https://twitter.com/JikkyKjj/status/1500282669724495873