
SARS-CoV-2, CD48, Remdesivir resistance, and Omicron chimerism
Soluble proteins are kinda important.

First, what is this CD48 thingy ? CD48 is a signaling protein, an antigen that helps differentiate (makes certain naive cells into specific ones), and its bound (glued) to the cell membrane.
It can affect the expression of cytokines, etc. It is a very important molecule in both health, and disease.
COVID-19 patients have increased levels of membrane-associated and soluble CD48
Soluble proteins are proteins that can freely “move” around the cell, in a crude manner. They can also be a problem, like the soluble form of the Spike Protein from SARS-CoV-2. For that to happen though, it needs to be truncated, biology term for misshapen, shorter. As one could guess, a soluble protein, specially a signaling one, can and will have systemic effects.
Authors find that the soluble form of CD48 is severely increased in any person infected with SARS-CoV-2.
Just want to leave my indignation, and outright rage, on the matter of researchers naming the same proteins 16 different names.
Here the authors are explained their thought process, and previous research, and state in an asthma model, the levels of CD48 were not correlated with a Th2 (Th2 are usually allergic reactions), or with specific interleukins.
sCD48 found to be higher in some viral infections, and I highlighted the most pertinent one, which I mentioned more than once here, EBV. I will come back to hematopoietic cells later.
If you want to understand the significance of IFN gamma, you should read this. I have argued that this specific Interferon response, and its byproducts are responsible for a good portion of the damage, and disease acceleration in many of the vaccinated, and also in a smaller portion of the unvaccinated, but infection. In comparison to the vaccinated, this number is 2 orders of magnitude smaller.
I find it fascinating that, whenever they find a new, unique marker, or physiological effect not seen in other respiratory viral infections, HIV mentioned somewhere. I have covered how the Spike Protein alone can damage hematopoietic cells, and it is very pertinent.
My argument here is the following, the Spike itself is upregulating CD48, and the viral infection adds fuel to the fire.
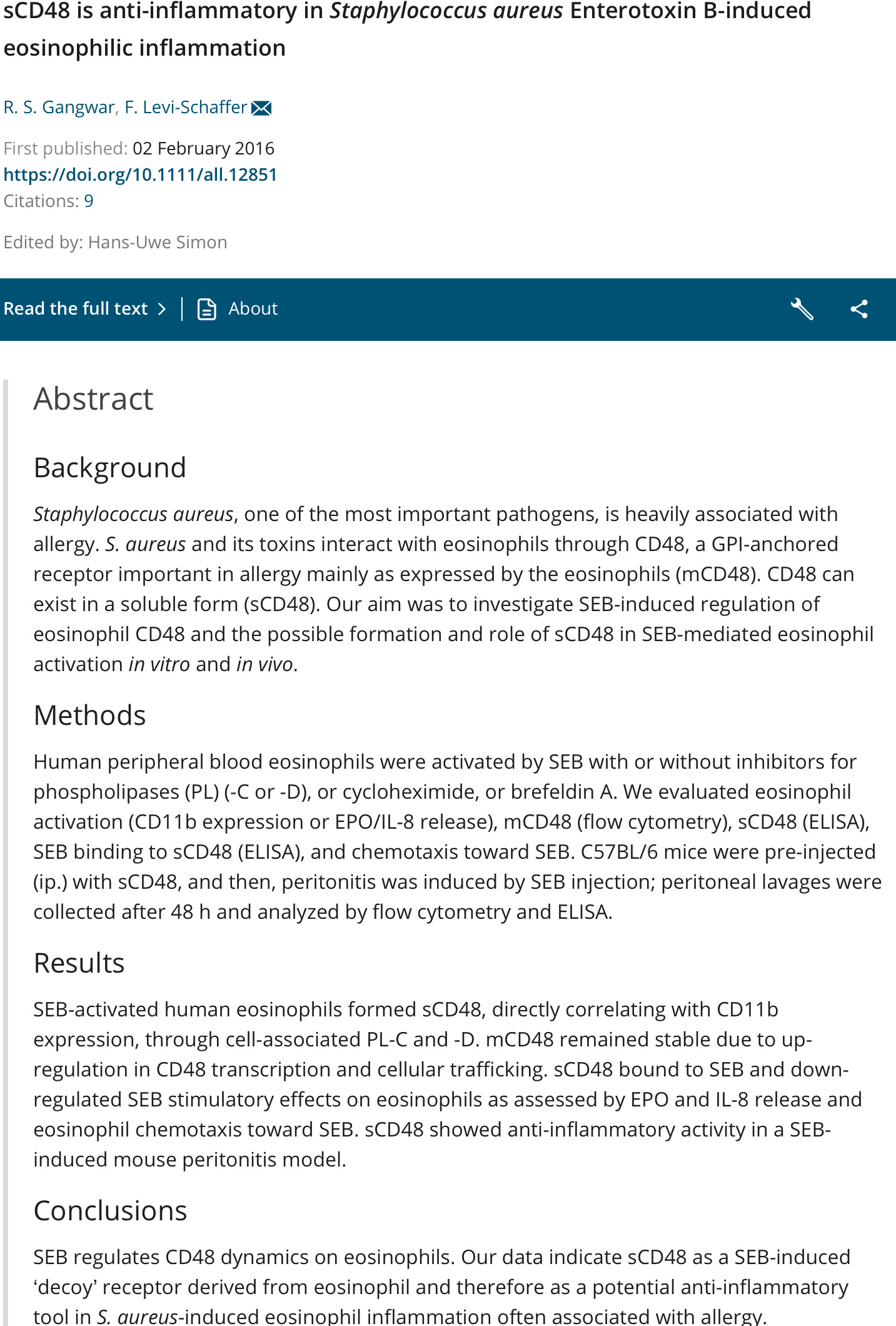
SARS-CoV-2 has a SEB motif, you can deduce the rest.
Engagement of SLAMF2/CD48 Prolongs the Time Frame of Effective T Cell Activation by Supporting Mature Dendritic Cell Survival
This paper is a little difficult to understand, but simplifying CD48 (they used the other name here, SLAMF2) can be used by Dendritic Cells as a survival molecule, protecting them from early cell death. It helps the DCs not to produce large amounts of type I Interferon, specially Beta.
So in the regards of the viral infection, this can be one of the pathways your body uses to regulate and modulate the immune response, trying not to shift it too hard to the wrong side.
Just for posterioty sake, a couple of interesting papers.
De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: a case report
SARS-CoV-2 remdesivir resistance mutations have been generated in vitro but have not been reported in patients receiving treatment with the antiviral agent. We present a case of an immunocompromised patient with acquired B-cell deficiency who developed an indolent, protracted course of SARS-CoV-2 infection. Remdesivir therapy alleviated symptoms and produced a transient virologic response, but her course was complicated by recrudescence of high-grade viral shedding. Whole genome sequencing identified a mutation, E802D, in the nsp12 RNA-dependent RNA polymerase, which was not present in pre-treatment specimens. In vitro experiments demonstrated that the mutation conferred a ~6-fold increase in remdesivir IC50 but resulted in a fitness cost in the absence of remdesivir. Sustained clinical and virologic response was achieved after treatment with casirivimab-imdevimab. Although the fitness cost observed in vitro may limit the risk posed by E802D, this case illustrates the importance of monitoring for remdesivir resistance and the potential benefit of combinatorial therapies in immunocompromised patients with SARS-CoV-2 infection.
I have mentioned before how Omicron can evade most of the monoclonal antibodies in use today, and here is an intriguing paper. As anyone with a cursory understanding of biology could expect, using a single type of treatment, with a narrow target would elicit selective pressure, and here they actually found in vivo, in a patient, one of said mutation.
This stands for an argument of not using only one treatment option, be them drugs, or supplements, but a wider approach.
Omicron: a chimera of two early SARS-CoV-2 lineages
It is known that the SARS-CoV-2 Omicron variant encodes 37 amino acid substitutions (including insertions and deletions) in the spike protein, and then the recombination event alone leads to 22 of them. Spike protein is the most crucial structural protein of SARS-CoVs. It plays a pivotal role in viral attachment, fusion, and entry and is also a target for developing antibodies, entry inhibitors, and vaccines. The recently emerged substitutions within the SARS-CoV-2 Omicron variant thereby raised concerns about the effectiveness of available vaccines and antibody therapeutics. It has been reported that these substitutions have led to some subtle variations in the spatial structure and the affinity to the hACE2 receptor of the spike protein.5 More importantly, it has caused the immune escape of the Omicron variant to the available vaccines and antibody therapeutics
I found this paper mildly interesting it, and since I already introduced the recombination aspect of the virus to my readers, I decided to share this one.
At some level I agree with the conclusion, and some evidence in this paper, just disagreee with some assertions and conclusions from the authors. Omicron is clearly a lab leak, to what purpose and to what effect, we can onlye guess. Alas, recombination by using different, ancient strains to achieve a specific goal (attenuation of severity of disease, and some ofthe nasty antigenic sites like the SEB one) would be easier to achieve by recombination, and not seamless techniques (what they used on SARS-CoV-2). Perhaps additionally after the recombinatory events.
The immune escape was inevitable, since billions imprinted with the ancestral strains via vaccine, and millions with natural infection, broader, leading to a very mild disease course, but would escape too.
I have another paper to share, but this is already complicated enough with the CD48, specially if you go read the hematopoietic post. I will finish writing it, and releasing tomorrow.
If you enjoy or take value from my independent, interdisciplinary analysis, consider becoming a free or paying subscriber, my work is fully support by you. Sharing also helps me tremendously. I truly appreciate all supporters.
So SC2 upregulates CD48 too, CD38 was enough for it being bad, what else are we going to find out?