

Omicron evasion, SARS-CoV2 and the brain
Omicron evasion, SARS-CoV2 and the brain
"Does it feel good to being proved right every day lately ?"

Today we will have a somewhat different post. I won’t cover the papers here in length unless someone asks for a more detailed write-up on a specific paper, but there will be enough resources for you to spend some time digging. I have covered similar topics extensively, so I see no reasons to dig as deep as some other pieces, but I do feel these deserve attention.
The paper below is directly correlated with this piece and the others linked inside, if you want a deep dive, be sure to read it.

Differential Evasion of Delta and Omicron Immunity and Enhanced Fusogenicity of SARS-CoV-2 Omicron BA.4/5 and BA.2.12.1 Subvariants
The rising case numbers of the SARS-CoV-2 Omicron BA.4, BA.5, and BA.2.12.1 subvariants has generated serious concern about the course of the pandemic. Here we examine the neutralization resistance, infectivity, processing, and fusogenicity of spike from the BA.4/5 and BA.2.12.1 SARS-CoV-2 variants compared with other Omicron subvariants and Delta. Critically, we found that the new Omicron subvariants BA.4/5 and BA.2.12.1 were more resistant to neutralization by mRNA-vaccinated and boosted health care worker sera and Omicron-BA.1-wave patient sera than were the BA.1 and BA.2 variants. Interestingly, Delta-wave patient sera neutralized more efficiently against not only Delta but also BA.4/5 and BA.2.12.1 variants that also contain substitutions at position L452, similar to Delta. The BA.4/5 and BA.2.12.1 variants also exhibited higher fusogenicity, and increased spike processing, dependent on the L452 substitution. These results highlight the key role of the L452R and L452Q mutations in BA.4/5 and BA.2.12.1 subvariants.
Again, no surprise here if you read my Substack for a few months now, especially more recent posts. Following a similar trend that other papers look upon (I had to triple check that this paper was indeed new… that is how much interest these mutations and subvariants have right now), in which the L452 mutation grants higher transmissibility and fusogenicity (glues cells together) and how it is important for the spread and immune evasion of this variants.
A finding that I found remarkable was the fact that Delta-wave patient’s sera (blood) could neutralize BA. 4/5 and BA.2.1 (the respective of BA.4 and 5 in the US in simple terms) and they argue it is because of this mutation (Delta originally had this mutation).
The authors go further on to describe the resistance of these subvariants to vaccine-elicited antibodies and immunity and how good a booster performs, which I won’t bother to debunk further. Well, I will by analyzing another paper after this. Which is in line with this particular paragraph.
Of note, differences between the NT50 values of BA.4/5, BA.2.12.1 and that of two single mutants became less apparent in vaccinated Delta-wave patients compared to unvaccinated Delta-wave patients , again indicating that breakthrough infection plus COVID-19 vaccination can offer not only enhanced but also broader protection against the Omicron sub-lineage variants.
Overall, these results revealed that the BA.1-wave infection does not seem to offer effective protection against the new emerged sub-lineages BA.4/5 and BA.2.12.1, especially BA.4/5, but a 3-dose booster mRNA vaccination can overcome the deficiency.
They go to further describe other points already covered in other pieces, but I would like to point out that the authors themselves found that while BA. 4 and 5 and BA.2.1 have the same mutation as Delta, it didn’t lead to similar dynamics, and one could argue it is because of previous immunity to that particular mutation. (They keep pushing the useless mRNA vaccines, how tiresome though).
Reduced neutralizing antibody potency of COVID-19 convalescent vaccinated plasma against SARS-CoV-2 Omicron variant
Convalescent Plasma means the liquid part of the blood of someone who recovered from an infection, the V here stands for vaccinated.
Similar to everything covered so far even the plasma of recovered vaccinated individuals have trouble neutralizing Omicron, and it the best approach would be to use the plasma of recently recovered Omicron infected, but this isn’t precisely why I shared this paper, but the following.
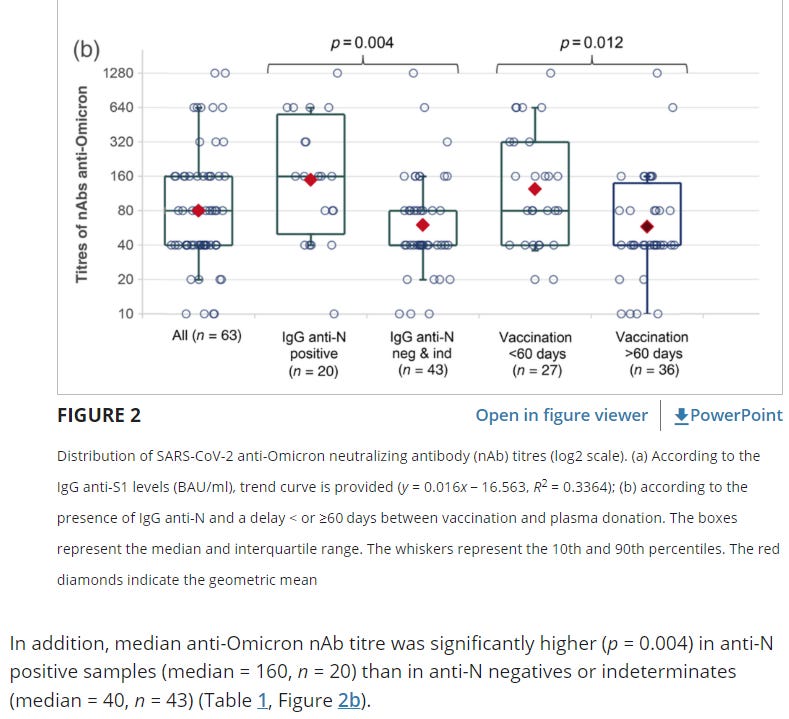
Another one of the massive piles of evidence on the importance of the Nucleocapsid Protein. As much as antibodies are a very poor metric to measure immunity, this one gives circumstantial evidence to a further developing thesis. The N protein is really important in dealing with the infection, and a lot of the vaccinated have a poor conversion rate towards developing anti-N protein immunity.
But unlike some, I don’t jump to conclusion, and so far the evidence shows that yes, the vaccinated can develop immunity towards the N protein, but the seroconversion (infected, recovering, and acquiring immunity) is poor, on average 40% of the vaccinated don’t develop, so you need new infections. The real question is, at what cost ?
As long as you take care of yourself and take supplements, and everything else, you will be fine. And finally, about to prove myself correct again. One argument of a certain subset of “writers” here and on Twitter was that Covid will directly lead to neurodegeneration. And I often said it wouldn’t, not on a systemic level, but would accelerate it. Pathogenesis (meaning development of a new disease) is entirely different from Pathogenic acceleration (I call it in some places Hermesian Pathogenic State heh…)
I have always argued this state would be driven by mitochondrial dysfunction, ferroptosis, and oxidative stress. I have many tweets arguing about it.
COVID-19 infection enhances susceptibility to oxidative-stress induced parkinsonism
(this research was done in mice to be clear)
Background Viral induction of neurological syndromes has been a concern since parkinsonian-like features were observed in patients diagnosed with encephalitis lethargica subsequent to the 1918 influenza pandemic. Given the similarities in the systemic responses following SARS-CoV-2 infection with those observed after pandemic influenza, there is a question if a similar syndrome of post-encephalic parkinsonism could follow COVID-19 infection.
Results K18-hACE2 mice infected with SARS-CoV-2 or MPTP showed no SNpc DA neuron loss following MPTP. In mice infected and recovered from SARS-CoV-2 infection, MPTP induced a 23% or 19% greater loss of SNpc dopaminergic neurons than SARS-CoV-2 or MPTP, respectively (p < 0.05). Examination of microglial activation showed a significant increase in the number of activated microglia in both the SNpc and striatum of the SARS-CoV-2 + MPTP group compared to SARS-CoV-2 or MPTP alone.
First for clarification, what the hell is MPTP. MTPT is the drug form of MPP+ (1-methyl-4-phenylpyridinium) It is a neurotoxin that acts by interfering with oxidative phosphorylation in mitochondria by inhibiting complex I, leading to the depletion of ATP and eventual cell death. It is widely used as a model in Parkinson research.
SNpc is a part of the brain, and its cells are highly important, here an amazing paper on the subject in relation to what the paper will discuss further down.
What does all this science talk means ? That SARS-CoV-2 has a synergistic effect with this neurotoxin. It leads to a greater loss of neurons than these alone and also there is a significant increase in the microglia (immune cells of the brain) than virus or the neurotoxin alone. This is one of the mechanisms for the progression of neurodegeneration, the presence, and activity of microglia in the brain, progressive (low-grade) inflammation, further exacerbating conditions for the progression of the disease.
Prior infection with SARS-CoV-2 increases neuroinflammation
In the SNpc, infection with SARS-CoV-2 (with or without MPTP) resulted in no change from controls animals in the total number of microglia in any of the 3 experimental groups
However, when we quantified resting vs activated microglia individually, we observed significant differences between groups. Overall differences were seen in both the number of resting microglia as well as activated microglia.
In regard to resting microglia, we measured a significant 36% reduction in the SARS-Cov-2+MPTP group compared to the vehicle, SARS-CoV-2 alone or MPTP alone. Quantitation of active microglia showed that SARS-CoV-2 infection or MPTP alone did not induce a significant increase compared to vehicle. We observed a 308% (p<0.002) increase in the SARS-CoV-2+MPTP group compared to vehicle and a 232% increase compared to SARS-CoV-2 alone (p<0.006)
Authors demonstrate that SARS-CoV-2 alone didn’t change the number of microglia with or without the neurotoxin, but there was a difference between resting (doing nothing) and activated microglia when compared to SARS-CoV-2 or the neurotoxin alone. In the presence of the neurotoxin, SARS-CoV-2 has the possibility of inducing a much more extensive progression of symptoms than the viral infection alone, leading to my former months-old observation of disease acceleration, not creation.
How does that works ? The authors will explain it to you, and I will further detail it. For clarification, the authors correlate this pandemic with the 1918 pandemi a lot, which I find valid, especially in the scenario they propose.
Both influenza and SARS-CoV-2 are respiratory viruses, both infect epithelial cells in the lung and gut and both the 1918 H1N1 influenza virus and SARS-CoV do not appear to have significant inherent neurotropic potential. Both the 1918 influenza and SARS-CoV-2 appear to induce an enhanced program of induction of pro-inflammatory cytokines and chemokines, known as a cytokine storm. These circulating peripheral cytokines and chemokines can easily penetrate the blood-brain barrier through capillary beds as well as communicate with brain parenchyma through brain glymphatics. Once these inflammatory proteins are in the brain, they have been shown to activate the innate immune system of the brain, (microglia and astrocytes) which also begin to secrete inflammatory proteins that have been shown to sensitize neurons to later insults
The cellular composition of the SNpc, which is the main CNS region that degenerates in PD, is unique, in that it contains the highest ratio of microglia:neurons within the CNS. This skewed microglia:neuron ratio places the SNpc at a higher risk for reactive oxygen induced damage and disruption of mitochondrial function. This cellular damage does not necessarily have to lead to an immediate effect, but can result in neurons having a long-term diminished capacity to handle insults. i.e the “hit and run” effect. This would then lead cells to have a lower threshold for survival following future insults that could include any other agent/environmental exposure or even genetic sensitivity associated with PD.
Here you have a couple of the mechanisms of how these changes and many of the neurologic symptoms appear in people. I will further explain in simplified terms.
Once any part of your body, but especially your brain gets disrupted by something (in this case a viral infection), a few of the mechanism that will lead to brain inflammation is those inflammatory proteins moving around and reaching the brain, others are slightly more complex, as parts of the virus getting in the brain (there is evidence for these, it is not systemic btw, not that common). In the presence of inflammation or foreign invaders (or pieces of a pathogen that elicit an immune response), the immune system will activate to fight it, and clean the region, and this leads to the consumption of resources and inflammation.
Inflammation in your brain is tricky, if it is too much, it will create Oxidative Stress and disrupt the entire brain's biochemistry, and disrupt the proper function of mitochondria, which are essential for the body, but in your brain, it is a matter of being alive or “sleeping sickness”.
It is not that SARS-CoV-2 will cause diseases, but further sensitize your entire body to whatever you are predisposed to, or it is subclinical (meaning undetectable because it is not a perceptible problem yet). My argument for a long time. As time goes by I will further be proved right.
One final note is that a portion of the Long Covid has either too much N protein in their brains or nothing at all. (Fasting WILL help with both of these states).
I know the more anxious among my readers might get a little… well, anxious, but I already addressed these in my Things Hidden series post, pinned in this Substack. Fasting, and large doses of antioxidants after any viral infection (preferably NAC, or liposomal Glutathione, with Vitamin C every 4 hours) will protect and correct most of it. If you have neurological symptoms after these, you just need to supplement certain nutrients and 99% of the time it “fixes it”. Fasting is powerful because of the many mechanisms involved in this. The aforementioned piece.
For last, this is another way Covid will do what the paper (and myself) described.
From here.
Tryptophan and nicotinamide deficiencies fall within the protein energy malnutrition (PEM) spectrum. They can arise if the kynurenine pathway is stressed by primary or secondary inflammatory conditions and the consequent imbalance of available catabolic/anabolic substrates may adversely influence convalescent phase efficiency. The replacement of depleted or reduced NAD+ levels and other cofactors can perhaps improve the clinical management of these disorders.

My mitochondria pieces would be a good starting point too !

As a final reminder, every first day of the month, something the first 2, I help my mother and grandmother get situated for the entire month, perhaps no posts, or very short ones, I will reply to messages and e-mails the same though. Hope you all have a fantastic evening.
Deep appreciation for all the supporters, you make this possible!
This info on microglia is fascinating and very valuable as is the inflammation aspect.
I have recommended NAC as well as more standard vitamin and nutritional supplements for elderly SARS-CoV-2 positive patients suffering from mental confusion/fog and in multiple cases, have received positive confirmation of it reducing symptoms.
This was in patients receiving ivermectin, HCQ, and not, as well as patients receiving follow up treatment for bacterial lung infection.
What is confusing the amyloid proponents is 1. The exact or even a hypothesized mechanism 2. Not realizing that systemic inflammation through alteration of the extracellular matrix results in pathological processes in and of itself. I have an idea the ultimate answer to this disease will have a silver lining and that it will be extensible to other chronic diseases of aging.
You are correct about ROS. Excessive ROS can by itself lead to mitochondrial dysfunction. The pathways you are talking about are consistent with this.
I got a 7 day ban from Twitter right after talking about the paper I am working on. If you have any ideas where to submit this I would appreciate it. I am retired and not affiliated with any university. I think this will be some obstacle. I have recently applied for membership as a contributor at the Am J Resp and CC Med.