

This post below and the whole Marek series will be fairly important in the coming months, as the exact scenario I proposed will come to pass, at least I see high probability of it.
A new Beyond Mathematical Odds coming tomorrow. I like doing a long analysis, rather than flooding your inboxes with emails. For iPhone users, Substack now has an app.
Omicron BA.2 (B.1.1.529.2): high potential to becoming the next dominating variant
Omicron variant of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has rapidly replaced the Delta variant as a dominating SARS-CoV-2 variant because of natural selection, which favors the variant with higher infectivity and stronger vaccine breakthrough ability. Omicron has three lineages or subvariants, BA.1 (B.1.1.529.1), BA.2 (B.1.1.529.2), and BA.3 (B.1.1.529.3). Among them, BA.1 is the currently prevailing subvariant. BA.2 shares 32 mutations with BA.1 but has 28 distinct ones. BA.3 shares most of its mutations with BA.1 and BA.2 except for one. BA.2 is found to be able to alarmingly reinfect patients originally infected by Omicron BA.1. An important question is whether BA.2 or BA.3 will become a new dominating “variant of concern”. Currently, no experimental data has been reported about BA.2 and BA.3. We construct a novel algebraic topology-based deep learning model trained with tens of thousands of mutational and deep mutational data to systematically evaluate BA.2’s and BA.3’s infectivity, vaccine breakthrough capability, and antibody resistance. Our comparative analysis of all main variants namely, Alpha, Beta, Gamma, Delta, Lambda, Mu, BA.1, BA.2, and BA.3, unveils that BA.2 is about 1.5 and 4.2 times as contagious as BA.1 and Delta, respectively. It is also 30% and 17-fold more capable than BA.1 and Delta, respectively, to escape current vaccines. Therefore, we project that Omicron BA.2 is on its path to becoming the next dominating variant. We forecast that like Omicron BA.1, BA.2 will also seriously compromise most existing mAbs, except for sotrovimab developed by GlaxoSmithKline.
Abstract of this paper is self-explanatory, and raise a point that many other papers already did, BA.2 has 32 mutations that are the same in BA.1, but 28 that are unique, as I previously covered, this is one of the reasons it makes BA.2 antigenically different, and under certain circumstances, it breaks through previous natural acquired immunity.
By using deep learning and complex mathematical model using to learn about all the shapes of the cell, the came up with the conclusion that BA. 2 will dominate as a variant and will break through all forms of “synthetic protection”. In my opinion, anything besides natural immunity should now be referred as synthetic protection, at least, this is what I will refer to from now on.
I am also not a big fan of deep learning, modelling papers, but they bear a lot of clues and further insights.
Nationwide Danish data in late December 2021 and early January 2022 indicate that Omicron BA.2 is inherently substantially more transmissible than BA.1 and capable of vaccine breakthrough. Israel reported a handful of cases of patients who were infected with original Omicron BA.1 strain and have reinfected with BA.2 in a short period. Although BA.2 did not cause worse illness than the original Omicron BA.1 strain, its reinfection is very alarming. It means the antibodies generated from the early Omicron BA.1 were evaded by the BA.2 strain. It is imperative to know whether BA.2 will become the next dominating strain to reinfect the world population.
Our model predicts that BA.2 is about 1.5 as contagious BA.2, which is the same as reported in an initial study
Vaccine breakthrough
Omicron BA.1 is well-known for its ability to escape current vaccines. Its 15 mutations at the RBD enable it to not only strengthen its infectivity by a stronger binding to human ACE2 but also create mismatches for most direct neutralization antibodies generated from vaccination or prior infection. Although
BA.1, BA.2, and BA.3 share 12 RBD mutations, BA.1 has 3 additional RBD mutations, BA.2 has 4 additional RBD mutations, and BA.3 has one mutation the same as that of BA.1’s additional ones and two mutations the same as those of BA.2’s additional ones
Experimental analysis of the variant vaccine-escape capability over the world’s populations is subject to many uncertainties.
The RBD mutations of the Delta variant cause 1.5 fold reduction in the neutralization capability. In the same setting, Omicron BA.1, BA.2, and BA.3 may lead to about 21, 27, and 18 fold increases in their vaccine-breakthrough capabilities. As such, BA.2 is about 30% more capable to escape existing vaccines than BA.1 and 17 times more than the Delta variant. Our prediction has a correlation coefficient of 0.9 with the experiment. With its highest infectivity and highest vaccine-escape potential, the Omicron BA.2 is set to take over the Omicron BA.1 in infecting the world population.
The authors go to great detail on how all the amino acid (AA from here on) changes and the impact they have, not only in the viral and infection dynamics, but everything else. I will refrain from citing it because it gets really complicated in about 30 seconds.
They state that the 15 AA changes in the RBD (Receptor Biding Domain) up the infectivity by a lot, and creates “enough differences” in the virus so the antibodies have trouble or not even neutralize the virus itself.
They extrapolate the mutations in the RBD, if compared to the advantage Delta gained, raise the increase of breakthrough infections by those folds (21, 27, 18, that is A LOT). BA. 2 in this scenario has a 30% more effectiveness to escape antibody response than BA. 1. Again, this is a lot.
One final addendum to this paragraph is to the small quoted text. I, personally, disagree with the authors in this matter. Yes, that analysis of antibody escape is subject to many uncertain variables, but you could do it, not for a scientific paper, but under a risk mitigation scenario, if you use a simplified Bayes model, or different methods, often interdisciplinary, of analysis.
This is exactly how I kept getting everything “right”, without “evidence”. The mountain of evidence was there, just not connected the way most are used. Plus all the signals.
Authors them go to talk about said AA changes in the RBD and how they impact treatment, which I won’t bother to cover, mAbs (monoclonal antibodies) are useful to treat moderate to severe patients, but I mentioned a couple papers before, and there are a few others, mAbs are also fueling viral evolution.
I will leave to the read is the following, in this post , I shared and commented a paper about 4 doses of inactivated vaccine and how it shifts the response away from the RBD. An argument could be made that the widespread use of monoclonals and non-neutralizing vaccines will create a big enough problem as the virus evolve.
Influenza A H1N1–mediated pre-existing immunity to SARS-CoV-2 predictsCOVID-19 outbreak dynamics
Susceptibility to SARS-CoV-2 infections is highly variable, ranging from asymptomatic and mild infections in most, to deadly outcome in few. Here, we present evidence that antibodies induced by currently circulating influenza A H1N1 (flu) strains cross react with the most critical receptor binding motif of the SARS-CoV-2 spike protein that interacts with the ACE2 receptor. About 58–5 68% of blood donors in Stockholm had detectable antibodies to this cross-reactive peptide, NGVEGF, and seasonal flu vaccination trended to enhance binding of inhibitory antibodies to SARS-CoV-2. This peptide also activated CD8 T cells in 20% of healthy subjects. Eleven additional CD8 T-cell peptides that cross-react with flu and SARS-CoV-2 were identified that potentially protect against SARS-CoV-2 in 40–71% of individuals, depending on their HLA type.
Authors argue for a new explanation on why the disease range from asymptomatic to mild in most people, and it is because the virus shares a peptide sequence with the H1N1 (with the N part of the flu). Previous infection with said flu strain, and harboring antibodies to the sequence NGVEGF, enhanced antibody binding to SARS-CoV-2 receptor binding motif. Said sequence also activated CD8 cells, and I covered here numerous time how CD8 T cell response is important to this virus (and many others).
They then explain viral and population dynamics and the spread of the virus, and how this flu strain hindering the spread, won’t bother covering here.
Hence, in some people, T cells trained to recognize unrelated pathogen peptides may protect against severe COVID-19 through cross-immunity (or molecular mimicry). However, as this virus can be transmitted by aerosols (22), it is unlikely that T cells protect against infection with SARS-CoV-2 on a population level. Instead, antibody protection is expected to be required.
I like how the authors raise the point of cross-immunity, mention molecular mimicry, which is something I covered before and give a lot of importance. In fact, while I didn’t delve further here on Substack, I believe much of the after damage the virus inflicts is via molecular mimicry. It has too many similar parts with other viruses, bacteria and fungi, which throws your immune system slightly to insanely out of whack. Their second point made me rage.
By now, with extensive clinical evidence, and scientific literature that T Cell responsive is one of the most critical aspects to protect you long term. Antibody fixation is what got us into this mess… I guess there is no other way to publish lately unless you insert dogmatic, bullshit science in your paper…
However, a method focusing on small 6-merpeptides to search for cross-reactive epitopes that are optimal for antibody binding identified a peptide in SARS-CoV-2, NGVEGF (Fig. 1A), that is identical to a peptide in the neuraminidase of two strains of influenza A H1N1 (swine flu): Nagasaki/07N005/2008 and Kyoto/07K520/2008.
Remarkably, this peptide was present in the most critical part of the receptor binding motif of the spike protein (amino acids (aa) N481 to F486, Fig. 1A) that interacts with the angiotensin converting enzyme 2 (ACE2) receptor
NGVKGF is present in SARS-CoV-2 variants from Brazil (gamma, P1), South Africa (beta, B.1.351, V 501Y.V2), and New York (iota, B.1.526) that carry an E484K mutation, and concerns have been raised that vaccines are less protective against viruses carrying this mutation. Thus, antibodies to NGVEGF/NGVKGF developed during a swine flu infection or after a seasonal flu vaccination may protect against SARS-CoV-2 infections.
By changing how they search for similar sequences in other virus, to epitopes (basically the top of the antigen that binds to your antibody, and initiates the immune response), they found out that it had a identical sequence to two strains of H1N1.
The sequence was present in the Brazilian, South African and Net York variants. Want some conspiracy ? There was an argument, back when said variants arose, that they were lad leaked. Dig deep and you might find your answer…
Since the prevalence or titers of NGVEGF-specific antibodies did not appear
to increase after SARS-CoV-2 infection, we speculate that NGVEGF is more immunogenic when present in neuraminidase (at a highly immunogenic site) than when present in the SARS-CoV-2 spike protein. Flu may also induce a more long-lasting antibody response than SARS-CoV-2. Since the majority of people have some NGVEGF-reactive antibodies, these new insights affect the interpretation of the role of NGVEGF-specific antibodies in SARS CoV-2 infected individuals, especially concerning their protective effects against variant viral strains containing the E484K, E484Q or the new E484A omicron mutation.
Authors state that NGVEFG specific antibodies do not appear to increase after SARS-CoV-2 infection, which is something to be expected, you are not being infected with the whole influenza virus, but just a (stitched IMO) peptide sequence.
Buckle up, it is about to get kind complex. Which we love it around here.
While antibodies may protect people from becoming infected, cytotoxic T cells are crucial to resolve life-threatening infections by killing virus-infected cells. In modeling analyses, we found that the NGVEGF peptide can be presented to CD8 T cells by some HLA class I molecules (HLA- A*33:01, HLA-A*68:01, HLA-A*31:01, HLA-A*11:01) found in about 22.2% of Scandinavian
Among a small group of highly capable geneticists, they talk among themselves how one of the major aspects of severity when infected with SARS-CoV-2 is your HLA type. Authors got interesting results.
We confirmed that B and T cells from healthy subjects recognize and respond to
NGVEGF peptides in vitro and that this reactivity was boosted in some people after seasonal flu vaccination (n = 20). The response was highly individual and differed for CD19, CD4, and CD8 T cells. Flu-vaccinated subjects had significantly more IFN-γ producing CD8 T cells that recognized the NGVEGF peptide (mean increase from 1.1% to 2.3%, p = 0.009) and B cells (mean increase from 1.9% to 3.5%, p = 0.003); IFN-γ producing CD4 T cells reactive to the NGVEGF peptide also trended higher after flu vaccination (mean increase from 1.6% to 2.0%, p = 0.0567. Interestingly, 7 of 20 (35%) individuals had a robust increase in the numbers of CD8 T cells reactive to NGVEGF (mean increase 4.3%); about 22% of Scandinavians are expected to have HLA types able to present this peptide efficiently to T cells.
Now we got to the good part… can readers tell, just by reading, what that would be ? The T Cell response, specially the type of it. IFN-γ CD8 cells, something that vaccinated individuals are completely lacking after vaccination, and even after infection most of the time. Another point of great interest is the following.
Flu infection and vaccination have something in common.
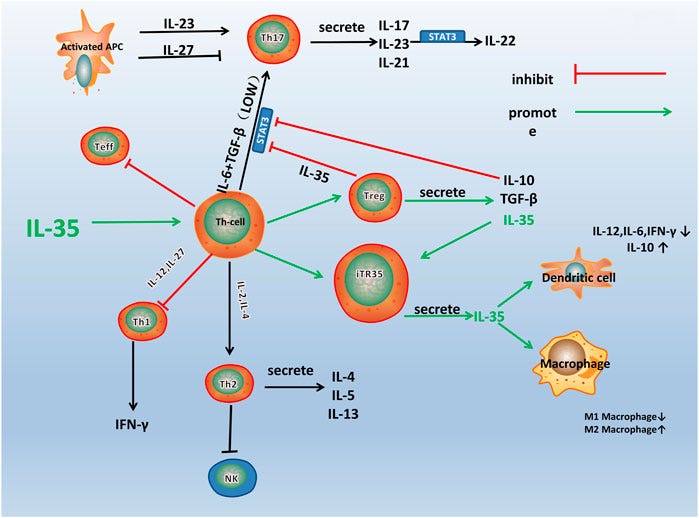
They elicit an Interleukin-35 response, do you know what IL-35 can do under specific immune dominance ? Stop the differentiation towards Th17, and the cell signalling involved. What a…coincidence…
Makes one wonder…really does… (yes, I mentioned this almost a year ago). Further reading for the curious.
A flu-mediated pre-immunity to SARS-CoV-2 may be less efficient and less sustainable after repeated flu vaccinations than after influenza A H1N1 infection that would elicit robust B- and T-cell immunity.
The flu vaccination recommendations and favorable HLA types might explain Sweden ́s lower incidence of severe COVID-19 disease in children under 10 years of age who had swine flu as their first influenza A H1N1 infection. So far, Sweden has not had high rates of severe infections among children requiring hospital care; however, multisystem inflammatory syndrome in children is twice as prevalent in Sweden as in the US. The syndrome develops 4–6 weeks after diagnosis of COVID- 19 and may not be related to the severity of SARS-CoV-2 infection.Flu vaccination strategies together with unfavorable HLA types with
lower capacity to present flu peptides to T cells may explain differences in susceptibility to SARS-CoV-2 infection and the risk of developing severe COVID-19 in different parts of the world.
Bold part, synthetic immunity is inferior to natural one, more news at 11. Otherwise, not only this bears wait to the HLA argument, but how SARS-CoV-2 structure and molecular mimicry play an important, complex role on its immunity, severity of infection, and most likely its after effects (setting off autoimmunity, clots, etc).
As a last comment to this paper, go to the post below and read the IRIS part. Tell me if, in some degree, the multisystem inflammatory syndrome doesn’t remind you of IRIS… hum… As for a conspiracy angle, I could imagine the vaccine companies and researchers finding out the overwhelming Th17 differentiation both in the severe infection, and vaccination, and trying to patch it up.
The House MD approach (one of my biggest medical influences, lol). Throw everything to the wall, see what sticks. The entire pandemic response was like this, too.
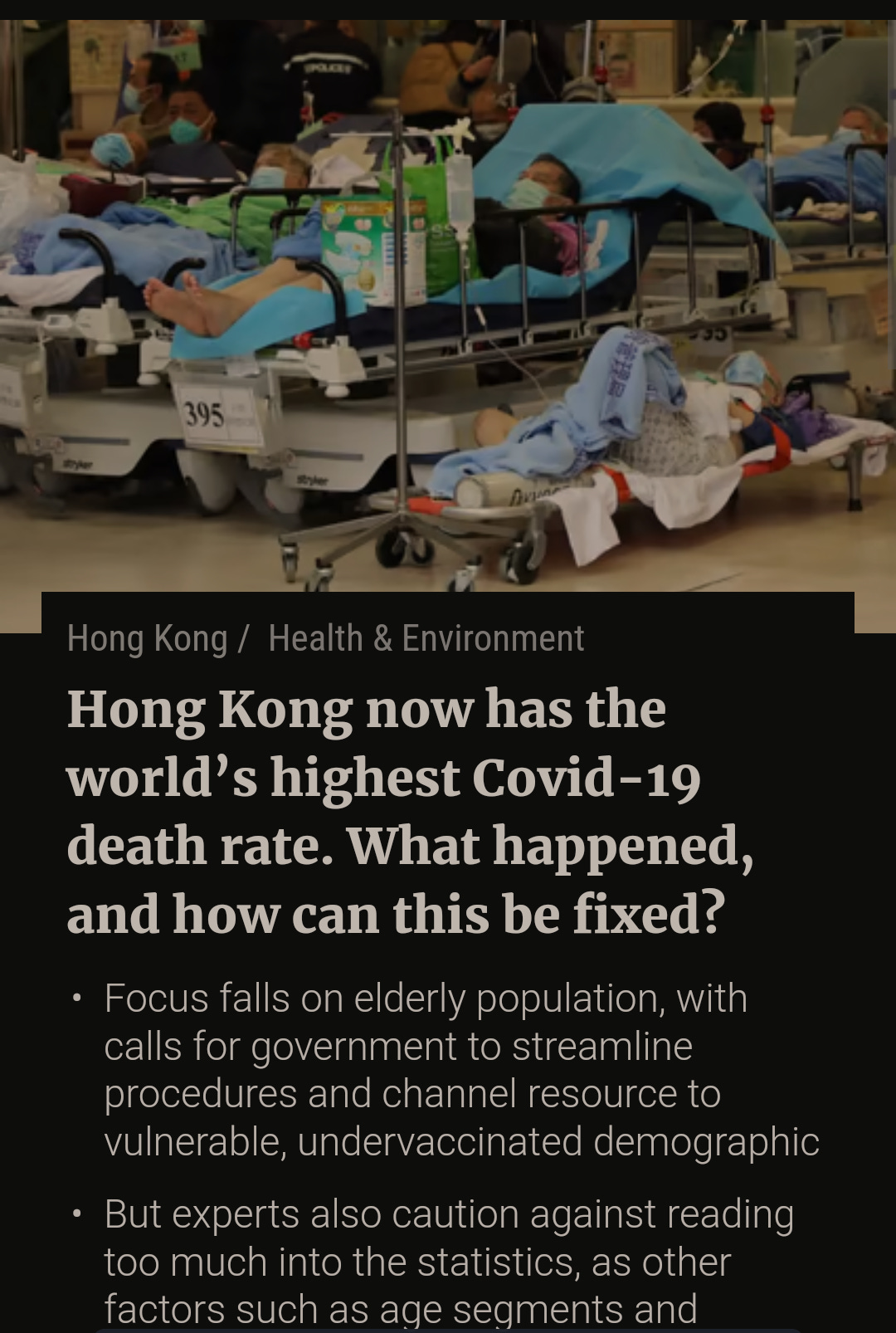
I commented about Hong Kong in this post. And I stand by my case for Reverse Marek.
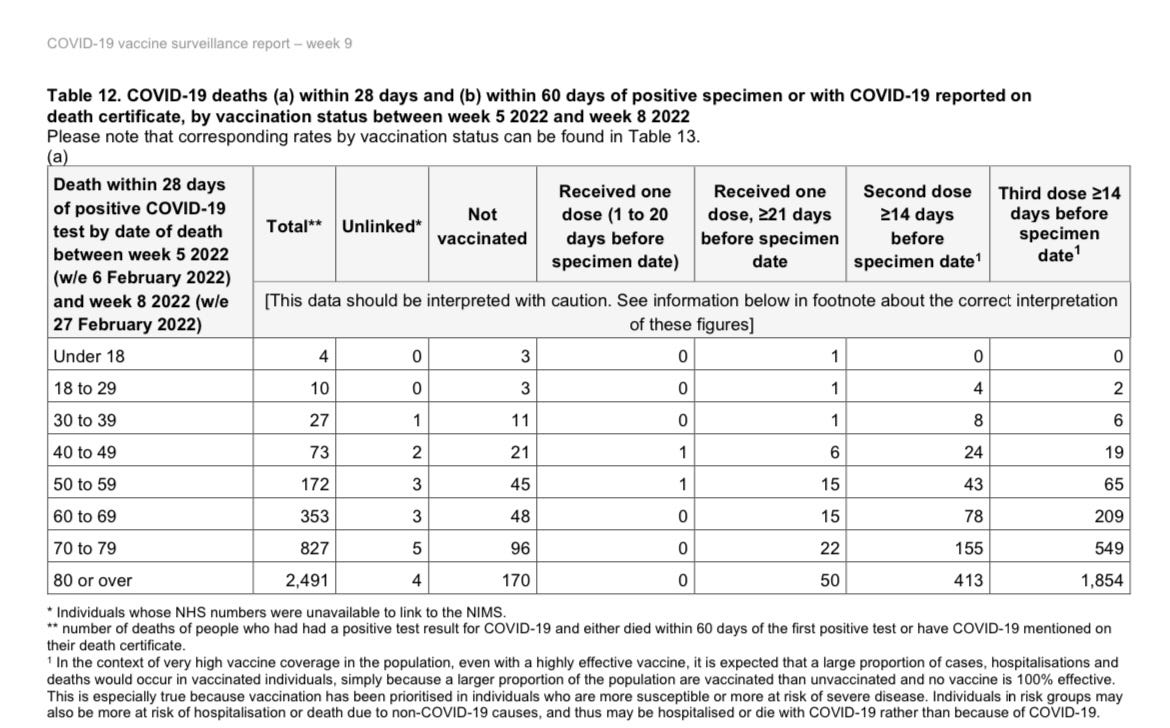
The data below is from the UK, Bereson already covered this, and probably others in Substack too. Most of the deaths are from vaccinated individuals now, and this is a trend that will keep growing in every highly vaccinated country.
As BA. 2, and the dysfunctional immune state the vaccinated find themselves, the death toll will increase. The vaccinated can NOT clean the virus, they don’t elicit a broad, and strong enough neutralizing response, which not only will aid viral evolution (further), but it will create a scenario of chronic infection.
If you enjoy or take value from my independent, interdisciplinary analysis, consider becoming a free or paying subscriber, my work, and autism is fully support by you. Sharing also helps me tremendously. Appreciate all supporters.